Article Text

Abstract
Background: A substantial proportion of patients with recurrent pneumonia do not have an apparent underlying condition, but they may have unknown defects in host defence mechanisms such as cough reflex.
Methods: Capsaicin cough sensitivity was measured in seven patients with recurrent pneumonia but no underlying condition. Recurrent pneumonia was defined as at least two episodes of pneumonia in 1 year, or three or more episodes at any time. After remission of pneumonia, 10 doubling concentrations of capsaicin (1.22–625 μM) were inhaled until five or more coughs were induced (cough threshold). Mucociliary clearance was assessed on the basis of nasal ciliary beat frequency and nasal clearance time. Twenty one age and sex matched healthy subjects were studied as controls.
Results: Each patient had 2–6 episodes of pneumonia. Most episodes developed in dependent lung segments, suggesting the involvement of silent aspiration. Log transformed cough threshold was significantly higher in patients than in controls (mean 2.37 M (95% CI 1.84 to 2.90) v 1.29 μM (95% CI 1.11 to 1.47); p<0.0001). The effect of pneumonia per se on cough reflex seemed unlikely since the cough threshold showed little change when re-examined after 3 months. The patients and controls did not differ with respect to the indices of mucociliary clearance.
Conclusions: Impaired cough reflex may be involved in the pathogenesis of recurrent pneumonia.
- recurrent pneumonia
- cough reflex
- mucociliary clearance
Statistics from Altmetric.com
Recurrent pneumonia is an important clinical problem.1,2 Various disorders may predispose patients to recurrent pneumonia, but a substantial proportion of patients with recurrent pneumonia do not have an apparent underlying condition.1,2 They may, however, possess unknown defects in host defence mechanisms.
Silent aspiration of pharyngeal secretions universally occurs during sleep, even in “healthy” individuals.3 The volume of aspirated material may contain substantial quantities of bacterial organisms3 which may lead to the development of pneumonia. Cough reflex, as well as mucociliary clearance, is assumed to play an essential role in the prevention of aspiration. However, studies of cough reflex as a defence mechanism are rare and mostly confined to patients with central nervous system disorders.4,5 The aim of this study was to verify the hypothesis that patients with recurrent pneumonia but no apparent underlying condition have impaired cough reflex.
METHODS
Subjects
Cough sensitivity to inhaled capsaicin and mucociliary function, assessed on the basis of nasal ciliary beat frequency and nasal clearance time, were evaluated in patients with community acquired recurrent pneumonia and healthy controls.
Patients were prospectively and consecutively recruited from those referred and admitted to the Chest Disease Research Institute, Kyoto University for treatment of pneumonia from 1993 to 1998. Seven patients (six men) of mean (SD) age 63 (14) years (range 43–83) met the entry criteria. All were well and led active daily lives except when they suffered from pneumonia. Four patients had never smoked cigarettes and three were ex-smokers who had quit smoking more than 2 years before the study. No patient had a deficiency in serum IgG, IgM, IgA titres or IgG subclass titres compared with published normal range. Pulmonary function of the patients was normal: vital capacity (VC) 99 (12)% (range 83–114), forced expiratory volume in 1 second (FEV1) 103 (16)% (range 85–118) of respective predicted values.
Recurrent pneumonia was defined as at least two episodes of pneumonia in 1 year, or three or more episodes at any time.6 Each episode was accompanied by pulmonary infiltrates and fever which responded to appropriate antibiotic treatment and resolved between episodes.6 None had any underlying respiratory illnesses such as bronchiectasis, emphysema or endobronchial tumours,1,2 confirmed by computed tomography of the chest and fibreoptic bronchoscopy in all patients. Patients with the following non-respiratory conditions were also excluded1,2,4–6: cardiac disease; immunocompromised state (diabetes mellitus, corticosteroid therapy, active malignancy, AIDS); predisposition to aspiration (central nervous system disorder,4,5 alcoholism, neuromuscular disease, postgastrectomy); or observed episodes of aspiration.4
Twenty one age and sex matched healthy subjects (18 men) of mean (SD) age 61 (15) years (range 41–79) with no previous history of pneumonia or other respiratory diseases who had never smoked formed the control group. None of the patients or controls were taking medication which might affect cough sensitivity, such as antitussives, narcotics, or ACE inhibitors.
Study design
Cough sensitivity was examined after pneumonia had responded to antibiotic treatment (median 16 days, range 10–21) after negative conversion of C reactive protein. Ten doubling concentrations of capsaicin solution (1.22–625 μM) were inhaled until five or more coughs were induced (cough threshold, C5).7 Each concentration of capsaicin was inhaled for 15 seconds during tidal breathing every 60 seconds.7 If five or more coughs did not occur at the highest concentration, C5 was arbitrarily set at 1250 μM. Cough sensitivity was re-examined after 12 weeks in six patients who did not have an additional episode of pneumonia during this period. The ciliary beat frequency of the nasal ciliated epithelium, obtained with a cytology brush, was measured using a photometric technique8 and the results were expressed as beats per minute (Hz). Nasal clearance time was measured with the use of saccharin.9 The time from saccharin particle placement on the inferior turbinate until the subjects reported the first sensation of a sweet taste was measured in minutes. Location of pneumonia in the lung was determined on the basis of chest radiographic or computed tomographic findings.
The study protocol was approved by the ethics committee of our institution and written informed consent was obtained from all subjects.
Data are expressed as mean (SD) except where specified otherwise. The unpaired t test was used to compare patients with controls. A p value of <0.05 was considered significant.
RESULTS
Each patient had 2–6 episodes of pneumonia (total 22 episodes). Of 20 episodes with identifiable locations, 19 developed in dependent lung segments.
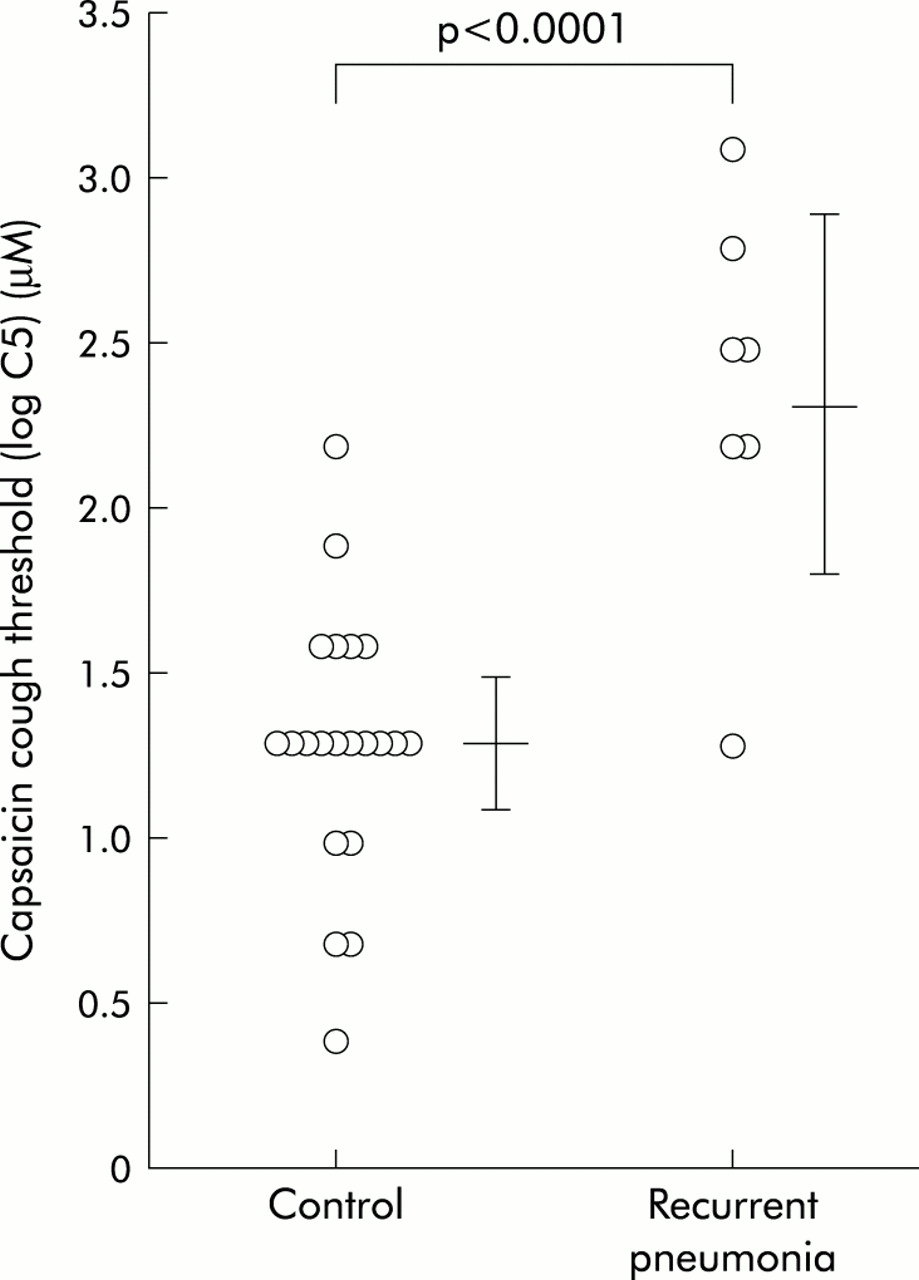
Log C5 was significantly higher in patients than in control subjects (mean 2.37 μM (95% CI 1.84 to 2.90) v 1.29 μM (95% CI 1.11 to 1.47); p<0.0001, fig 1). Cough sensitivity, re-examined in six patients, did not change (n=3), decreased (n=2), or increased (n=1) by only 1 doubling concentration of capsaicin. The patients and controls did not differ with respect to ciliary beat frequency (12.0 (0.6) v 12.3 (1.1) Hz) or nasal clearance time (7.3 (2.4) min v 7.2 (2.2) min) (p>0.1 for both).

{kind=link}
Capsaicin cough threshold (log C5) in patients with recurrent pneumonia and control subjects. Bars indicate mean (95% CI).
DISCUSSION
This study shows, for the first time to our knowledge, that cough sensitivity is significantly attenuated in patients with recurrent pneumonia who lack apparent underlying illnesses or a predisposition to aspiration. Mucociliary function did not differ between the patients and controls. Immunoglobulin deficiencies, a potential cause of recurrent pneumonia,1 were not found in the patients. Almost all episodes of pneumonia developed in dependent lung segments, suggesting the involvement of silent aspiration. These findings suggest that a lowered cough reflex in patients impairs defence mechanisms against aspiration, leading to the development of recurrent pneumonia.
The cough reflex is reportedly less sensitive in men than in women. In addition, aging may or may not attenuate cough reflex and mucociliary function. We believe these effects were negligible in our study because the patients and controls were matched for sex and age. The effect of pneumonia per se on cough reflex also seems unlikely, since the cough threshold showed little change in patients re-examined after 3 months.
In conclusion, impaired cough reflex may be involved in the pathogenesis of recurrent pneumonia. Prophylactic protussive treatment might be indicated in patients with recurrent pneumonia who have lowered cough sensitivity. The effectiveness of such treatment, however, must be confirmed by future studies in larger numbers of patients. Mechanisms involved in the impairment of cough reflex, including genetic factors,10 should also be investigated.
Acknowledgments
This study was supported in part by a Grant-in-Aid for Scientific Research from the Ministry of Education, Science, and Culture (13670599) of the Japanese government.