Article Text

Abstract
Background: A review was undertaken of the clinical features and results of diagnostic tests in non-HIV infected patients who developed granulomatous Pneumocystis carinii pneumonia (PCP).
Methods: A retrospective review was performed of the charts and radiographs of patients with a granulomatous reaction to P carinii identified from computerised pathology records at Memorial Sloan Kettering Cancer Center, a university affiliated tertiary care hospital.
Results: Three cases were identified; the incidence of granulomatous PCP was 3%. All patients had risk factors for PCP and had received high dose corticosteroids which had been stopped. Two patients had received chemotherapy. Presentation was insidious with only mild symptoms; only one patient had fever. Chest radiographs showed a reticulonodular pattern. Bronchoscopy was negative for PCP in all cases and open lung biopsy was necessary.
Conclusion: A granulomatous pathological reaction to PCP occurs rarely in patients with malignancy. In these cases the clinical presentation may be atypical and bronchoscopy can be non-diagnostic.
- pneumonia
- granuloma
- malignancy
Statistics from Altmetric.com
Pneumocystis carinii causes serious pneumonia in immunocompromised patients. It occurs in those who are infected with the human immune deficiency virus (HIV), following organ transplantation, in patients with malignancy (particularly those receiving corticosteroids), and in others on immunosuppressive drugs for a variety of underlying diseases. Classic pathological findings of P carinii pneumonia (PCP) consist of a characteristic foamy intra-alveolar eosinophilic exudate which contains trophozoites and cysts of the organism, surfactant, fibrin, and cellular debris. There may also be a mild interstitial infiltrate. A granulomatous histological response to P carinii is unusual but has been reported in a few patients with HIV infection,1,2 as well as rarely in other immunocompromised patients.3,4 In these cases, biopsy specimens show palisades of epithelioid cells forming granulomas with the organisms of PCP found within them rather than free in the alveolar space. Necrosis is often present. The reason for the development of a granulomatous reaction in some patients with PCP is speculative but has been postulated to be related to the state of the host's defence system.
The impact of the development of a granulomatous pathological picture on the clinical presentation and diagnosis of PCP is not well described, particularly in non-HIV infected patients with cancer. In this paper we report our experience with cases of PCP in patients with cancer in whom a granulomatous reaction occurred, and identify the clinical presentation and diagnostic features in this subset of patients.
METHODS
Cases of a granulomatous reaction to P carinii were identified by searching the computerised pathology records and discharge summaries from 1986 to 1998 at Memorial Sloan-Kettering Cancer Center. Patients infected with HIV were excluded. The charts, radiographs, and pathological specimens of these patients were reviewed.
RESULTS
Incidence
From 1986 to 1998 three cases of granulomatous PCP in non-HIV infected patients were identified. Approximately 11 case of PCP are seen yearly at Memorial Sloan-Kettering Cancer Center in patients who are HIV negative.5 The average incidence of granulomatous PCP among all cases of PCP was therefore 3%.
Patients
Details of patient characteristics are given in table 1. There were two women and one man and their ages ranged from 17 to 56 years. Two patients had haematological malignancies and one had a primary brain tumour. All had received high doses of corticosteroids but the steroids had been tapered off before the diagnosis of PCP in all cases. Steroids had been stopped from 2 weeks to 2 months before presentation with PCP. Two of the patients had received chemotherapy as well as steroids; one had received mechlorethamine, vinblastine, procarbazine, thiotepa, doxorubicin, bleomycin, vincristine sulfate and prednisone and the other had received fludarabine for three cycles followed by two cycles of cyclophosphamide, doxorubicin, vincristine sulfate and prednisone. One patient had received aerosolised pentamidine while on corticosteroids. The other patients had not received prophylaxis for PCP.
Characteristics of patients
Presentation
All patients had only mild symptoms of cough or dyspnoea, with fever in one case. Abnormal pulmonary function test results in one asymptomatic patient led to radiography which revealed infiltrates. On questioning, this patient admitted to very mild respiratory symptoms but had not spontaneously complained of these symptoms. The serum LDH level was slightly raised in one case but was normal in the others. The chest radiographs, however, showed impressive reticulonodular infiltrates in all cases. Pulmonary function tests showed a decreased transfer factor in all three patients with an increased alveolar-arterial gradient and significant exercise desaturation (table 1).
Diagnosis
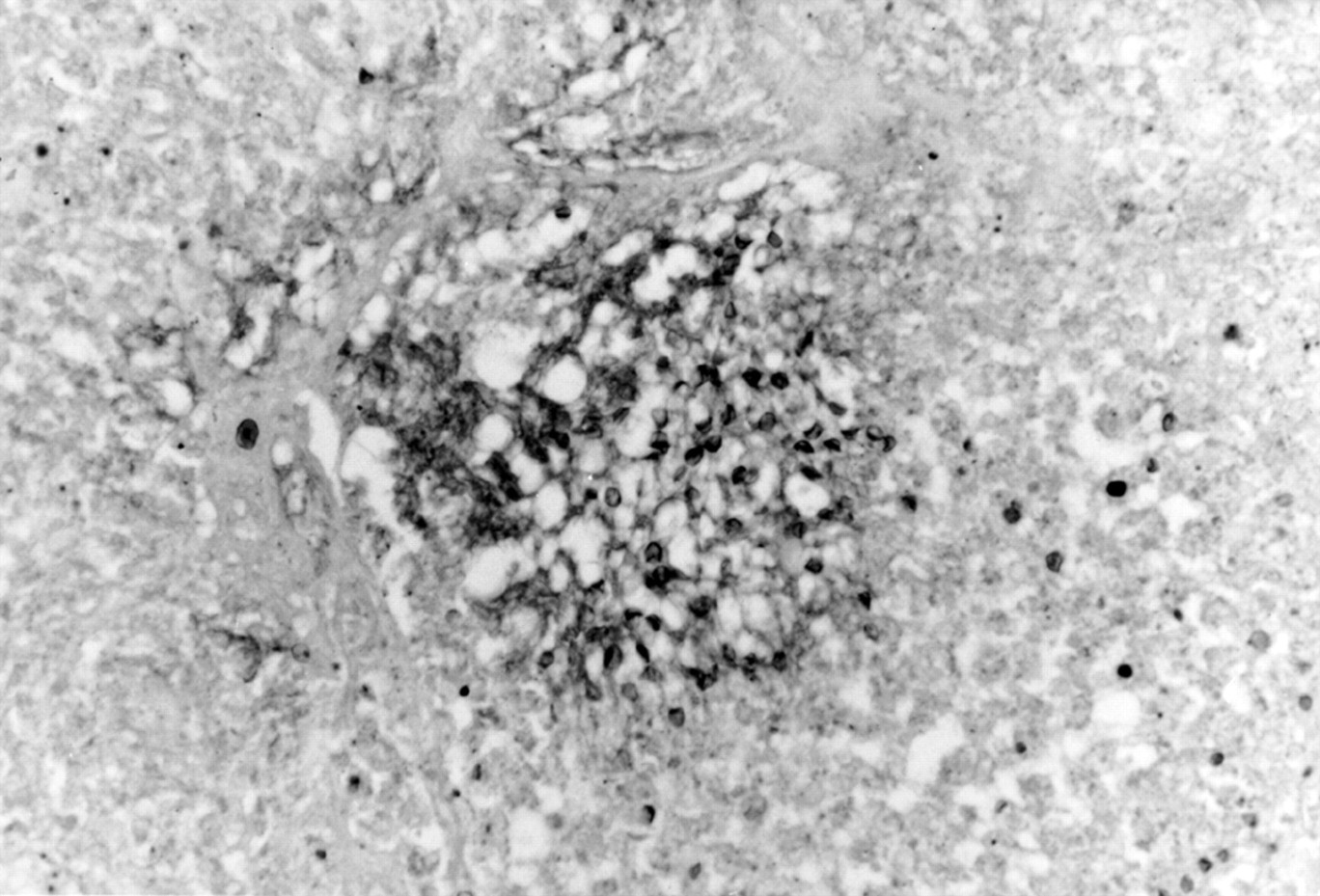
All patients underwent bronchoscopy with bronchoalveolar lavage (BAL); two patients also had transbronchial biopsies. All specimens were negative for PCP. On open lung biopsy, a necrotising granulomatous reaction was found in each case and special stains confirmed the presence of PCP within the granuloma (figs 1 and 2).

Haematoxylin and eosin stain of an open lung biopsy specimen showing necrotising granuloma.
{kind=link}
{kind=link}
Silver methenamine stain showing the cysts of Pneumocystis carinii in the granuloma.
Treatment and outcome
Two patients were treated with sulfamethoxazole and trimethoprim (TMP-SMZ) without corticosteroids with resolution of the pneumonia. In one patient who was started empirically on TMP-SMZ after bronchoscopy the condition worsened. She was placed on pentamidine with corticosteroids after confirmation of PCP by open lung biopsy and subsequently completely recovered.
DISCUSSION
The development of a granulomatous histological reaction in PCP is unusual, occurring in only 3% of the cases of PCP identified in patients with malignancy at our institution. All of these patients had expected risk factors for development of PCP but they had atypical clinical features. The presentation was insidious with very minimal symptoms and the radiographs showed a reticulonodular pattern rather than the expected interstitial-alveolar infiltrates. This pattern is more characteristic of HIV infected patients than of those with malignancy where the presentation is often subacute to fulminant and dyspnoea is the prominent symptom.6 In addition, an increased serum level of LDH, which is a sensitive marker for the presence of PCP, was not found in our patients.7 The LDH level was normal or only slightly raised.
The unexpected finding of most clinical significance was the non-diagnostic bronchoscopy in all cases, even in the two cases from whom transbronchial biopsy specimens were taken in addition to BAL. Although the diagnostic yield of BAL in non-HIV infected patients is lower than in HIV patients, the yield of transbronchial biopsy combined with BAL is believed to be very high in this setting.8 Thus, the negative findings of PCP on bronchoscopy combined with the atypical clinical features led to consideration of other diagnoses and a delay in treatment. Kester et al also reported an inability to make a diagnosis of granulomatous PCP by bronchoscopy in two patients with granulomatous PCP and lymphoma.4 The reason for the insensitivity of bronchoscopy is unclear, but it may be that fewer organisms are present with a granulomatous pathological reaction or, alternatively, that the presence of the organism inside the granuloma rather than free in the alveoli contributes to the lower diagnostic yield, particularly with BAL.
The presence of a low transfer factor on lung function testing and an increased alveolar-arterial gradient, as expected with PCP, remained helpful in confirming the presence of a significant diffuse pulmonary process. Unfortunately, these findings are non-specific and do not distinguish PCP from other infectious or non-infectious entities.
The factors that have led to the development of granulomatous histological findings in some patients are unknown. The role of corticosteroids in the development of PCP in the non-HIV infected patient is complex. While most cancer patients who develop PCP have received corticosteroids,5 suggesting that this drug leads to the impairment in immunity that allows PCP to develop, clinically overt pneumonia has often been noted as the corticosteroid dose is being tapered.9 It is assumed that the tapering of steroids unleashes an inflammatory response to the infection that has developed. The relationship of corticosteroid dose to symptoms of PCP is also supported by the finding that the use of adjunctive corticosteroids in addition to antibiotics in the treatment of life threatening PCP in patients with AIDS has led to decreased symptoms and improved survival.10 The role of increasing or restarting steroids in the non-HIV infected patient is not as clearly defined, but many clinicians in this setting will not taper steroids further or consider increasing the dose during the acute pneumonia episode. It is notable that all three of our patients and one previously described by Kester et al4 with granulomatous PCP had been tapered off steroids before their presentation. This may have allowed a granulomatous response to occur. This particular combination of infection with an intense granulomatous response led to the development of reticulonodular infiltrates and significant pulmonary function test abnormalities, even though the acute clinical symptoms of pneumonia were absent or not apparent. The presentation of PCP in a given individual is therefore likely to depend on a number of factors—including the number of organisms, type and rapidity of development of host response, and perhaps the length of time infection has been present. Interestingly, in case 3 the addition of corticosteroids appeared to be important in patient improvement.
An alternative explanation for the development of granulomatous changes may be related to the genetic diversity among strains of P carinii. Different populations of P carinii express different major surface glycoproteins (MSG). Since MSG binds to fibronectin receptors of type I epithelial cells, macrophage mannose receptors and alveolar surfactant proteins, it has been postulated that these changes in these highly immunogenic substances might alter the histological response of the host to P carinii.2 A granulomatous response may be more likely with some strains of PCP than with others, and this may be responsible for some cases of granulomatous PCP.
In summary, we found that a small percentage of patients with malignancy who develop PCP have a granulomatous reaction to the organism. This occurs in those with classic risk factors for PCP, but an atypical clinical picture is found which is characterised by an insidious clinical presentation with minimal symptoms and a reticulonodular pattern on the radiograph. The serum LDH level may not be raised and a negative bronchoscopic examination is likely. In patients with malignancy in whom granulomatous PCP is a consideration, open lung biopsy specimens may be necessary for diagnosis and a negative bronchoscopic result should not preclude the entity.