Article Text

Abstract
Airway inflammation with eosinophils is now reported to occur not only in asthma but in other airway diseases such as cough variant asthma, chronic cough, atopic cough, episodic symptoms without asthma, allergic rhinitis, and COPD. Although the prevalence of eosinophilic bronchitis (EB) is less than in asthma, the causes, mechanisms and treatment of EB in these conditions appears to be similar to asthma where allergen induced IL-5 secretion and symptoms are readily responsive to inhaled corticosteroids. The prognosis of EB without asthma is not known but it may be a precursor for asthma and, if so, recognition of this syndrome may permit effective treatment and reduction in the rising prevalence of asthma. Induced sputum analysis allows recognition of EB in clinical practice. The place of the asthma treatment paradigm with early and sustained corticosteroid treatment needs to be defined in EB without asthma. Airway wall remodelling can occur in rhinitis, COPD, and cough variant asthma with EB. The mechanisms and long term implications of this complication in EB without asthma need to be clarified.
- eosinophilic bronchitis
- asthma
- chronic cough
- chronic obstructive pulmonary disease
Statistics from Altmetric.com
Soon after Ehrlich described the eosinophil as an entity at the end of the 19th century, the presence of eosinophils in sputum was recognised as a characteristic feature of bronchial asthma.1 Since that time the spectrum of disorders characterised by eosinophilic airway inflammation has broadened. Eosinophilic bronchitis (EB) is now known to be a feature not only of bronchial asthma, but also of cough variant asthma, atopic cough, isolated chronic cough, respiratory symptoms without asthma, allergic rhinitis, and chronic obstructive pulmonary disease (COPD). EB has an established place in asthma where it contributes to airway hyperresponsiveness (AHR), asthma symptoms, and airway remodelling. Anti-inflammatory agents such as inhaled corticosteroids are used successfully to treat EB in asthma.2,3 Inhaled corticosteroids are introduced early in the course of the disease and are continued during asymptomatic periods. The implications of eosinophilic airway inflammation in disorders other than asthma and the potential role of the asthma treatment paradigm in those disorders with EB is the subject of this review.
DEFINITIONS
Eosinophilic bronchitis
Eosinophils are typically absent in sputum samples from normal subjects. The main cell seen is the macrophage, followed by a smaller proportion of neutrophils. The upper normal limit of sputum eosinophils in adults and children is 2.5% or less of cells.4–,6 These studies included people with allergic rhinitis and it is possible that the upper limit of normal for sputum eosinophils is, in fact, less than this. For example, Rytila et al found the upper limit to be 0.7%.7 For the purposes of this review, EB is defined as sputum eosinophilia of >2.5% in either spontaneous or induced sputum samples where the cellular differential is comparable.
Asthma
Asthma is defined as episodic respiratory symptoms occurring in association with variable airflow obstruction which may be demonstrated by bronchodilator responsiveness, increased diurnal variability of peak expiratory flow (PEF), or the demonstration of AHR.
Episodic respiratory symptoms without asthma
Episodic cough, wheeze, or dyspnoea occurring with normal forced expiratory volume in 1 second (FEV1), ratio of FEV1 to vital capacity (VC) of >70%, and no evidence of variable airflow obstruction.7
COPD
COPD represents a persistent reduction in FEV1 below 80% predicted, with a reduction in the FEV1/VC ratio below 70% after bronchodilator treatment.
MECHANISMS
Interleukin (IL)-5 is a key cytokine associated with the development of eosinophilia in various tissue sites in the body. IL-5 promotes the growth and differentiation of eosinophil precursors, prolongs their lifespan in tissue by inhibition of apoptosis, and can activate tissue eosinophils.8 Gene expression for IL-5 is increased in asthma.9 The consequences of this are eicosanoid activation, particularly the production of potent spasmogens such as leukotrienes C4, D4, E4 from eosinophils.10 EB in chronic cough has a similar pathogenesis to asthma with increased IL-5 gene expression9 and increased eicosanoid production.10 In COPD with bronchial eosinophilia there is also increased IL-5 expression.11 The cytokines responsible for EB occurring in association with allergic rhinitis have not been reported.
The mechanisms of EB in asthma are well defined, and studies indicate that the same mechanisms operate in COPD and chronic cough to cause EB. It is likely that other mediators also contribute to the pathogenesis of EB. For example, the chemokines eotaxin (I, II) and RANTES (regulated and activated, normal T cells expressed and secreted) are potent eosinophil chemoattractants that could play a role in EB. Cytokines and enzymes such as the matrix metalloproteinases that participate in tissue remodelling are also increased during eosinophilic airway inflammation. The subepithelial fibrosis that characterises asthma is one manifestation of tissue remodelling that is also reported to occur in allergic rhinitis with EB.12 Through these mechanisms, chronic eosinophilic inflammation could lead to permanent structural changes in the airway and be responsible for fixed airflow obstruction. The place of airway remodelling in non-asthmatic EB is not clearly defined.
Changes in eosinophilic airway inflammation are a well established cause of increased airway responsiveness in asthma. Airway responsiveness is also modified by eosinophilic inflammation, even when this is in the non-asthmatic range.13 For example, exposure to occupational sensitisers worsens airway responsiveness and airway inflammation in both the “asthmatic” and “non-asthmatic” ranges of airway responsiveness. Similarly, corticosteroid treatment reduces eosinophilic inflammation and improves airway responsiveness in both the asthmatic2,3 and non-asthmatic range.14 These data suggest that EB is only one of several determinants of AHR. Other important determinants include airway wall remodelling (increased smooth muscle mass and/or contractility, subepithelial fibrosis). Consequently, EB cannot be equated with AHR but is an important modifier of the degree of airway responsiveness.
CAUSES
Airway inflammation with eosinophils can be caused by exposure to allergens and occupational sensitisers. The triggers that cause EB without asthma are similar to the triggers of EB in asthma. Exposure to allergens,15–,18 occupational chemicals,19 and drugs20 are all reported to cause EB with cough. Some patients with chronic cough and EB have associated gastro-oesophageal reflux (GOR), raising the possibility that this may also induce eosinophilic airway inflammation.21 It is interesting to note that the presence of eosinophilic oesophagitis is a feature of GOR,22 and that neuropeptide release can promote tissue eosinophilia. This is a potential mechanism of EB caused by GOR.23 Viral infection is another potent cause of asthma exacerbation and cough that is associated with eosinophil recruitment to the lower airway.24
TREATMENT
EB responds well to anti-inflammatory treatment with inhaled corticosteroids. This beneficial treatment response is seen in asthma with EB, chronic cough with EB,14,25 atopic cough,26 cough variant asthma,27,28 EB with episodic respiratory symptoms but without asthma,7 and COPD with EB.29 Similarly, when eosinophils are not increased, corticosteroids have little benefit in chronic cough29,30 and COPD.29,31
CLINICAL PRESENTATIONS OF EB
Eosinophilic bronchitis in asthma
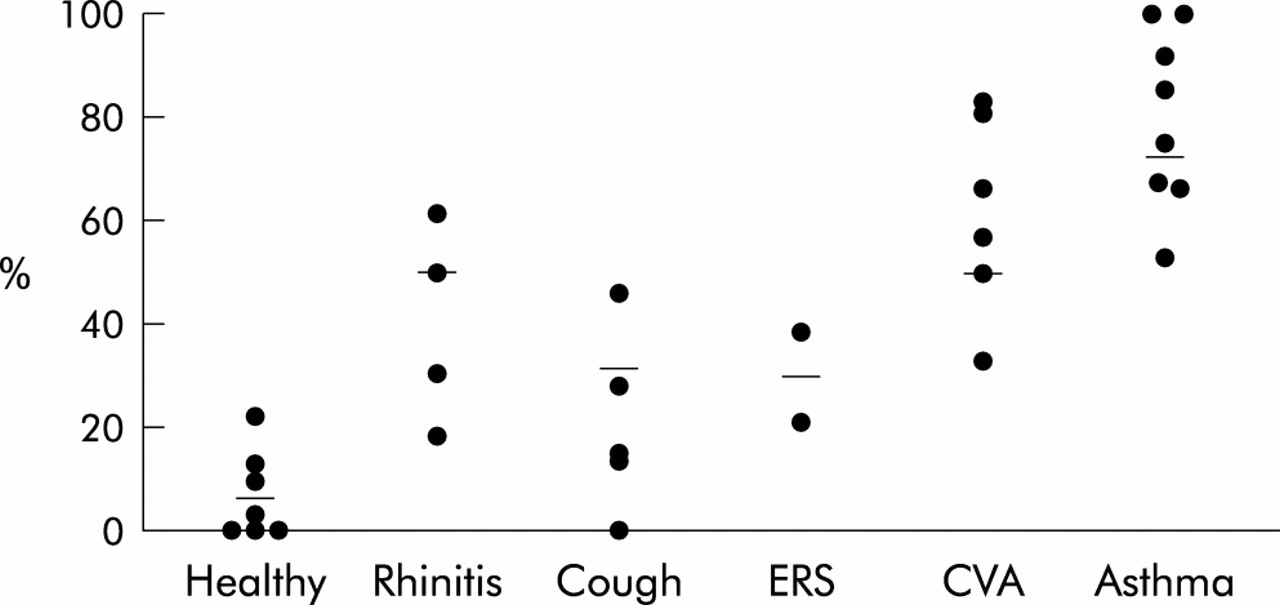
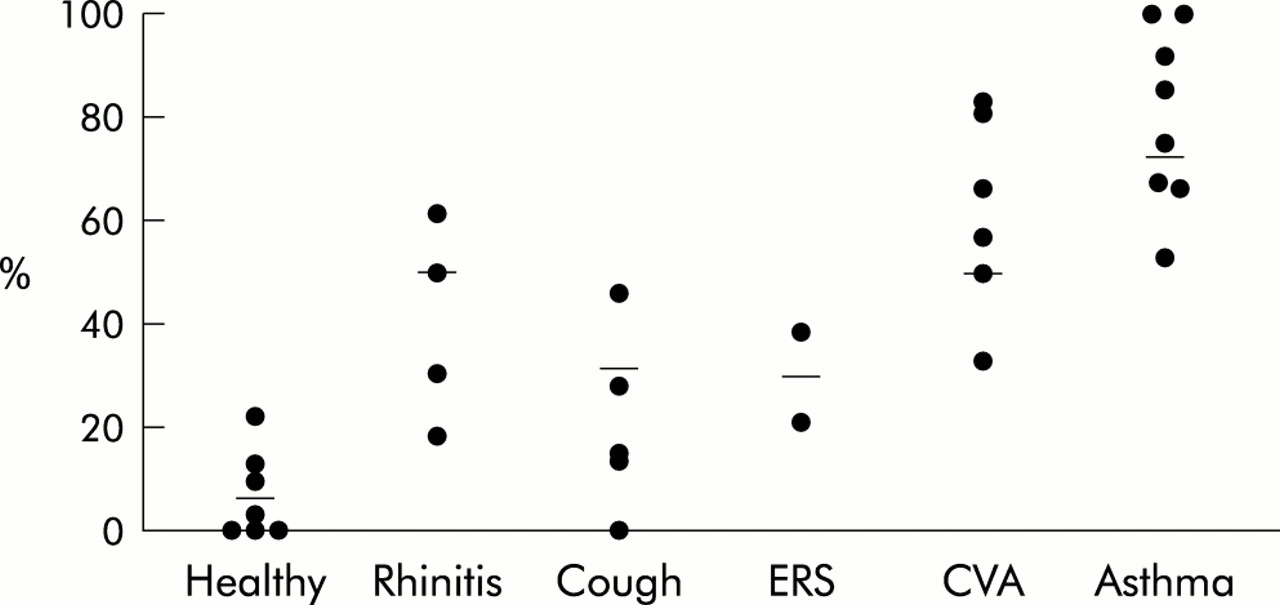
Eosinophilic bronchitis is a key feature of asthma where it forms part of the current definition32 and is believed to be responsible for AHR and asthma symptoms. EB is not a universal feature of asthma, however. The prevalence of EB in asthma ranges from 66% to 100% (table 1⇓, fig 1⇓). Eosinophilic bronchitis may be absent during exacerbations of asthma33,34 and also in stable disease.35,36
Prevalence and consequences of eosinophilic bronchitis in different clinical syndromes
{kind=link}
Prevalence of eosinophilic bronchitis (sputum eosinophils >2.5% or BAL eosinophils >1%) in published reports. ERS = episodic respiratory symptoms without asthma; CVA = cough variant asthma.
In asthma EB is a determinant of severity, increases during exacerbations of the disease, and is the focus of preventive treatment.32 Eosinophilia is one of several risk factors for increased mortality in asthma,37 with a 7.4 fold increase in the risk of death from asthma if blood levels of eosinophils are raised. The development of airway wall remodelling is a characteristic feature of asthma that may result from chronic eosinophilic inflammation, so the focus of asthma treatment is directed at controlling eosinophilic airway inflammation. Inhaled corticosteroids are administered on a daily basis and generally for long periods in order to suppress symptoms and exacerbations. Increasingly, the trends in treatment are to introduce corticosteroids earlier in the course of the disease and to continue treatment during asymptomatic periods to prevent the adverse effects of eosinophilic airway inflammation—namely, exacerbations and remodelling.
Eosinophilic bronchitis in allergic rhinitis
Patients with seasonal allergic rhinitis and atopic subjects without asthma may have EB demonstrated either by sputum analysis38–,41 or in bronchial biopsy samples.12 Approximately 50% of subjects with allergic rhinitis have EB (table 1⇑, fig 1⇑); the level of EB can be similar to that seen in asthma and correlates with the degree of airway responsiveness.42 Asthma symptoms are typically absent, although cough can develop during the pollen season in some patients.43 EB in seasonal allergic rhinitis is more common when patients are studied during a period of allergen exposure, indicating that allergen exposure is a trigger of lower airway eosinophilia in patients with allergic rhinitis without asthma.44,45 Similarly, nasal allergen provocation induces lower airway eosinophilia and adhesion molecule expression in subjects with allergic rhinitis without asthma.44 Histological characteristics of tissue remodelling, such as increased thickness of the reticular basement membrane, can also occur in rhinitis.12 Allergic rhinitis is a risk factor for subsequent asthma,46 especially after intense allergen exposure such as thunderstorm asthma.47
Cough variant asthma
Cough variant asthma (CVA) is characterised by eosinophilia in sputum,48–,51 bronchoalveolar lavage (BAL) fluid,21,52 and in bronchial biopsy specimens.52,53 Up to 50% of patients with CVA have EB (table 1⇑, fig 1⇑), and the degree of eosinophilia is similar to asthma. In addition, there can be thickening of the subepithelial basement membrane, a feature of airway wall remodelling.53 The degree of remodelling is less than in classical asthma and raises the possibility that eosinophilic inflammation in CVA may be a precursor to the development of asthma. CVA progresses to typical asthma in 17–37% of cases.54–,57
Eosinophilic bronchitis in chronic cough
Isolated chronic cough is a common clinical problem. EB may occur in patients with chronic cough who are subsequently diagnosed as having CVA, EB without asthma,14 or atopic cough.15 EB without asthma was described by Gibson et al in 198958 and is responsible for about 12% of cases of isolated chronic cough in tertiary referral clinics.49,59 These patients typically respond to inhaled and/or oral corticosteroids with suppression of daily coughing, of sputum eosinophilia, and of cough reflex to inhaled capsaicin.14,25 Interestingly, although airway responsiveness is in the normal range, it improves further with corticosteroid treatment.14
Atopic cough was described by Fujimura et al in 1992.60 Over 80% of cases have airway eosinophilia demonstrated either by bronchial biopsy specimens15 or sputum eosinophilia.48 Treatment with corticosteroids or antihistamines is effective. It appears that there is considerable overlap between the atopic cough described by Fujimura et al and EB without asthma as described by Gibson and others.61 Atopic cough is reported to be more prevalent in patients with chronic cough in Japan because of the corresponding low prevalence of cough associated with GOR and postnasal drip which are common causes of cough in western countries.21,49,59
Some correspondents have suggested that chronic cough with EB or atopic cough should be considered a form of asthma.62,63 These patients do not meet the current definition of asthma since they have normal airway responses to methacholine, histamine, and adenosine,14,49 they fail to improve with bronchodilators, and diurnal peak flow variability is normal.15,49,60 The relation between cough with EB and asthma is nevertheless important for several reasons:
Does cough with EB progress to asthma?
Does cough with EB cause airway remodelling?
Does cough with EB cause chronic airway obstruction? A single case report suggests this can occur.64
How should cough with EB be treated? Either until symptoms are suppressed or continuously and early as in asthma?
There is also an important issue of diagnosing cough with EB. Typically, cough is managed using the anatomical/diagnostic protocol (ADP) of Irwin.65 This does not allow for recognition of EB and this omission is seen by some as a limitation of this approach to chronic cough.59,63,66 Clinical features, long term outcome, and characteristics of exacerbations in EB with cough are poorly described.
Episodic respiratory symptoms without asthma
Patients presenting with episodic respiratory symptoms of cough, wheeze, chest tightness, dyspnoea, and sputum production but whose lung function measurements do not fulfil the criteria for asthma are often left without a diagnosis and without effective treatment.7 Up to one third of children develop clinical asthma over a 2 year period.67 EB is responsible for episodic respiratory symptoms without asthma in 21%68 to 38%7 of cases (table 1⇑, fig 1⇑). Bronchodilator response, PEF variability, and airway responsiveness to histamine or 4.5% saline are normal.7,68 These patients respond well to inhaled beclomethasone, but up to 13% may progress to develop asthma over a 1 year period.7
The clinical course and treatment requirements for these patients are not well defined. The high incidence of subsequent asthma in patients with EB without asthma suggests that this condition may be a precursor of subsequent asthma. The same issues arise for EB with respiratory symptoms as for cough.
Eosinophilic bronchitis and COPD
In addition to the typical IL-8 mediated neutrophil influx,69 some patients with COPD have eosinophilic inflammation detected in sputum, bronchial washings, BAL fluid, and bronchial biopsy specimens (table 1⇑).30,31,70–,73 Eosinophilic inflammation in COPD is associated with the degree of airflow obstruction70,72 and mortality.74 Airway remodelling is also evident in these patients, with subepithelial fibrosis being present and greater in patients with BAL eosinophilia who respond to corticosteroids.75,76
COPD can develop in patients who do not smoke. The mechanisms of chronic airflow obstruction in these patients are poorly characterised, but it is important to note that EB without asthma has progressed to chronic airflow obstruction in the absence of smoking.64 This raises the possibility that, just as in chronic asthma, chronic airflow obstruction may develop as a consequence of EB without asthma.
EOSINOPHILIC BRONCHITIS AND THE RISING ASTHMA PREVALENCE
The prevalence of asthma is increasing in western countries, predominantly in atopic subjects. There are increases in the prevalence of wheeze with AHR as well as wheeze without AHR. The conditions that precede the development of asthma are not well defined, but may represent an opportunity to intervene and reduce the rise in asthma prevalence. Cough variant asthma with EB may be a precursor of typical asthma with wheeze, and allergic rhinitis with EB may be a precursor for cough with EB, and also for episodic respiratory symptoms without AHR.
Much work is being directed at interventions in infancy to prevent the development of atopic disease. Another approach could be to prevent the development of symptomatic asthma by targeting EB without asthma. If EB is a precursor for asthma, then intervention at this stage could reduce the rising prevalence of asthma. Since cough is an early feature of EB, the recognition and effective treatment of cough with EB may reduce asthma prevalence.
SIGNIFICANCE OF EOSINOPHILIC BRONCHITIS WITHOUT ASTHMA
The studies reviewed establish that EB occurs not only in asthma, but also in chronic cough, COPD, and allergic rhinitis. The mechanisms and causal factors that operate in EB without asthma are similar to EB with asthma. The optimal treatment and prognosis of EB need to be considered, especially in the context of the rising prevalence of asthma and the development of chronic airflow obstruction.
The prognosis for EB in the various clinical syndromes needs to be established by longitudinal observational studies. In particular, is EB a risk factor for subsequent asthma, for airway remodelling, or for the development of chronic airflow obstruction?
What is the optimal treatment for EB without asthma? Should inhaled corticosteroids be given only to control symptoms, or should they be continued during asymptomatic periods in order to reduce exacerbations and prevent disease progression? Are other treatments effective, in particular nasal corticosteroids or histamine H1 antagonists, especially if there is atopy or nasal disease present? It is likely that other treatments will be effective, since atopic cough responds to treatment with systemic histamine H1 antagonists without the need for inhaled corticosteroids in nearly 60% of patients,15,60 and sputum histamine levels are raised in patients with cough with EB.10 It is also likely that patients defined using the ADP as having cough with postnasal drip syndrome have EB and may have responded to treatment of nasal disease including systemic antihistamines.65 Uncontrolled observations indicate that patients with chronic cough do well when treated according to the ADP.21,65 This also suggests that treatments other than inhaled corticosteroids may benefit patients with EB in chronic cough. It will be important to examine the effectiveness of these treatments in controlled studies and to investigate their effects on eosinophilic airway inflammation.
DIAGNOSIS
How can the recognition of EB be incorporated into clinical practice? Based on the prevalence of EB in various syndromes and after clinical assessment and assessment for variability of airflow, patients can be stratified according to their likelihood of having EB. Patients with symptoms, increased variability of airflow, who are not taking inhaled corticosteroids have a high prevalence of EB (66%)68 and can be started on anti-inflammatory treatment without further testing. Patients without variability of airflow or who are on inhaled corticosteroids have a lower prevalence of EB (20%) and assessment of induced sputum77 is warranted to guide further treatment.
The ADP has been used to establish the diagnosis and treatment for patients presenting with chronic cough. The assessment of EB is not part of this protocol. Studies assessing EB and using the ADP have found EB to be present in patients with cough due to CVA, allergic rhinitis, and GOR.21,49,62 Assessment of EB would allow the diagnosis of atopic cough and EB without asthma. Induced sputum analysis would also allow corticosteroid treatment to be commenced with a reasonably high chance of success and would provide an objective marker of treatment response. This is in contrast to the ADP where a diagnosis can only be reached retrospectively after the cough resolves, based upon treatment in an uncontrolled treatment trial and without objective markers of response. It seems likely that assessment of induced sputum for EB could be included in the ADP after assessment for variable airflow obstruction.63
Although the ADP can be applied to patients with chronic cough, its applicability to other conditions such as episodic respiratory symptoms without asthma and EB without asthma has not been established. The usefulness of assessing EB early in the evaluation of these patients is that it permits the introduction of potentially effective treatment relatively early in the evaluation process. There is a need to conduct further randomised controlled trials to validate these recommendations, since at present they are based on level III evidence (table 1⇑).
CONCLUSIONS
Eosinophilic bronchitis, although classically associated with asthma, is now known to occur in other conditions such as allergic rhinitis, chronic cough, episodic respiratory symptoms without asthma, cough variant asthma, and COPD. The causes, inflammatory mechanisms, and response to treatment with inhaled corticosteroids of EB in these syndromes are similar to asthma. The prognosis of EB in terms of subsequent asthma, airway remodelling, and development of fixed airflow obstruction is unknown. EB may be a precursor for subsequent asthma. It can be recognised by induced sputum analysis and may assist in the selection of treatment options.