Article Text

Abstract
BACKGROUND Pseudomonas aeruginosa is a frequent cause of infection in patients with bronchiectasis. Differentiation between non-infected patients and those with different degrees of P aeruginosainfection could influence the management and prognosis of these patients. The diagnostic usefulness of serum IgG antibodies againstP aeruginosa outer membrane proteins was determined in patients with bronchiectasis without cystic fibrosis.
METHODS Fifty six patients were classified according to sputum culture into three groups: group A (n=18) with no P aeruginosain any sample; group B (n=18) with P aeruginosa alternating with other microorganisms; and group C (n=20) with P aeruginosa in all sputum samples. Each patient had at least three sputum cultures in the 6 months prior to serum collection. Detection of antibodies was performed by Western blot and their presence against 20 protein bands (10–121 kd) was assessed.
RESULTS Antibodies to more than four bands in total or to five individual bands (36, 26, 22, 20 or 18 kd) differentiated group B from group A, while antibodies to a total of more than eight bands or to 10 individual bands (104, 69, 63, 56, 50, 44, 30, 25, 22, 13 kd) differentiated group C from group B. When discordant results between the total number of bands and the frequency of P aeruginosa isolation were obtained, the follow up of patients suggested that the former, in most cases, predicted chronic P aeruginosacolonisation.
CONCLUSION In patients with bronchiectasis the degree of P aeruginosa infection can be determined by the number and type of outer membrane protein bands indicating which serum antibodies are present.
- antibodies
- Pseudomonas aeruginosa
- bronchiectasis
Statistics from Altmetric.com
Patients with bronchiectasis are predisposed to persistent lower respiratory tract infections.1 Haemophilus influenzae,Staphylococcus aureus, andStreptococcus pneumoniae may be isolated in the sputum in early or less advanced stages of the disease. Later,Pseudomonas aeruginosa may be detected, alternating with other microorganisms but, as the disease progresses, P aeruginosa displaces the other organisms and appears more consistently in the sputum.2 ,3It has been observed in patients with cystic fibrosis thatP aeruginosa infection of the lower respiratory tract may be associated with a progressive deterioration in pulmonary function.4 ,5 Early detection of initial or intermittent P aeruginosa infection in patients with cystic fibrosis may be important as certain antibiotic treatments have proved useful in preventing or delaying chronicP aeruginosa infection.6
It is possible to monitor the specific immune response toP aeruginosa by antibody detection since it has been proved in patients with cystic fibrosis that the response is greater as the disease evolves or when mucoid phenotypeP aeruginosa is isolated.7 In these patients the production of high titres of specific antibodies toP aeruginosa appears to be an important factor in them becoming chronically infected with P aeruginosa. These antibodies are not only incapable of eradicating the bacteria, but form immune complexes that activate inflammation mediators with subsequent destruction of lung parenchyma tissue and progressive deterioration in pulmonary function.2 ,7 ,8 It has therefore been suggested that the detection of specific anti-P aeruginosaantibodies in patients with cystic fibrosis correlates with an aggressive course of the chronic infection and worse prognosis of the disease.9
Similar events appear to occur in some bronchiectasis patients without cystic fibrosis. The sequence of microorganisms isolated from the bronchial tree is similar and, although P aeruginosa infection in these patients could simply be a marker of severe disease, it has been associated with greater disease progression and worse lung function.10-12 Nevertheless, cystic fibrosis is a disease with specific characteristics and it is unknown whether the antibody response to P aeruginosa in bronchiectasis patients without cystic fibrosis follows the same pattern.
The aim of this study was to establish the presence of specific antibodies to P aeruginosa and to assess whether these antibodies permit differentiation of different infectious states in patients with bronchiectasis not caused by cystic fibrosis.
Methods
PATIENTS
Fifty six patients with bronchiectasis diagnosed by clinical history and high resolution chest CT scanning were included in the study. Two sweat tests were normal in all cases. Blood samples were all negative for 31 cystic fibrosis mutations including AF508, G542X and N1303K, the most frequent mutations in Spain.13 The cause of the bronchiectasis was not identified in 33 cases, 16 patients had a history of pulmonary tuberculosis, six had an immunodeficiency, and one patient had Young's syndrome. All had attended the pneumology outpatient clinic during the previous year and were clinically stable on inclusion in the study. At least three sputum cultures, separated by a minimum of 1 month, were taken in the 6 months before the start of the study.
Patients were classified into three groups according to microbiological criteria: group A (n=18) from whom P aeruginosawas not isolated in any of the sputum samples; group B (n=18) from whom P aeruginosa was isolated alternating with positive cultures for other microorganisms; and group C (n=20) from whom P aeruginosa was isolated in all sputum samples.
Sex, age, time with previous positive cultures to P aeruginosa, number of admissions in the year prior to the study, and pulmonary function spirometric parameters were evaluated in each patient. The results of sputum cultures performed in the 24 months after inclusion in the study were also collected.
BLOOD AND SPUTUM SAMPLE PROCESSING
A blood sample for later antibody study was obtained from each patient. Microbiological study of sputum was performed if the latter fulfilled determined quality criteria on microscopic examination.14 The study included Gram smear, conventional culture in blood agar, McConkey and Sabouraud media, and quantitative culture in chocolate agar. P aeruginosa was identified by conventional microbiological methods15 and the AMS Vitek (Bio Mérieux, Marey-Etoile, France) system.
STRAINS AND CULTURE CONDITIONS
Several P aeruginosa strains isolated from sputum samples of patients with chronic P aeruginosa infection were selected according to their morphological characteristics (mucoid phenotype in blood and McConkey agar). As all had a very similar outer membrane protein pattern on Western blot analysis, the P aeruginosastrain used for detection of anti-P aeruginosa outer membrane protein specific antibodies was selected for its better capacity to grow in the absence of iron.16 The strain was cultured at 37°C under shaking in a chemically defined medium (CDM) containing 40 mM (NH4)2SO4, 3.2 mM K2HPO4.3H2O, 0.62 mM KCl, 0.5 mM NaCl, 0.4 mM MgSO4.7H2O, and 50 mM 3-(N-morpholino)-2-hydroxy-propanesulfonic acid (MOPSO).17The pH of the medium was adjusted to 7.8 with NaOH. Following sterilisation of the medium and before inoculating the strain, 40 mM glucose were added as the only source of carbon and energy.
OUTER MEMBRANE PROTEIN PREPARATION
Outer membrane protein preparation was carried out according to the method of Filip et al.18Bacteria grown at 37°C in CDM were collected by centrifugation and resuspended in sterile physiological serum. The humid weight was calculated and they were resuspended in distilled water at 10 ml for each 0.5 g and broken by sonication in an ice bath (20 kHz for 2 minutes, 5 cycles). Whole cells were eliminated by centrifugation at 5000g for 20 minutes. Sarcosyl (N-lauroyl-sarcosine Na) was added up to a final concentration of 2% to solubilise the inner membranes and incubated at room temperature for 30 minutes. Outer membranes were collected by centrifugation at 38 000g for 1 hour at 4°C. The pellets with outer membrane proteins were resuspended in 50 mM Tris-HCl (pH 6.8) and stored frozen at –70°C until used. The total protein concentration of the preparation was calculated by the benzethonium chloride method with a BM/Hitachi 917 automatic analyser (Boehringer-Mannheim Corporation, Indianapolis, IN, USA) following the method of Luxton et al.19
WESTERN BLOT
Separation of outer membrane proteins was achieved using vertical electrophoresis in SDS-polyacrylamide gel in a 4–20% gradient according to the Laemmli method20 with the Protean II system (Bio-Rad Laboratories, Hercules, CA, USA). The quantity of outer membrane proteins was 120 μg per gel diluted up to a final volume of 250 μl with 50 mM Tris-HCl (pH 6.8). This preparation was mixed with 250 μl of sample buffer (10% glycerol, 2% SDS, 5% 2-mercaptoethanol, 0.003% bromophenol blue in Tris-HCl pH 6.8 (50 mM)) and heated at 90°C for 10 minutes before being inoculated into the gel. Following electrophoresis, transfer to nitrocellulose was made in accordance with the Towbin method21 for 3.5 hours at 100 volts plus 15 hours at 35 volts. The nitrocellulose membrane containing outer membrane proteins was cut into strips 3 mm in width which were stored at 4°C until use.
The Immun-blot Assay Kit (Bio-Rad Laboratories) with anti-human IgG conjugated with alkaline phosphatase was used for detection of type IgG immune response. The whole process was carried out at room temperature and in an orbital shaker. All serum samples were assayed at a dilution of 1/100. Briefly, the nitrocellulose strips were blocked for 1 hour with 5% skimmed milk in Tris-NaCl (20 mM Tris-HCl, 500 mM NaCl, pH 7.5) and washed once with Tris-NaCl with 0.05% Tween 20. Serum samples diluted in Tris-NaCl with 0.05% Tween 20 plus 2% skimmed milk were incubated with the nitrocellulose strips for 2 hours, washed three times with Tris-NaCl with 0.05% Tween 20, incubated for 1 hour with human anti-IgG conjugated with alkaline phosphatase diluted 1/3000 in Tris-NaCl with 0.05% Tween 20 plus 2% skimmed milk, and then incubated for 30 minutes with the substrate (nitroblue tetrazolium and 5-bromo-4 chloro-3 indoyl phosphate) prepared following the manufacturer's instructions.
CALCULATION OF MOLECULAR WEIGHT
The molecular weight of the individual protein bands detected by Western blot was estimated by comparison with a pattern of proteins of known molecular weight (6.5–200 kd) (Bio-Rad Laboratories) which were subjected to electrophoresis and transfer under identical conditions to outer membrane protein preparation.
ASSESSMENT OF WESTERN BLOT TECHNIQUE
To assess the total number of outer membrane protein bands and the presence of each individual band found by our Western blot technique, serum samples from 30 healthy individuals of similar age and sex distribution to the patients with bronchiectasis were assayed.
STATISTICAL ANALYSIS
Qualitative variables are presented as absolute values and corresponding percentages, and quantitative variables are presented as mean (SD) values or median (quartiles 1–3) when normality criteria were not met. Qualitative variables were compared using the Pearson's χ2 test or Fisher's exact test according to application conditions. The Student's t test was used to compare quantitative variables between two groups or the Mann-Whitney U test when normality criteria were not met. Multiple comparisons between three or more groups were made using analysis of variance or the Kruskal-Wallis test if the data were not normally distributed. The level of statistical significance in all cases was ⩽0.05. Optimum cut off points selected were those with the highest efficiency (percentage of well classified individuals), and the area under the ROC curve (ROCarea) with its 95% confidence interval (95% CI) is provided to describe their discrimination power.
Results
PATIENT CHARACTERISTICS
Characteristics of the three groups of patients with bronchiectasis are shown in table 1. Significant differences were found in respiratory functional parameters, absolute and percentage predicted forced expiratory volume in 1 second, and percentage predicted forced vital capacity between the three patient groups and in the number of hospital admissions during the year prior to inclusion in the study.
Characteristics of the three groups of patients with non-CF bronchiectasis
MOLECULAR WEIGHT OF OUTER MEMBRANE PROTEIN BANDS DETECTED BY WESTERN BLOT
The presence of antibodies to 20 bands of P aeruginosa outer membrane proteins was studied by Western blot. The bands were denominated by their estimated molecular weight with a mean of three values of 121, 104, 94, 89, 81, 69, 63, 56, 50, 47, 44, 36, 30, 26, 25, 22, 20, 18, 13, and 10 kd.
ASSESSMENT OF WESTERN BLOT TECHNIQUE
In one of 30 healthy individuals (16 men, mean (SD) age 62 (13) years) the median (quartiles 1–3) total number of bands detected by Western blot was 1 (0.0–1.0). When each of the individual outer membrane protein bands detected was assessed, antibodies to the 56 kd band were found in nine (30%) and antibodies to the 10 kd band in six (20%) of these healthy individuals. Fewer than 10% had antibodies to any of the 12 outer membrane proteins (94, 81, 69, 47, 36, 30, 26, 25, 22, 20, 18, and 16 kd bands). No healthy individuals had antibodies against six outer membrane proteins (121, 104, 89, 63, 50 and 44 kd).
ASSOCIATION BETWEEN TOTAL NUMBER OF BANDS DETECTED BY WESTERN BLOT AND FREQUENCY OF P AERUGINOSAISOLATION
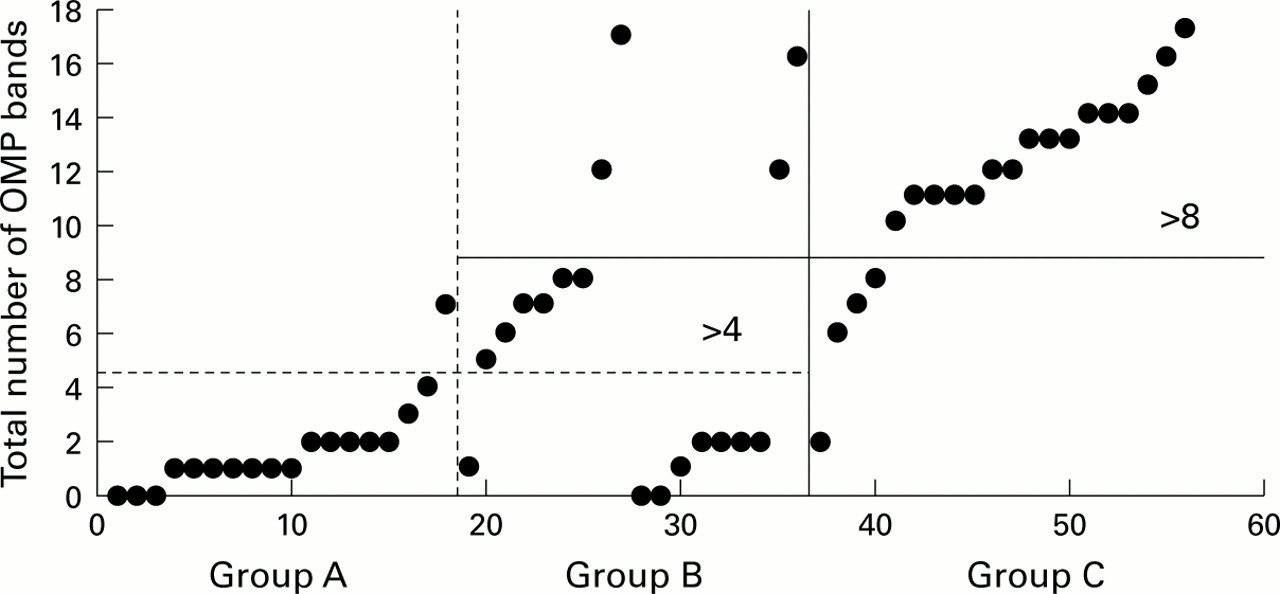
The presence of P aeruginosa anti-outer membrane protein antibodies assessed by the total number of bands in each group of bronchiectasis patients is shown in fig 1 and table 2. No significant differences were found in the total number of bands between those without previous isolation of P aeruginosa (group A) and the healthy individuals, but significant differences were found between the three groups of bronchiectasis patients (table 2). The Kruskal-Wallis test for multiple comparison analysis of the three patient groups indicated that the differences observed were significant between group C and group A (p<0.05) and between group C and group B (p<0.05).

{kind=link}
Total number of outer membrane protein bands (OMP) detected by Western blot analysis. Each patient in the three groups of patients with bronchiectasis (A=18, B=18, C=20) is represented by the total number of OMP bands to which antibodies were detected.
Total number of P aeruginosa outer membrane protein bands to which antibodies were detected by Western blot
All the possible cut off points, using the total number of outer membrane protein bands detected, were assessed to differentiate between the patient groups. The best cut off point between groups A and B was >4 bands (efficiency 75%, ROCarea 0.75, 95% CI 0.58 to 0.88). Similarly, the optimum cut off point obtained to differentiate between groups C and B was >8 bands (efficiency 75%, ROCarea 0.79, 95% CI 0.63 to 0.91).
In group A 17 of the 18 patients (94.4%) had ⩽4 bands and, with the exception of two in whom a first P aeruginosa isolation was obtained 18 and 20 months later, the rest (15/18) remained free from P aeruginosainfection in the follow up period. P aeruginosa was later isolated from the only patient in this group who had >4 bands (7 bands).
Eight of the 18 patients in group B had ⩽4 bands and in seven of these P aeruginosa had been isolated for the first time during the month before the serum sample was taken. With the exception of one case, P aeruginosa was not isolated during follow up. In six of the 18 patients in this group 5–8 bands were detected, but P aeruginosa was isolated in only one. In the four remaining patients >8 bands were detected and P aeruginosa was isolated from three of these during the follow up period.
In 16 of the 20 patients in group C >8 bands were detected and on only three occasions was P aeruginosa not isolated in the follow up period (3, 6 and 12 months of control). In three patients 6, 7, and 8 bands were detected, respectively, althoughP aeruginosa continued to be isolated chronically. In one case the number of bands was ⩽4 butP aeruginosa continued to be isolated chronically.
ASSOCIATION BETWEEN INDIVIDUAL BANDS DETECTED BY WESTERN BLOT AND FREQUENCY OF P AERUGINOSA ISOLATION
The presence of antibodies against individual bands ofP aeruginosa outer membrane proteins and their possible association with the three patient groups was assessed (table 3). No significant differences were found in the presence of individual bands between patients in group A and the healthy individuals. The presence of antibodies against five individual bands (36, 26, 22, 20 and 18 kd) of the 20 detected by Western blot was significant when patients of group A were compared with those of group B (table 3). When patients in groups B and C were compared the difference in the presence of antibodies to 10 bands (104, 69, 63, 56, 50, 44, 30, 25, 22, and 13 kd) was significant (table3).
Results of Western blot by individual P aeruginosa outer membrane protein bands to which antibodies were detected
Discussion
It has been suggested that the specific immune response may identify patients with cystic fibrosis infected withP aeruginosa.22 Although this response would also be expected to be useful in evaluating non-cystic fibrosis patients with bronchiectasis infected withP aeruginosa, no study investigating this possibility has been found in the literature. In this study a correlation was found between the frequency of P aeruginosa isolation in sputum and anti-P aeruginosa antibodies detected by Western blot, which suggests that this technique could identify and distinguish between different degrees of P aeruginosa infection in these patients.
Various types of antigens have been used by different authors to ascertain the presence of specific antibodies to P aeruginosa in patients with cystic fibrosis.22-26We chose to use outer membrane proteins as antigens as they have some advantages, the most important of which are their conservation among the 17 P aeruginosaserotypes,27 their proven antigenicity,28 ,29and the fact that they present no cross reaction with other Gram negative bacilli.27
To obtain the outer membrane protein preparation we assessed several strains isolated from sputum samples of our patients chronically infected by mucoid P aeruginosa, as did Shand et al.17 Since all the strains had a very similar pattern of outer membrane protein on Western blot analysis, as expected by their conservation amongP aeruginosa serotypes,27 theP aeruginosa strain used for detection of anti-P aeruginosa outer membrane protein specific antibodies was finally selected for its better capacity to grow in the absence of iron as this is necessary to guarantee the production of iron regulated outer membrane proteins.16
Although the classic technique for demonstrating the presence of these antibodies has been crossed immunoelectrophoresis,22immunoenzymatic techniques such as enzyme-linked immunosorbent assay23-26 or Western blot analysis17 ,28 ,30 have proved to be much more sensitive; the latter permits simultaneous study of antibodies against different antigenic components. Our Western blot technique even introduces some improvements compared with that used by Shand et al 17 since, with the use of gels in a gradient of 4–20%, better separation and transfer of outer membrane proteins to nitrocellulose membrane are achieved, thereby permitting better assessment of high molecular weight outer membrane proteins.31
As reported in other studies,10 ,12 the presence ofP aeruginosa in the sputum of non-cystic fibrosis patients with bronchiectasis is associated with greater deterioration in pulmonary function and a higher number of hospital admissions. We do not believe that this implies a bias which invalidates the results since it is clear that the detection of antibodies against P aeruginosa must be attributed directly to the immunological stimulus resulting from the presence of this bacterium in the bronchial tree.
With respect to the total number of bands found, our results indicate that the presence of antibodies against more than four bands permits differentiation between patients with bronchiectasis from whomP aeruginosa was not isolated (group A) and those with intermittent isolation (group B). The presence of antibodies to some protein bands in patients in group A might be explained by the presence in their serum of antibodies that may cross react with some of the outer membrane proteins studied, in most cases (38.9%) against the 56 kd protein. Similarly, 30% of individuals in the healthy group showed reactivity against the same protein. In the only patient in group A who had more than four bands, P aeruginosa was isolated chronically during follow up. In fact, using an enzyme-linked immunosorbent assay, Brettet al 32 found that an increase in the titre of IgG against P aeruginosasurface antigens above the control range preceded isolation ofP aeruginosa in patients with cystic fibrosis in whom it had not been isolated previously. In the present study we also found that the presence of antibodies against more than eight bands permits the diagnosis of chronic isolation ofP aeruginosa in bronchiectasis patients. The distribution of the results in group B may be explained by the difficulty in interpreting microbiological results when isolation ofP aeruginosa is not consistent. However,P aeruginosa was not isolated again in most of the patients in group B with four bands or less, while in those with more than eight bands P aeruginosa continued to be isolated during the follow up period. Thus, in the former patients an absent or low antibody response could suggest a transient infection with response at the bronchial level but not sufficiently intense at the systemic level, while in the latter group an increased response would suggest an early response or failure inP aeruginosa recovery owing to an inadequate sample or low bacteria counts in chronically infected patients. Høibyet al 22 observed a positive correlation between the severity of P aeruginosa infection in patients with cystic fibrosis and the number of precipitating bands detected by crossed immunoelectrophoresis using soluble antigen. The number of precipitating bands has even been used together with sputum microbiology to identify patients with chronic P aeruginosainfection.22 Shand et al,30 using the same soluble antigen and Western blot technique, found highly significant differences in the number and intensity of blotted bands between serum samples taken before and after a diagnosis of P aeruginosa lung infection. Hancock et al,28 using Western blot and outer membrane protein preparation (as in our study), found a correlation in patients with cystic fibrosis between the presence of antibodies against P aeruginosa outer membrane proteins and P aeruginosa isolation for more than one year.
Shand et al 17 studied the chronological appearance of antibodies against outer membrane proteins including those dependent on iron. The earliest antibodies appeared against outer membrane protein H1 (21 kd) and were generally accompanied by antibodies against G (20–25 kd) and/or I (15–16 kd). Antibodies against iron-dependent outer membrane proteins (71, 74, 76, and 83 kd) appeared late and only in seriously ill patients; thus, it is likely that these proteins are not expressed until the infection is very advanced. Although we did not identify the outer membrane protein bands of P aeruginosa or perform sequential analysis of patients, we did observe that antibodies against 36 kd and/or 18 kd proteins were probably the most precocious since, though rarely found in group A patients, they did appear in most of the patients in groups B and C. Antibodies to the 69, 63, 30, 25, and 22 kd proteins differentiated well between patients in groups C and B and therefore probably appear later. Our high molecular weight proteins (81–121 kd) probably corresponded to iron-dependent outer membrane proteins and, as observed by Shand et al,17 appeared much later only in some patients in group C.
As in cystic fibrosis, determination of anti-P aeruginosa antibodies could also be useful in patients with bronchiectasis without cystic fibrosis. It would be particularly useful in patients who have difficulty in producing good quality samples for microbiological sputum culture and in those whose previous clinical and microbiological history is unknown. Furthermore, it would contribute additional information to that obtained from microbiological study of sputum samples.
Acknowledgments
The authors wish to thank Christine O'Hara for useful manuscript corrections, Rosa Lloria for secretarial assistance, and Maria Teresa Barbero for technical assistance.
E Caballero and M-E Drobnic both contributed equally to the study.