Article Text

Abstract
BACKGROUND Investigation and management of pleural effusions is an important clinical problem yet the pathogenesis of pleural fluid accumulation is poorly understood. Vascular endothelial growth factor (VEGF) is a potent inducer of capillary permeability that is produced by both malignant and inflammatory cells. A study was undertaken to determine whether VEGF has a potential pathogenic role in the development of pleural effusions and whether VEGF receptors are present on human pleural mesothelial cells.
METHODS Normal and inflamed pleura were examined immunohistochemically for the presence of FLT-1 (the fms-like tyrosine kinase receptor of VEGF). VEGF levels were measured by ELISA in 78 consecutive patients presenting with undiagnosed unilateral pleural effusions and the levels were correlated with the aetiology of the effusions.
RESULTS Immunohistochemical staining of normal and diseased pleura demonstrated the presence of the FLT-1 VEGF receptor on human mesothelial cells. Median VEGF levels were 2500 pg/ml in the malignant group and 305 pg/ml in the non-malignant group (median difference 1397.5 pg/ml (95% CI 851 to 2693), p<0.005). Median VEGF levels varied according to tumour histology. VEGF levels were also significantly raised compared with transudates (median 36.5 pg/ml) in empyema (4651 pg/ml (95% CI 833 to 10 000), p<0.001) and parainfectious effusions (360 pg/ml (95% CI 46 to 597), p<0.005).
CONCLUSIONS This first report of VEGF receptors on pleural mesothelial cells has indicated a potential mechanism for the biological activity of VEGF on pleural tissue. VEGF levels are raised in the majority of exudative effusions, implying a pathogenic role for this molecule in the development of pleural effusions.
- vascular endothelial growth factor
- pleural effusions
- pathogenesis
Statistics from Altmetric.com
Pleural effusion is a common clinical problem arising as a result of many aetiologies. It has been estimated that there are over 800 000 cases per year in the USA.1 The diagnosis and management of pleural effusions remains difficult and is associated with significant costs to both patients and the health care system. It is likely that increased fluid production within the pleural space is a feature in most cases of pleural effusion.2 Our current understanding of the basic mechanisms by which fluid accumulates within the pleural space is poor and limits the development of improved treatment to prevent recurrence.
Vascular endothelial growth factor (VEGF), also known as vascular permeability factor, is a 34–42 kD homodimeric protein which is a potent inducer of capillary permeability, being 10 000 times more potent than histamine in vitro. It functions through binding with its fms-like tyrosine kinase receptor (FLT-1). VEGF is believed to function as a tumour angiogenesis factor being mitogenic for endothelial cells.3 VEGF mRNA is formed by almost all tumours4 and VEGF is secreted by tumour cell lines in vitro.5 These two properties led to its study in experimental models of malignant ascites showing that accumulation of fluid is directly correlated with VEGF production.6
Several histological types of lung cancer have been shown to express VEGF.7-9 Indeed, the metastatic potential of lung tumours has been correlated with the immunohistochemical expression of VEGF and its receptor FLT-1 in tumour sections.10 However, VEGF is also produced by most inflammatory cells including eosinophils, lymphocytes, macrophages, and neutrophils.4 ,11 Raised levels are present in the synovial fluid of patients with rheumatoid arthritis.12 Proinflammatory cytokines such as tumour necrosis factor α (TNFα) and interleukin 8 (IL-8) stimulate neutrophils to produce VEGF.11 We hypothesised therefore that VEGF production might be a final common pathway for pleural fluid accumulation in both malignant and inflammatory effusions.
This study was undertaken (1) to determine whether the VEGF receptor FLT-1 is present on the pleural surface, a prerequisite for a role of VEGF in the pathogenesis of pleural effusions, and (2) to determine whether VEGF levels vary in pleural fluid of different aetiology.
Methods
PATIENTS
In an attempt to reduce the effect of selection bias, consecutive patients with undiagnosed unilateral pleural effusion were included in this study. Seventy eight patients were studied (48% men) with an age range of 36–94 years. The causes of pleural effusion were defined as follows:
Malignant effusion (n = 36): an effusion with positive histological proof of a malignant process.
Probable malignant effusion (n = 4): a clinically malignant effusion with no other obvious cause, that recurred at least once, but the patient declined further investigation.
Empyema (n = 14): an effusion that was either microbiologically positive or purulent fluid with a pleural fluid lactate dehydrogenase (LDH) level above 1000 IU/l and a glucose level below 2 mmol/l.
Parainfectious effusion (n = 10): patients with a clinical history suggestive of recent infection who had no features of empyema and the effusion did not recur at six week outpatient follow up.
Transudates (n = 6): effusions secondary to left ventricular impairment or hypoalbuminaemia with a protein content of less than 30 g/dl and no other identifiable cause.
Rheumatoid effusion (n = 4): patients with clinical rheumatoid arthritis with either biopsy proven histology or rheumatoid factor positive in the pleural fluid with no clinical evidence of empyema.
Miscellaneous (n = 4): effusions that did not fit into the above criteria.
For immunohistochemical staining, formalin fixed and paraffin embedded pleural tissue sections from thoracoscopic biopsy specimens were obtained from patients with inflammatory (n = 2) and metastatic effusions (n = 2). Normal pleura was obtained from patients undergoing pleurectomy for recurrent pneumothorax (n = 3).
STUDY DESIGN
All patients had routine pleural fluid cytological examination, microbiological examination, and measurement of pleural fluid protein, glucose and lactate dehydrogenase (LDH) levels. Pleural fluid (20 ml) was centrifuged to remove the cellular fraction and frozen at –70°C for subsequent VEGF measurement. Further investigation of the underlying cause of the effusion was performed according to standard clinical practice. The Southmead ethics committee granted full approval for the study.
Immunohistochemical staining for the FLT receptor was carried out using a rabbit polyclonal antibody raised against a carboxy terminal of the human FLT peptide (Santa Cruz, USA). Immunostaining was performed using the DAB method. Sections 4 μm thick were cut consecutively from formalin fixed and paraffin embedded tissue samples mounted on poly-l-lysine coated slides and dried overnight at 58°C. Paraffin sections were dewaxed by xylene, rehydrated with graded concentrations of ethanol, and washed in Tris-buffered saline (pH 7.6) for 10 minutes. For optimal antigen retrieval, sections were pressure cooked in 0.01 M citrate buffer (pH 6.0) for 90 seconds.
Endogenous peroxidase activity was blocked using a 3% hydrogen peroxide solution in methanol for 10 minutes. After washing twice in phosphate buffered saline (PBS)/1% saponin, endogenous avidin and biotin were blocked using the Vector Labs Blocking Kit. Sections were again washed in PBS/1% saponin.
Sections were incubated with primary antibody solution for two hours at room temperature using a working dilution of the antibody 1:150 concentration. Negative control slides were incubated with rabbit polyclonal antibody (Super Sensitive Rabbit, Biogenix, USA). Slides were rinsed twice in PBS/1% saponin.
Secondary biotinylated anti-immunoglobulin antibody (Biogenex, USA) was added for 30 minutes at room temperature and the sections rinsed twice with PBS/1% saponin. Streptavidin conjugated to horseradish peroxidase (Biogenex, USA) was incubated for 30 minutes then rinsed off with deionised water. DAB substrate solution was then added for 30 minutes. A brown colour reaction represented a positive result.
VEGF was measured using a sandwich ELISA kit according to the manufacturer’s instructions (R&D Systems, UK). This ELISA has an interassay precision in our hands of 7.8%. The intra-assay coefficient of variation in our hands is 6.8% The minimum detectable dose of VEGF is 3.75 pg/ml. Recovery of VEGF spiked in five samples of malignant effusion is 97%.
STATISTICAL ANALYSIS
The Ryan-Joiner normality test was used to test the distribution of the data. Significant differences between raw data and normal distribution were observed (p<0.01). To justify quoting multiple comparisons of VEGF between various patient groups an initial Kruskal-Wallis test was performed. A highly significant result was found (p = 0.001). Mann-Whitney tests were therefore used throughout the study to compare individual groups. All results are quoted as median values with median differences and 95% confidence intervals for differences. Statistics were analysed using Minitab for Windows.
Results
IMMUNOHISTOCHEMICAL EXPRESSION OF FLT-1 RECEPTOR IN HUMAN PLEURA
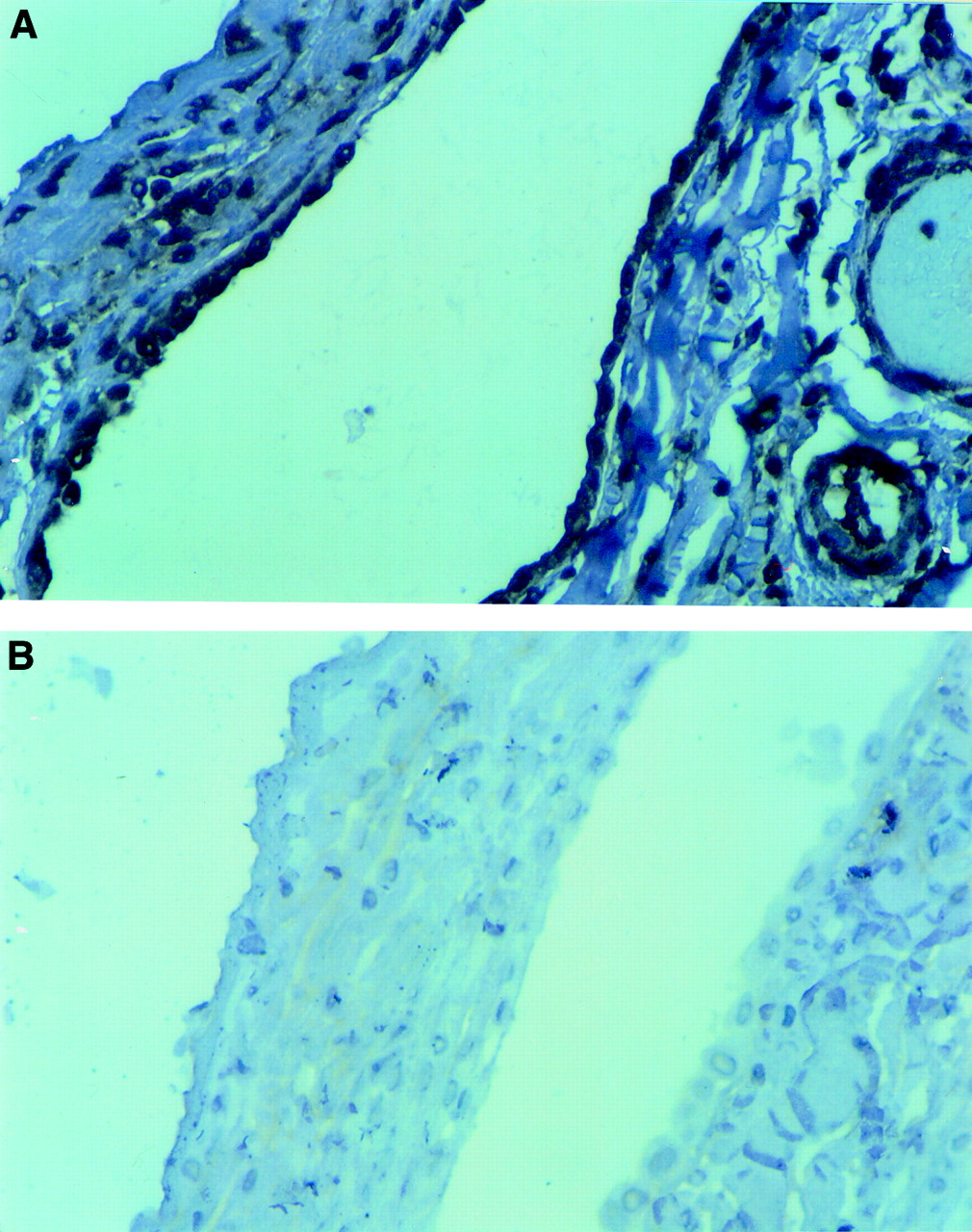
Pleural tissue from various sources was tested by immunohistochemistry for the presence of the FLT-1 VEGF receptor. Mesothelial cells and vascular endothelial cells from normal pleura stained intensely for FLT-1 (fig 1). FLT-1 receptors were also present on chronically inflamed pleura and infiltrating malignant tissue. We believe this is the first report of the expression of FLT-1 by pleural mesothelial cells and demonstrates a mechanism by which VEGF may be involved in the pathogenesis of pleural effusions.

Immunohistochemical expression of FLT-1 receptor on (A) normal human pleura. (B) Negative control.
VEGF IN PLEURAL FLUID
Seventy eight consecutive patients were recruited between October 1996 and July 1998. The median VEGF level in the malignant effusions was 2500 pg/ml compared with 305 pg/ml in the non-malignant group (median difference 1397.5 pg/ml (95% CI 851 to 2693), p<0.0001, Mann-Whitney U test). The histology of the tumour appeared to influence the level of VEGF present within the malignant effusions, as shown in fig 2.

Pleural fluid levels of VEGF according to histology.
Pleural fluid cytology was positive in 36% of malignant effusions. Pleural biopsy increased the diagnostic rate to 50%. Additional invasive procedures were needed to diagnose the nature of the cytologically negative effusions in 36 patients.
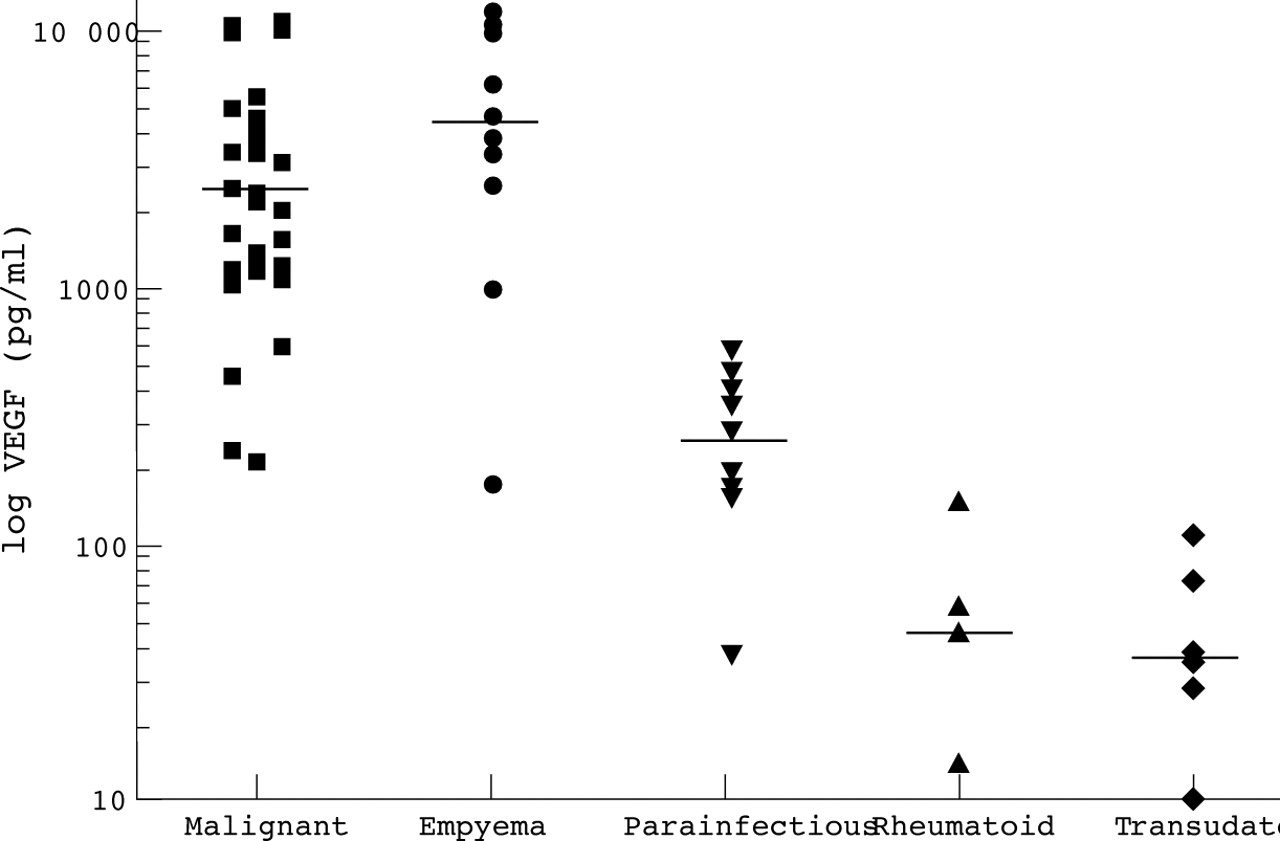
Inspection of the data in the non-malignant group showed that VEGF levels varied greatly according to the aetiology of the effusion. Median empyema fluid VEGF levels were significantly raised at 4651 pg/ml compared with 360 pg/ml in the parainfectious effusions (mean difference 4291.0 pg/ml (95% CI 833 to 10 000), p<0.006, Mann-Whitney U test). Parainfectious effusions had significantly more VEGF than transudates (median 36.5 pg/ml, median difference 289.4 pg/ml (95% CI 46 to 597), p<0.005). There was no significant difference between rheumatoid effusions (median 55.5 pg/ml) and transudates (median 36.5 pg/ml, p = 0.31, Mann-Whitney U test). The differences between the major groups are illustrated in fig3.

{kind=link}
{kind=link}
{kind=link}
Pleural fluid levels of VEGF according to aetiology.
Figure 3 shows that most malignant effusions and empyemas had a VEGF level above 1000 pg/ml. There was no significant correlation between survival in the malignant group and pleural VEGF levels. When empyemas are excluded using established clinical criteria, only patients with malignancy had a VEGF level above 1000 pg/ml.
Discussion
Abnormal accumulation of pleural fluid probably occurs due to a combination of increased pleural fluid formation and, in some cases, decreased lymphatic drainage.2 The molecular mechanisms underlying increased fluid accumulation in exudative effusions are poorly understood but may involve the intrapleural production of cytokines such as TNFα and TGFβ which are known to increase vascular permeability.13 ,14 No single mediator has so far been found to be important in all types of exudative pleural effusion.
This study has shown an increased level of VEGF above the maximum value found in transudates in 90% of exudative pleural effusions. VEGF levels vary significantly according to both aetiology and, in the malignant group, according to histology. We believe this is the first study to demonstrate the immunohistochemical expression of the VEGF receptor, FLT-1, by human pleural mesothelial cells, suggesting that intrapleural VEGF may be biologically active.
VEGF is one of the most potent inducers of endothelial cell permeability currently known, being active in the picomolar range in vitro. Animal experiments of malignant ascites have shown that accumulation of ascitic fluid is closely correlated with ascitic fluid concentration of VEGF.6 VEGF increases the permeability of the peritoneal microvessels in parallel with increases in ascitic fluid volume.15 If human pleural mesothelial cells or microvessels respond in a similar fashion, then abnormal pleural fluid accumulation may occur in response to increased intrapleural VEGF concentrations.
Transudates occur due to changes in osmotic pressure gradients, and therefore we would expect the observed low VEGF levels. Surprisingly, rheumatoid effusions also had low levels of VEGF. This is in contrast to the high levels found in the synovial fluid of rheumatoid patients.12 If VEGF production is important for fluid accumulation, then the low VEGF levels might explain why rheumatoid effusions are usually static and rapid fluid accumulation is not a key clinical feature.16
When left untreated, empyema fluid develops fibrinous loculations and progressively organises into fibrotic tissue. Angiogenesis is known to be an early part of this process in experimental empyema. Many known pro-angiogenic factors are present within empyema fluid including TGFβ, IL-8, and TNFα.17 All of these can stimulate VEGF secretion from endothelial or inflammatory cells.18 ,19
VEGF contributes to angiogenesis by both direct and indirect mechanisms.20 It stimulates microvascular endothelial cells to proliferate, to migrate, and to alter their pattern of gene expression. In addition, VEGF renders these same microvascular endothelial cells hyperpermeable to fibrinogen and promotes the clotting of fibrinogen within the extravascular space. This leads to the formation of a fibrin gel which may serve as a provisional matrix that favours and supports the growth of new blood vessels and other mesenchymal cells that generate mature vascularised stroma.21 The known biological functions of VEGF suggest therefore that high levels within empyema fluid may promote both the accumulation of fluid and the process of loculation/organisation of chronic empyema.
This study suggests that VEGF levels are significantly raised in malignant compared with benign effusions. The levels are variable according to the histology, with adenocarcinomas producing the largest amounts. From this retrospective patient series it is evident that VEGF levels above 1000 pg/ml are suggestive of either empyema or malignancy. After excluding empyema using established clinical criteria, all patients with a VEGF level above 1000 pg/ml had malignancy. The clinical use of VEGF measurement as a diagnostic tool warrants further validation in a prospective clinical trial.
In summary, this study has demonstrated increased levels of VEGF in the majority of exudative pleural effusions. The presence of VEGF receptors on pleural mesothelial cells suggests this may be biologically active. If VEGF is important for pleural fluid accumulation then novel anti-VEGF therapies currently undergoing clinical trials in refractory lung cancer could directly influence the rapidity of pleural fluid accumulation in addition to possessing an anti-tumour effect.22
Acknowledgments
The authors thank Dr N Ibrahim for providing the tissue sections. This research was funded by the H C Roscoe Fellowship which is administered by the British Medical Association.