Article Text

Abstract
BACKGROUND Although patient education is a key step in the Australian Asthma Management Plan, its impact has not been assessed in a hospital outpatient asthma clinic.
METHODS A controlled trial was undertaken in 125 adults with asthma recruited from the Alfred Hospital Asthma and Allergy Clinic and randomly allocated to an intervention (n = 64) or control (n = 61) group. Subjects in the intervention group attended three education sessions, each of 90 minutes duration, spread over three successive weeks. Asthma knowledge, quality of life, self-management skills, and attitudes and beliefs about asthma were assessed by questionnaires at baseline and after six months. The intervention group was also assessed immediately after the three education sessions. The control group was evaluated after six months of usual care.
RESULTS Asthma knowledge improved significantly in the intervention group after three education sessions (p = 0.0001) and this was retained six months later (p = 0.03). The impact of asthma on quality of life decreased significantly immediately after intervention (p = 0.03) but this was not maintained six months later (p = 0.35). On the other hand, the intervention had little impact on self-management skills or attitudes and beliefs about asthma. However, the control group had also improved their knowledge, quality of life and self-management skills after six months of usual care. The difference in mean change in knowledge score at six months between the intervention and control groups was not significant (p = 0.51).
CONCLUSIONS In contrast to some other studies, a limited asthma education programme in a hospital outpatient setting had a positive impact on patients’ knowledge of asthma, but not on their quality of life, self-management skills, or attitudes and beliefs about asthma.
- asthma education
- outpatient clinic
Statistics from Altmetric.com
Asthma is a major public health problem in Australia1 with a prevalence in adults and adolescents of approximately 7% and 16.5%, respectively.2 ,3 A significant number of asthma deaths are thought to be preventable.4 ,5 Asthma and related health problems use a significant percentage of the health care budget in most developed countries.6 ,7
Asthma education is considered an essential component of asthma management8 and is necessary to help patients gain the motivation, skills and confidence to control their asthma.9 The six step Australian Asthma Management Plan (AAMP) was developed by the Thoracic Society of Australia and New Zealand10 to improve asthma management. Patient education is one of the six components of the plan. To date, little evaluation of the level of asthma education among patients has been conducted in the context of the six step AAMP. Most importantly, no study has evaluated patient education in a hospital outpatient clinic. Only two randomised controlled trials of asthma education have previously been conducted in Australia. Allen et al 11studied asthmatic patients from the community and Yoonet al 12 studied adult asthmatic patients admitted to a university teaching hospital for a severe exacerbation of asthma. We report the impact evaluation of a randomised controlled trial of an education programme for adults with asthma in a hospital outpatient clinic.
Methods
The study was conducted in 1994/95 at the Alfred Hospital’s Asthma and Allergy Clinic which is a public outpatient clinic in the inner south-eastern suburbs of Melbourne, Victoria. The study protocol was approved by the Alfred Hospital ethics review committee and informed consent was obtained from all patients.
SUBJECTS
Patients were eligible if they were diagnosed as having asthma by an attending physician and asthma was their primary problem, were over the age of 16 years, were literate and capable of completing questionnaires in English, intended to reside in Melbourne during the six month study period, and had a recorded address. The diagnosis of asthma was based on the American Thoracic Society criteria.13 Patients for whom asthma was not their major illness, those with hearing or sight problems, and those who could not communicate, read and write English adequately were excluded from the study.
RANDOMISATION
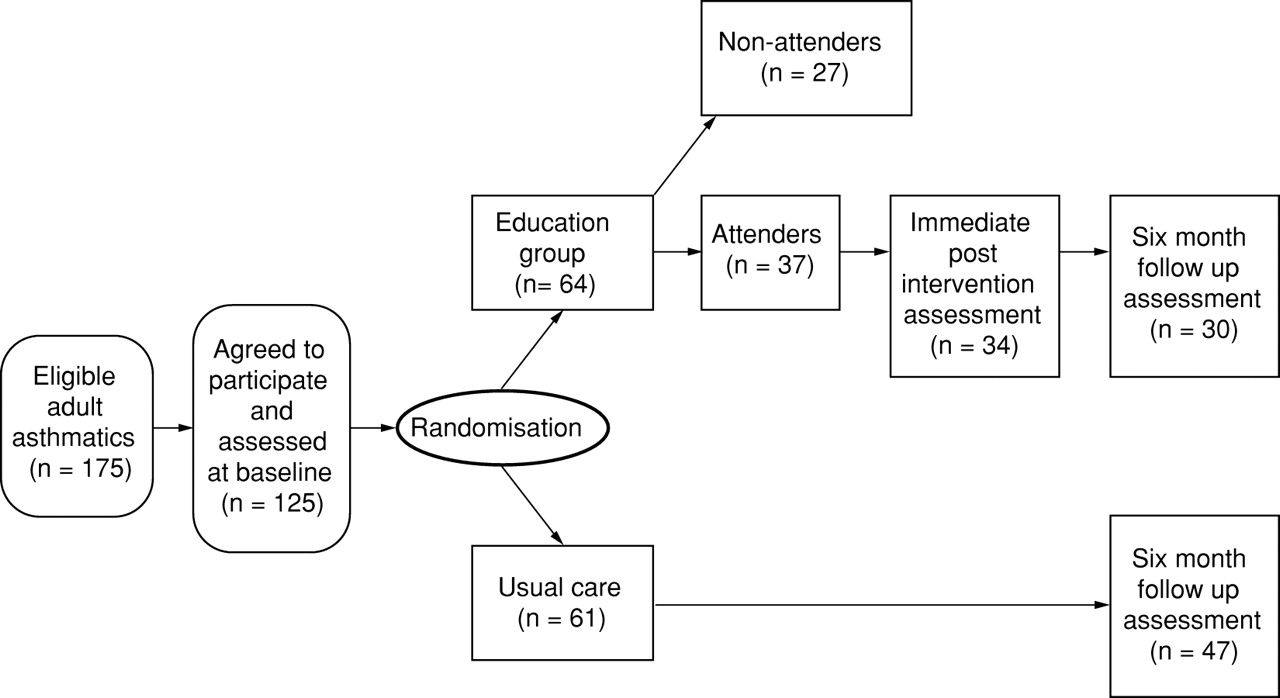
A total of 125 patients who agreed to participate in the study were allocated to either intervention (n = 64) or control (n = 61) groups by a simple random number table. The study design is shown in fig 1.

Study design for a randomised trial of asthma education.
INTERVENTION
The theoretical framework for the intervention was based on “Social Learning Theory”.14 The model described by Hawe et al 15 for evaluation of a health promotion programme was adopted and formed the basis upon which the current intervention programme was structured. The patient education checklist described in the National Asthma Campaign “Asthma Management Handbook”16 was adopted as indicating the educational needs of subjects with asthma. An intervention programme was planned to include detailed objectives, contents, methods, and evaluation tools relevant to the needs of the adult population attending the outpatient clinic.
The intervention programme was organised into three educational sessions each of 90 minutes duration spread over three successive weeks. Patients in the intervention group were taught self-management skills such as how to recognise the features of poorly controlled asthma and when to seek medical help, peak flow monitoring, aerosol inhalation technique and devices. Specifically, the first session covered basic knowledge about asthma, the physiology of asthma and triggers of asthma, the second session addressed the topic of the understanding of and skills in using peak flow meters, peak flow record books and asthma action plans, and the third session covered the understanding of and skills in the use of asthma medications and devices. The education sessions were facilitated by qualified nurse educators with experience in counselling and teaching asthma patients. At the end of every session patients were given a package of printed asthma education materials.
The study subjects were organised into five groups with a maximum of 13 subjects per group. Peak flow meters were given out at no cost to those who participated and completed the study.
DEMOGRAPHIC AND CLINICAL DATA
Data such as age, sex, cigarette smoking, languages other than English, place of birth, and socioeconomic status were collected. The age of onset of asthma, previous admissions, asthma severity, prior asthma status, nocturnal asthma symptoms in the previous six weeks, exercise limitation, percentage predicted forced expiratory volume in one second (FEV1), diurnal variability in peak expiratory flow (PEF), and use of medications were recorded. The predicted FEV1 at baseline was calculated for both men and women separately using prediction equations described by Gibsonet al.17 The mean PEF variability was calculated using the equation: % variability = (highest—lowest)/highest × 100 as described by Woolcocket al.10 Access to or owning a peak flow meter and written asthma management plans were also assessed.
The severity of asthma was categorised according to medication requirements. Patients were classed as mild if they used bronchodilators less than once a week and did not use inhaled steroids, moderate if they used bronchodilators together with inhaled steroids, and severe if they used bronchodilators more than 3–4 times per day together with inhaled or oral steroids. Medications used were grouped into generic categories (β agonists, anticholinergics, and inhaled or oral steroids).
QUESTIONNAIRES
Each patient recruited was required to complete the four questionnaires twice (on entry and after six months). In addition, subjects in the intervention group who had attended the programme were to complete the four questionnaires immediately after the last session.
The Asthma General Knowledge Questionnaire11 was used to assess patients’ knowledge of asthma. The questionnaire was marked out of 31 and the knowledge score was the total number of correct answers. The Asthma Quality of Life Questionnaire (AQLQ)18consisted of 20 items which made up one total quality of life scale and four subscales of “breathlessness”, “mood disturbance”, “social disruption”, and “concern for health”. A single total AQLQ score was obtained by adding scores for the 20 items, dividing by 20 and multiplying by 2.5. The scores for the four subscales were calculated in the same way. The higher the score, the greater the impact of asthma and the poorer the quality of life. The validity and reliability of this AQLQ have been reported elsewhere.18Hypothetical Asthma Attack Scenarios19 were used to assess the self-management skills of patients and contained two separate scenarios—one attack of slow onset and another of rapid onset. This questionnaire has proved to be a simple and effective method of identifying self-care problems.19 ,20 The scoring method of Kolbe et al 20 was used to assess patients’ responses. The Asthma Attitudes and Beliefs Questionnaire21 was used to assess patients’ attitudes and beliefs about asthma. The questions covered were: how it felt to have asthma, the effect of asthma on relationship with others, severity of asthma, the effect of asthma on activities, asthma attacks, asthma medication, and the quality of the relationship with the treating doctor.
All patients received their usual asthma management by the consulting physicians during their scheduled clinic visits. The purpose of the education programme was explained to all patients at the time of enrolment. Subjects in the control group were subsequently given the opportunity to attend all sessions at the end of the study period. No requested educational information was withheld from any patients.
ANALYSIS OF DATA
Questionnaire responses were coded, double entered, and verified before analysis using the SAS for Windows statistical package.22 Categorical variables were summarised as percentages and associations tested in contingency tables by χ2 tests. For continuous variables which were normally distributed the difference in mean change in scores between groups was assessed by the unpaired Student’s t test. Paired Student’s t tests were used to determine the significance of mean changes from baseline in each outcome within groups. For continuous variables which were not normally distributed equivalent non-parametric tests were used. Differences in change in binary categorical variables within each group were analysed using McNemar’s test and the changes between the two groups were assessed by χ2 tests for trend. Analysis of covariance (ANCOVA) was used to adjust for characteristics unequally distributed at baseline which could potentially confound the association between the intervention group and asthma knowledge. The ANCOVA model used asthma knowledge at six months as the outcome with baseline knowledge employed as a covariate. The potential confounders were age, written asthma action plan, educational status, atopy, languages spoken other than English, prior asthma status, and inhaled steroid use. All statistical tests were two tailed and p values of <0.05 were used to determine statistical significance.
The sample size calculation was based on the current and expected increase in the mean asthma knowledge score. During the pilot phase a study of 99 adults with asthma indicated that the mean asthma general knowledge score was 20.7 (out of 31) with a standard deviation of 4.2. As a result of the educational intervention it was hypothesised that the mean knowledge score would increase to 24 after six months in the intervention group but remain at 21 in the control group. A difference between the groups of three units was therefore hypothesised at the end of the six month period. Assuming a standard deviation of 4.2 between knowledge scores of subjects in each group at the six month follow up, a sample size of 42 patients per group was required to detect a difference of three units with 90% power using a two tailed 5% significance level. Allowing for one third to drop out, the sample size was increased to a target of 65 in each group.
Results
PARTICIPATION AND RESPONSE RATES
All 125 adult subjects who agreed to participate completed the baseline questionnaires. Of those randomly allocated to the intervention group (n = 64), 34 (53.1%) attended the full programme and completed questionnaires immediately after intervention, and 30 (88.2%) of these participants completed the six month follow up questionnaires. Of those assigned to the control group (n = 61), 47 (77%) completed the six month follow up questionnaires. Data from the 125 subjects at baseline (64 intervention and 61 control), the 34 intervention group subjects who attended the programme, and 30 of the intervention and 47 of the control group subjects who completed the six month follow up questionnaires form the basis of this report. The characteristics of the participants and non-participants have been reported previously.23 Patients who were over 60 years old and allocated to immediate education were more likely to attend a hospital based asthma education programme.
BASELINE CHARACTERISTICS
The mean (SD) age was 45.6 (18.4) years (range 16–82); 40% of the sample were men, 27% were pensioners, 17% were employed in trade and clerical jobs, 13% in para-professional or professional jobs, and 10% were students. Over half (59%) of the subjects had received secondary education, a further 27% had also received tertiary education, and 14% had primary education only. Sixty four per cent were Australian born and 17% were able to speak a language other than English. More than half (65%) had never smoked, 32% were ex-smokers, and only 3% were current smokers. Most (84.2%) of the participants were atopic; 57% had developed asthma between the age of 0 and 17 years, and 65% had had one or more previous admissions to hospital with asthma.
Almost all of the sample (96%) had either moderate or severe asthma based on their medication use; 11.2% had been admitted to the intensive care unit, 26% had lost consciousness during an attack, 55% reported nocturnal symptoms of asthma in the last six weeks, and 48% had limitation of exercise tolerance. The mean (SD) FEV1was 54.1 (18.6)% predicted and the median diurnal variability in PEF over one week was 14.6% (range 1.36–45.5%). The median duration of attendance of subjects at the asthma clinic was 5 years (range 0–36).
BASELINE COMPARABILITY
There were no important differences between the intervention and control groups at baseline (table 1). However, there were slightly more pensioners and subjects with primary education in the intervention group than in the control group, probably indicating that the older subjects randomised to intervention had less opportunity for education. There were slightly more subjects with an onset of asthma between the ages of 46 and 69 years in the intervention group than in the control group.
Baseline characteristics of subjects
There were no relevant differences in medication usage between the two groups at baseline. In both groups almost all of the subjects (98%) were using a β agonist bronchodilator. Compared with other types of medication the use of anticholinergic medication was low in both groups (intervention 9.4%; control 13.1%). On the other hand, the use of inhaled corticosteroids was 95% and 89% in the intervention and control groups, respectively. The proportion of subjects who had owned or had access to a peak flow meter was 70.3% and 70.5% in the intervention and control groups, respectively; 42% of the intervention group and 46% of the control group had written asthma action plans.
MAIN OUTCOMES AT BASELINE
Asthma knowledge
There was no significant difference in the mean knowledge scores between the intervention and control groups at baseline (t = 0.35, p = 0.72; table 2).
Asthma knowledge, quality of life and self-management skills at baseline
Impact on quality of life
There were no differences in either the total score or any of the four subscales of quality of life between the two groups on entry to the study (table 2). In both groups asthma had the greatest impact on the breathlessness subscale and the least impact on the social disruption subscale.
Self-management skills
Despite the control group scoring slightly higher than the intervention group in the rapid onset scenario, onset scores were similar for the two groups on entry to the study (table 2).
Attitudes and beliefs about asthma
On entry to the study few significant differences were found between the two groups. However, significantly more patients in the intervention group than in the control group would have taken action before their asthma deteriorated (table 3).
Patients’ ability to take action before asthma deteriorated
IMPACT OF INTERVENTION
Asthma knowledge
Table 4 shows the asthma knowledge scores immediately following the intervention, at six months, and the changes that occurred. Knowledge scores increased significantly in the intervention group immediately following the intervention and the six month follow up score was still significantly higher than the baseline score. However, the knowledge score at six months was significantly lower than the score immediately after intervention. The control group also showed an improvement in knowledge scores from baseline to six months but this did not achieve statistical significance. Comparison of the intervention and control group knowledge scores without adjusting for covariates gave a difference in average change in knowledge score over six months of 0.6. After adjustment for age, written asthma action plans, education, atopy, languages spoken other than English, prior asthma status, and inhaled steroids, the difference between the change in mean knowledge scores was 1.00 (95% CI –0.66 to 2.65). However, there was still no clinically important or statistically significant difference in change in knowledge scores between the two groups at the six month time point.
Knowledge scores for the intervention and control groups after education (maximum score 31)
Quality of life
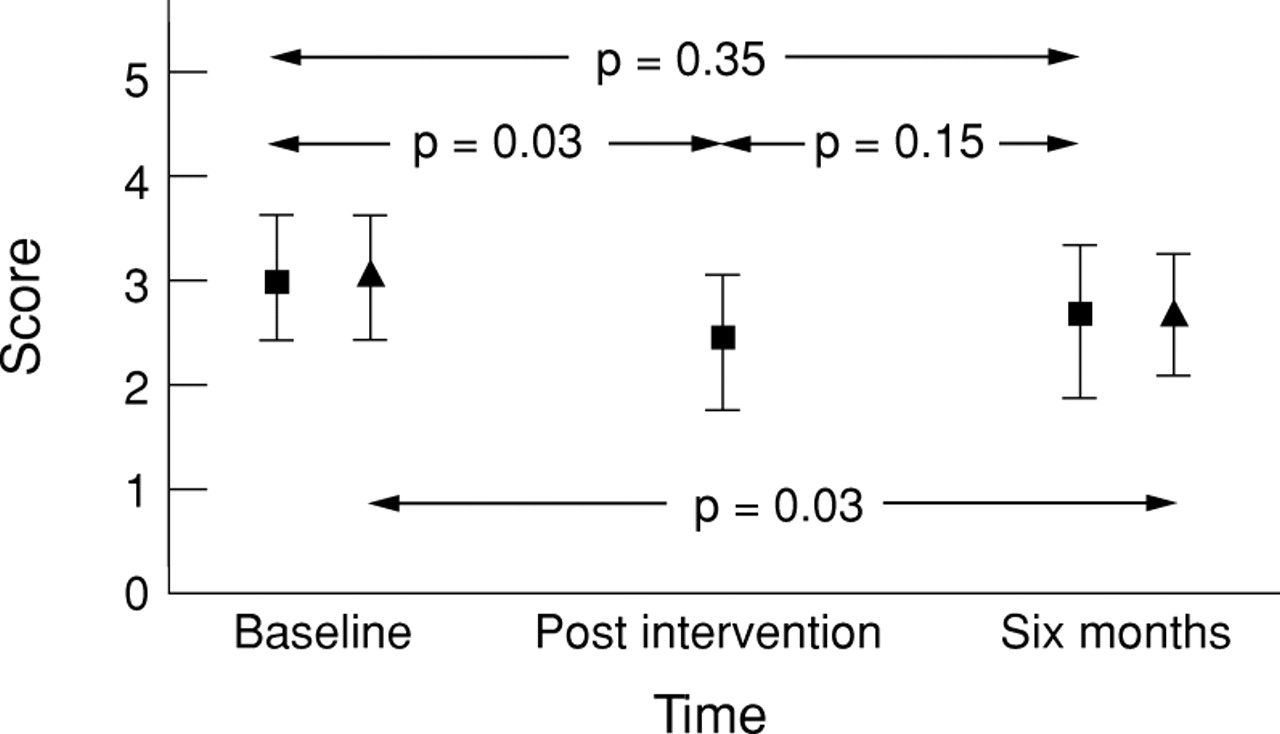
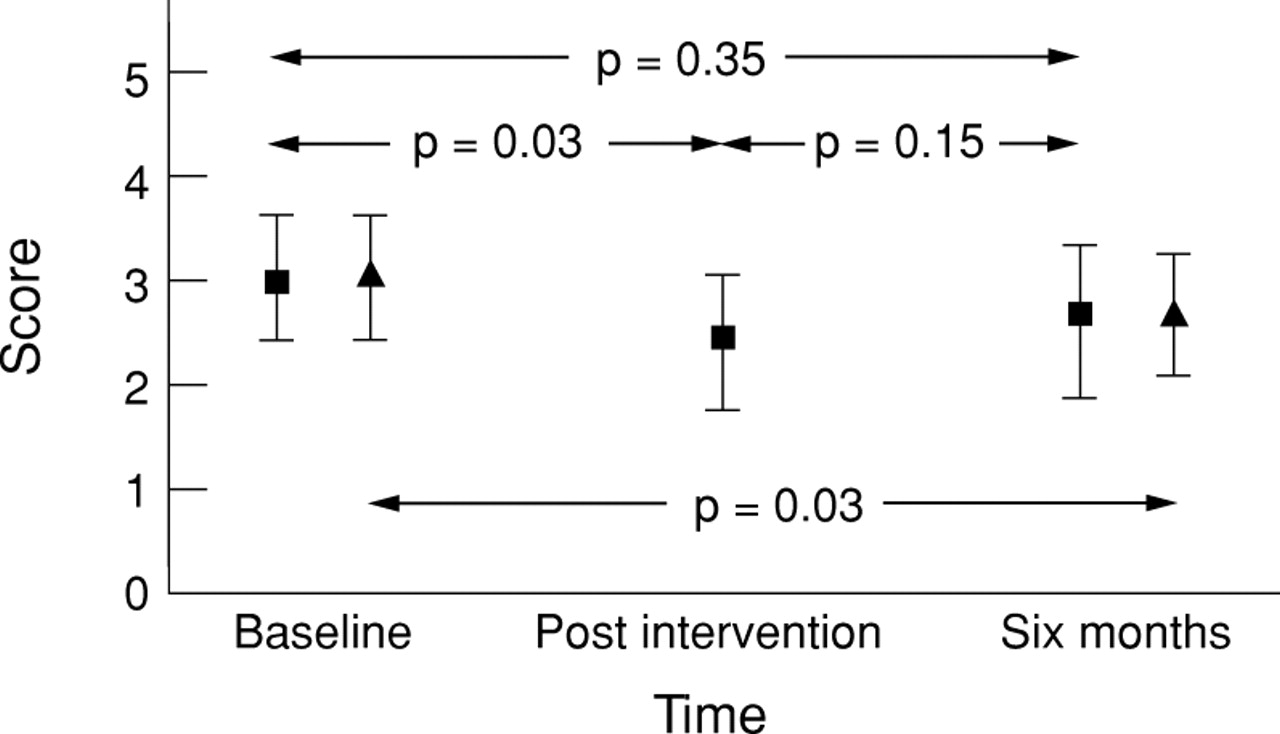
The impact of asthma on the total quality of life and subscales among subjects immediately after intervention, at six months, and the changes that occurred are presented in table 5. The main findings of the impact of asthma on total quality of life are summarised in fig 2. As at baseline, asthma had the greatest impact on the breathlessness subscale and the least impact on the social disruption subscale in both groups six months later (table 5). Total asthma quality of life, social disruption, and concern for health subscales improved significantly following the intervention (p = 0.03, p = 0.01, p = 0.002, respectively) but subsequently declined so that after six months there were no significant differences between intervention and control groups (table 5). Furthermore, there was a significant improvement in total quality of life in the control group at the six month follow up (p = 0.03). Despite showing improvements, the impact of the intervention on the breathlessness and mood disturbance subscales of quality of life was not significant.
Total quality of life and subscales of quality of life scores for the intervention and control groups after education
{kind=link}
{kind=link}
Effect of intervention on total quality of life (score out of 10 and 95% CI for mean); ■ = intervention group, ▴ = controls.
Self-management skills
Table 6 shows the median scores for the slow and rapid onset scenarios and the changes that occurred following intervention. Despite improvements in both the slow and rapid onset scores in the intervention group, the improvement was only significant for the rapid onset score immediately after intervention (p = 0.04). On the other hand, the control group improved significantly in their slow onset asthma attack scenario score (p = 0.02) at six months, but the difference from the intervention group was not significant (p = 0.48).
Self management skill scores for the intervention group after education and control group after 6 months
Attitudes and beliefs about asthma
There was an increase in the proportion of patients with asthma who were “not angry” about their condition in the intervention group from 50% to 53% immediately after intervention and 73% at six months. However, the final increase was not significant and at six months this just failed to reach statistical significance (p = 0.058). The proportion of patients who were “not angry” fell in the control group from 62% to 53%, but the change was not significant either. However, the difference in change at six months within groups was in favour of the intervention group (p = 0.049).
There was no significant improvement in the proportion of patients who were “optimistic” about their asthma getting better following the intervention. Despite a slight increase in the proportion of patients who were optimistic immediately after intervention from 64% to 68%, the difference was not significant. At six months there was a significant decrease in the proportion of patients feeling “optimistic” about their asthma outcome to 37% in the intervention group (p = 0.001) and 51% in the control group (p = 0.03). The difference in change from baseline to six months between the groups was not significant (p = 0.88).
The effect of the intervention on patients’ perceived ability to prevent an asthma attack was modest. There was an improvement in the proportion of subjects who felt they could prevent an asthma attack in the intervention group from 50% to 62% immediately following the intervention (p = 0.052). At six months the proportion of subjects in both groups who felt they could prevent an asthma attack had decreased but not significantly so (from 50% to 47% in the intervention group and from 65% to 51% in the control group). The difference in change from baseline to six months between the groups was not significant (p = 0.48).
Discussion
We have assessed the effectiveness of an asthma educational intervention on patients attending an outpatient clinic. Patients’ asthma knowledge, total quality of life, social disruption, concern for health, and self-management skills could be improved short term by the intervention, but not for long. By six months knowledge in the intervention group, although remaining significantly higher than baseline, was no different from the control group. Similarly, the improvements seen in quality of life and self-management skills for the rapid onset asthma attack were not retained. The intervention had very little impact on attitudes and beliefs about asthma.
In the absence of any intervention, the control group increased their asthma knowledge, total quality of life, and self-management skills for slow onset asthma attacks. This finding is consistent with the report by Snyder et al 24 that “waiting list controls increased their knowledge of asthma without any intervention other than the periodic filling out of questionnaires.” In their opinion, “asking an asthmatic about asthma improves his awareness and, correspondingly, his understanding of the disorder.” A further possible explanation for this finding in the present study was that the six month questionnaires were mailed to patients’ home addresses while the baseline questionnaires were administered at the clinic. Since the evaluation of the effectiveness of the intervention was entirely based on questionnaires, it was difficult to be confident that the six month questionnaires were completed by subjects unaided. A third possible reason could be that the subjects in the intervention group were recalled sooner to the programme than the control group. As a result of the delay, the control group could have been exposed to more in the way of general asthma education initiatives in the community or experienced a change in attention to education in the clinic as a result of increased awareness due to a study taking place.
This study was able to reproduce what had previously been reported by controlled studies—namely, that educational programmes can increase patients’ knowledge of asthma.11 ,24 ,25 Whilst there was a short lived significant improvement in quality of life among the educated group following the intervention, overall there was no significant change, as reported previously.25 Likewise, the intervention had only a brief but significant impact on self-management skills, at least for asthma attacks of rapid onset, which is also consistent with previous reports.11 ,12 ,25Attitudes and beliefs about asthma did not change and there was no difference between the two groups at follow up, as reported in other controlled trials.26 ,27 Maes and Schlosser26concluded that “there were no significant intervention effects on the cognitive attitude variables such as optimism, locus of control and shame or stigma”. Furthermore, the Grampian Asthma Study of Integrated Care27 found no significant difference in psychological outcomes such as anxiety, depression, self-efficacy, or social and physical functioning between groups.
The impact of asthma on the quality of life of subjects in this study was moderate. Comparison with other studies is difficult to make as there are no published controlled studies that have used this particular asthma quality of life questionnaire. However, the same questionnaire has been previously used in a few observational studies in Australia. Marks et al 28 in a population based cross sectional study of 98 adults with asthma reported a median AQLQ score of 1.0 (IQR 0.6–1.8) out of a possible score of 10. Unlike subjects in the present study, most of their subjects had mild asthma. Rassaby29 also conducted a cross sectional study of 130 adults with asthma who were purchasing asthma medications from community pharmacies in Melbourne and found a median AQLQ score among the subjects of 2.13 (IQR 1.28–3.75). Unlike subjects in the present study, only 50% of her sample had ever been to a hospital emergency department for their asthma.
The self-management scenarios have not been extensively used in the past. Kolbe et al 19 modified the scenarios for similar patients with moderate to severe asthma who were attending a hospital clinic in Auckland, New Zealand. The mean scores (out of a possible 25) for their subjects were 12.8 and 13.9 for the slow and the rapid onset attacks, respectively. Despite a difference in maximum possible scores between the two studies, patients in the present study scored higher than the New Zealand patients in asthma attacks of both slow and rapid onset as a proportion of the total score, even at baseline.
The study sample was likely to be representative of adult patients who were attending a tertiary hospital outpatient clinic. The randomisation procedure ensured that both groups were well matched at baseline, except in one item of attitudes and beliefs about asthma. Despite having a flexible timetable and format, a significant number of patients who had expressed interest failed to attend. There were no significant differences at baseline between participants and non-participants in the programme in any of the clinical parameters. Age and group allocation were the only significant predictors of attendance.23 The participation of patients in this hospital based education programme was poor. Of 64 subjects allocated to the intervention group who had expressed interest, 30 (47%) of them did not attend the programme. Of 61 subjects in the control group who completed the baseline questionnaires, 14 (23%) of them did not complete the six month follow up questionnaires. The reasons for non-response among the control subjects included lack of interest and loss to follow up. Among subjects who expressed lack of interest, telephone calls and three mail reminders failed to improve the response rate. To achieve this modest participation rate every attempt was made to encourage patients in the intervention group to attend the education sessions. Such measures included an offer of incentives (free information package and peak flow meter) and conducting the sessions at subjects’ preferred times. The reasons for the low participation rate remain unclear. Perhaps patients were not sufficiently interested and consequently did not value the usefulness of the educational programme highly enough. More research is needed to understand why patients do not attend hospital based asthma education programmes.
Although there was a substantial drop out rate, with sample sizes of 30 and 47 in the intervention and control groups, respectively, the study still had 80% power to detect a difference between the two groups of 2.8 in their change in knowledge scores.
The results of this study indicated that an intervention programme directed at adults with asthma attending an outpatient clinic had a positive impact on patients’ knowledge of asthma, but did not bring about lasting changes in quality of life, self-management skills, or attitudes. Limited benefit was associated with three education sessions each lasting 1.5 hours. This is consistent with a systematic review of adult asthma education in the context of the Australian Asthma Management Plan by Gibson and co-workers.30 They concluded that limited education did not have an impact on hospital admissions, doctor visits, lung function, medication use, or asthma symptoms. In their opinion, limited information based education alone was unlikely to improve health outcomes, but could be beneficial to some extent for people with severe asthma attending emergency rooms. Thus, there is no strong evidence that knowledge alone can lead to better asthma management practices or asthma control. Most importantly, limited education is unlikely to have a positive impact on behaviour, self-management skills, or “hard” health outcomes such as hospital admissions. For patient education to achieve its goal it has to be provided in a format with close involvement of both physicians and nurses. To achieve significant improvements in quality of life and self-management skills of patients with moderate to severe asthma will require coordinated ongoing education and support, and these parameters cannot be sufficiently influenced by a brief intervention programme. However, some past studies have shown that a relatively brief instruction in self-management techniques can reduce emergency room visits, days off work,31 asthma morbidity, utilisation of medical services,32 and subsequent admissions to hospital.33
In conclusion, we acknowledge that although 64 subjects were allocated to the intervention group, 30 (47%) of them did not attend the programme. There was no reason to recruit patients from outside the clinic. Asthmatic subjects attending a hospital outpatient clinic differ in severity from those presenting to other settings such as general practice. Our findings should therefore only be generalised to hospital patients with moderate to severe asthma, and the applicability of this intervention outside the clinic is limited. As data were not obtained from the control group immediately after intervention, the two groups could not be compared at this time. Knowledge alone may not be the first step in patient education and does not necessarily lead to behavioural change. The primary focus of patient education and asthma management strategies should be to identify negative behaviours and work towards positive behavioural changes. Such a strategy can help patients to seek more knowledge to consolidate their behaviour relevant to good asthma management. The role and usefulness of alternative models in educational programmes should be explored in order to address key management problems such as poor compliance with medication. Thus, future programmes should focus on broad behavioural change and not only on improving patients’ knowledge about asthma. The challenge for patient education is to come up with a better strategy to address patients’ behaviour in a systematic way. This may involve a more comprehensive assessment of factors associated with patients’ social and asthma management strategies.
Acknowledgments
The authors acknowledge the financial support of the National Health and Medical Research Council of Australia. Allersearch donated peak flow meters, and Glaxo (Allen & Hanburys), Astra, the Asthma Foundation of Victoria and the National Asthma Campaign provided educational materials. Claire Walton and Gina Karamountzos conducted some of the sessions. The authors also thank Associate Professor Daniel Czarny, Dr Frank Thien, Dr Larry Light and the staff of the Alfred Hospital Asthma and Allergy Clinic for their support and Dr Guy Marks, Rae Allen and Bonnie Sibbald for permission to use their questionnaires. Dr John Kolbe gave permission to use his scoring system for the asthma attack scenarios.