Article Text

Abstract
Background and purpose Long obstructive sleep apnoeas (LOSAs) can cause brain ischaemia through paradoxical embolism since they can lead to right to left shunting (RLSh) but this has never been assessed as a risk factor for stroke. We investigated whether the combination of LOSA and RLSh is associated with ischaemic stroke or transient ischaemic attack (TIA) on waking (wake-up stroke).
Methods We prospectively considered patients aged over 18 years, admitted to 13 stroke units for acute ischaemic stroke or TIA. Patients had to be able to give consent, to specify whether the event occurred on waking, and to cooperate sufficiently to undergo contrast transcranial Doppler examination and cardiorespiratory sleep study within 10 days of the onset of symptoms. Single LOSA events, lasting 20 s or more, were considered a possible harbinger of RLSh.
Results Between April 2008 and March 2010, 335 patients (109 women; 61 TIA, mean age 64 years) were enrolled; 202 (60%) had at least one LOSA and 116 (35%) a RLSh; 69 (21%) had both. There were significantly more wake-up strokes/TIAs in subjects with RLSh plus LOSA than those without this association (27/69 vs 70/266; OR 1.91, controlled for age, sex, hypertension, diabetes, atrial fibrillation, antithrombotic therapy; 95% CI 1.08 to 3.38; p=0.03). No other risk factor was associated with an increase in the incidence of events on waking.
Conclusions The study suggests that the combination of LOSA and RLSh could be a new major, potentially treatable risk factor for cerebrovascular ischaemic events.
- Sleep apnoea
Statistics from Altmetric.com
Key messages
What is the key question?
-
Does the combination of right to left shunt (RLSh) and obstructive sleep apnoea (OSA) raise the risk of wake-up stroke?
What is the bottom line?
-
The probability of detecting the association of long OSA with RLSh is significantly higher (OR 1.91; 95% CI 1.08 to 3.38) in patients with wake-up stroke and TIA than in patients with stroke or TIA while awake.
Why read on?
-
To realise a new potential treatable risk factor for ischaemic cerebrovascular events.
Introduction
Although ischaemic stroke is one of the leading causes of death and long-term disability worldwide, routine diagnostic testing does not clarify its cause in about 30% of patients.1 A right to left blood shunt (RLSh) is considered a potential cause of paradoxical brain embolism and is mostly associated with a patent foramen ovale (PFO). Usually, the higher left atrium pressure keeps the PFO closed but in certain conditions that affect intrathoracic pressure and cardiopulmonary haemodynamics (eg, weight lifting, straining, vomiting, sexual intercourse, coughing) a RLSh can occur2 allowing clots formed in the venous system to pass into the arterial system. Although PFO is very common, the condition triggering a RLSh just before the stroke is frequently missed2 and an embolic venous source is rarely found unless the search for venous thrombosis is done extensively early after stroke.3 ,4 Consequently, it is often not clear whether a PFO in a patient with stroke should be considered the primary cause of the event or an incidental finding.5 Obstructive sleep apnoea (OSA), provoked by occlusion of the upper respiratory airways during sleep, is one of the missed conditions that might result in a RLSh. During an OSA event, there is transient elevation of right-sided pressures which, in the presence of a PFO, may cause a RLSh if the apnoea lasts long enough (more than 17 s).6 ,7 The possibility of paradoxical embolism during OSA has been considered in single cases8 but has never been assessed as a risk factor for stroke.9 The present study was specifically designed as a cross-sectional study to investigate whether the combination of RLSh and OSA events is associated with the risk of wake-up stroke.
Methods
Study design and participants
We analysed a series of patients admitted to 13 different stroke units. Patients were eligible if they were older than 18, had a definite clinical diagnosis of acute ischaemic stroke (stroke was defined as any acute focal cerebral event with symptoms lasting at least 24 h) or transient ischaemic attack (TIA, ie, any acute focal cerebral ischaemic event with symptoms lasting less than 24 h) occurring on waking or while awake, could undergo a cardiorespiratory sleep study and cooperate during contrast transcranial Doppler sonography (cTCD) within 10 days of the onset of symptoms. If cTCD was not feasible (eg, when the acoustic temporal bone window was lacking), RLSh could be investigated with contrast trans-esophageal echocardiography (cTEE). A cerebral CT scan or MRI was required to exclude patients who had an intracranial haemorrhage.
Centres participated on a voluntary basis and were asked to enrol patients consecutively, even during short periods of time, in the 2 years of the study, depending on the availability of personnel and services (many centres, for instance, were not able to enrol patients during weekends, bank holidays or some periods of the year). All patients gave written informed consent before enrolment. The study was approved by the ethics committees of the coordinating centre (Niguarda Hospital) and the other centres.
Information collected
We recorded the following data for all patients: age, sex, body mass index, neck circumference, oral anatomy according to Mallampati,10 atrial fibrillation (documented by ECG), history of hypertension (systolic blood pressure ≥135 mm Hg and/or diastolic ≥85 mm Hg), diabetes (fasting serum glucose >127 mg/ml), hypercholesterolaemia (total cholesterol ≥190 mg/dl), family history of coronary artery disease (father died of myocardial infarction at age <55 years and/or mother at <65 years), smoking (number of cigarettes/day and duration of smoking),11 ,12 previous strokes, TIA or myocardial infarction, chronic therapies in use at the moment of the index event.
Neurological deficit was evaluated the day of the cardiorespiratory sleep study, using the National Institutes of Health Stroke Scale (NIHSS)13 by examiners trained and certified in its use. Vascular syndromes were classified on the basis of the clinical presentation at the onset of symptoms, according to the Oxfordshire Community Stroke Project (OCSP),14 as lacunar syndrome (LACS), posterior circulation syndrome (POCS), total anterior circulation syndrome (TACS) or partial anterior circulation syndrome (PACS).
Specific examinations
All patients underwent a cardiorespiratory sleep investigation to confirm the presence of OSA, and cTCD or cTEE for the detection of RLSh.
Cardiorespiratory sleep study
The presence of a sleep breathing disorder (SBD) was assessed using a portable monitoring device in the ward in an attended setting, in conjunction with a comprehensive sleep evaluation.15 ,16 All the study centres used the same cardiorespiratory sleep recorder (Embletta, Embla, The Netherlands). Nasal air flow, chest and abdominal effort, pulse oximetry, snoring, heart rate and body position during sleep were continuously recorded. Data were analysed using the Somnologica for Embletta software (Medcare, Embla), and manually reviewed by a medical doctor specialised in sleep medicine, certified by the Italian Association of Sleep Medicine. Respiratory events were scored according to current standard criteria.17 Besides conventional indexes expressing the number of respiratory events per hour (aponea-hypopnoea index—AHI, obstructive apnoea index, central apnoea index, mixed apnoea index, hypopnoea index, oxygen desaturation index), we also recorded the number of OSA events lasting 20 s or more (long OSAs (LOSAs)).
Contrast transcranial Doppler sonography
cTCD to detect RLSh was done in awake patients following a standardised protocol18: an 18-gauge needle was placed in the cubital vein with the patient supine and at least one middle cerebral artery (MCA) was insonated using TCD. The contrast agent was prepared using 9 ml isotonic saline solution and 1 ml air mixed with a three-way stopcock by exchanging the saline–air mixture between the syringes, and injected as a bolus. If few or no microbubbles (MB) were detected in the MCA under basal conditions, the examination was repeated using the Valsalva manoeuvre (VM). Contrast agent was injected 5 s before starting the manoeuvre, which lasted 10 s. A four-level classification was used to describe the RLSh, depending on the MB count: (1) 0 MB (negative); (2) 1–10 MB; (3) >10 MB and no curtain; and (4) curtain. ‘Curtain’ refers to a shower of MB, where no single bubble can be identified. The test was done separately in basal conditions and during the VM.
Contrast trans-esophageal echocardiography
cTEE was done at rest and under the VM with the patient in the left lateral decubitus position, after topical anaesthesia (lidocaine) of the pharynx. The fossa ovalis area was imaged in multiple planes. At least three contrast injections (agitated saline) were given into an antecubital vein, accompanied in at least one instance by a VM. RLSh was diagnosed if the right to left passage of at least 1 MB was observed within three cardiac cycles after opacification of the right atrium.19
Index event and risk factor definition
Wake-up stroke or TIA
The onset of symptoms of the index event (ischaemic stroke or TIA) was carefully assessed by questioning the patient and any witness, to ascertain whether it was noted on waking or when already awake. In the former case, the index event was classified as ‘wake-up stroke’, and in the latter as ‘stroke while awake’. When symptoms were noted on waking, the onset of TIA or stroke was conventionally considered the time at which the subject fell asleep, so a wake-up TIA was defined as such when the time elapsed from falling asleep to resolution of symptoms was less than 24 h. This categorisation was done by a neurologist working in the stroke unit and data were blinded with respect to sleep study results.
Right to left shunting
RLSh was considered present when either cTCD or cTEE detected at least one MB under basal conditions or using the VM.
Long obstructive sleep apnoea
LOSA was considered present when at least one episode of obstructive apnoea lasted 20 s or more.
Risk factor
The coexistence of LOSA plus RLSh was considered the risk factor for wake-up stroke or TIA; the absence of one or both these conditions was considered as absence of the risk factor.
Sample size
We planned the study of independent cases (wake-up stroke or TIA) and controls (stroke or TIA while awake) with three controls per case, assuming a 0.25 proportion of wake-up stroke/TIA in a series of patients admitted to stroke units.20 ,21 We assumed that the probability of exposure to OSA plus RLSh among controls was 0.23 on the basis of prior data indicating a prevalence of about 0.5 of OSA among stroke patients 22 and a prevalence of about 0.45 of RLSh among those with OSA.23–25 Setting the true probability of exposure among cases to 0.4 and the probability of a type I error <0.05, 332 patients (83 cases and 249 controls) gave 0.8 power to detect the expected difference in proportion using a two-sided Pearson's χ² test with Yates’ correction for continuity.
Statistics
All data were checked and validated on the basis of the rules we had established, then analysed with suitable descriptive methods. General clinical data for patients with RLSh plus LOSA and patients without the association were compared with Fisher's exact text (binomial variables) and Mann-Whitney U test (continuous variables).
Inferential analysis was done using the wake-up stroke as the primary endpoint. Comparisons by cross-tabulation were done with Pearson's χ² test and calculating the Mantel-Haenszel OR and its 95% CI. Logistic regression was used in univariate analysis to assess the effects of continuous and categorical variables on the endpoint. Multivariate analysis was done to adjust the effect size of these variables for potential confounding effects of general risk factors for stroke and possible clinical differences between patients with RLSh plus LOSA and patients without the association. The results of statistical tests were considered significant for p <0.05. All analyses were done using the Stata/SE V.11.1 statistical package.
Results
Patients
Between 1 April 2008 and 1 April 2010, centres consecutively enrolled patients for a mean of 5.9 months (range 2–15 months). During this period 1560 patients were admitted to the stroke units for TIA or ischaemic stroke (figure 1). About 76% of patients (1183 patients) were not eligible because they were not able to collaborate, refused to participate or it was not clear whether the symptom onset was on waking or not. Among the eligible patients, 47 were excluded because the RLSh (cTCD/cTEE with VM unreliable or not feasible, n=24) and/or OSA (cardiorespiratory sleep monitoring not feasible or not correctly interpretable because of technical problems, n=23) were not assessed, meaning they could not be assigned to either of the two categories (with or without the RLSh–LOSA association). Therefore, 335 patients were analysed; 61 (18%) had a TIA and 274 (82%) an ischaemic stroke. The mean NIHSS score on the day of the cardiorespiratory sleep study was 3.0 (±3.7). The index event happened on waking in 97 patients (29%). General clinical features and the proportions of index event (TIA or stroke) were not significantly different in patients with RLSh plus LOSA with respect to those without the association. As regards the OCSP classification of index events, POCS were significantly higher (p=0.029) in patients with RLSh plus LOSA while LACS prevailed (p=0.016) in patients without the association (table 1).
Patients’ main clinical findings

Consort diagram. *Each centre enrolled patients consecutively, although for a short period (mean 6 months; range 2–15 months, see text).
The results of specific examinations are reported in table 2.
Results of specific examinations
AHI was more than 5 in 60% of cases; 202 (60%) patients had at least one LOSA and 37 of these (18%) had an AHI <5. In 12 patients the cTCD was not feasible or not assessable and RLSh was evaluated with the cTEE. A RLSh was detected in 116 patients (35%); 69 (21%) had a RLSh and at least one LOSA event.
Univariate analysis
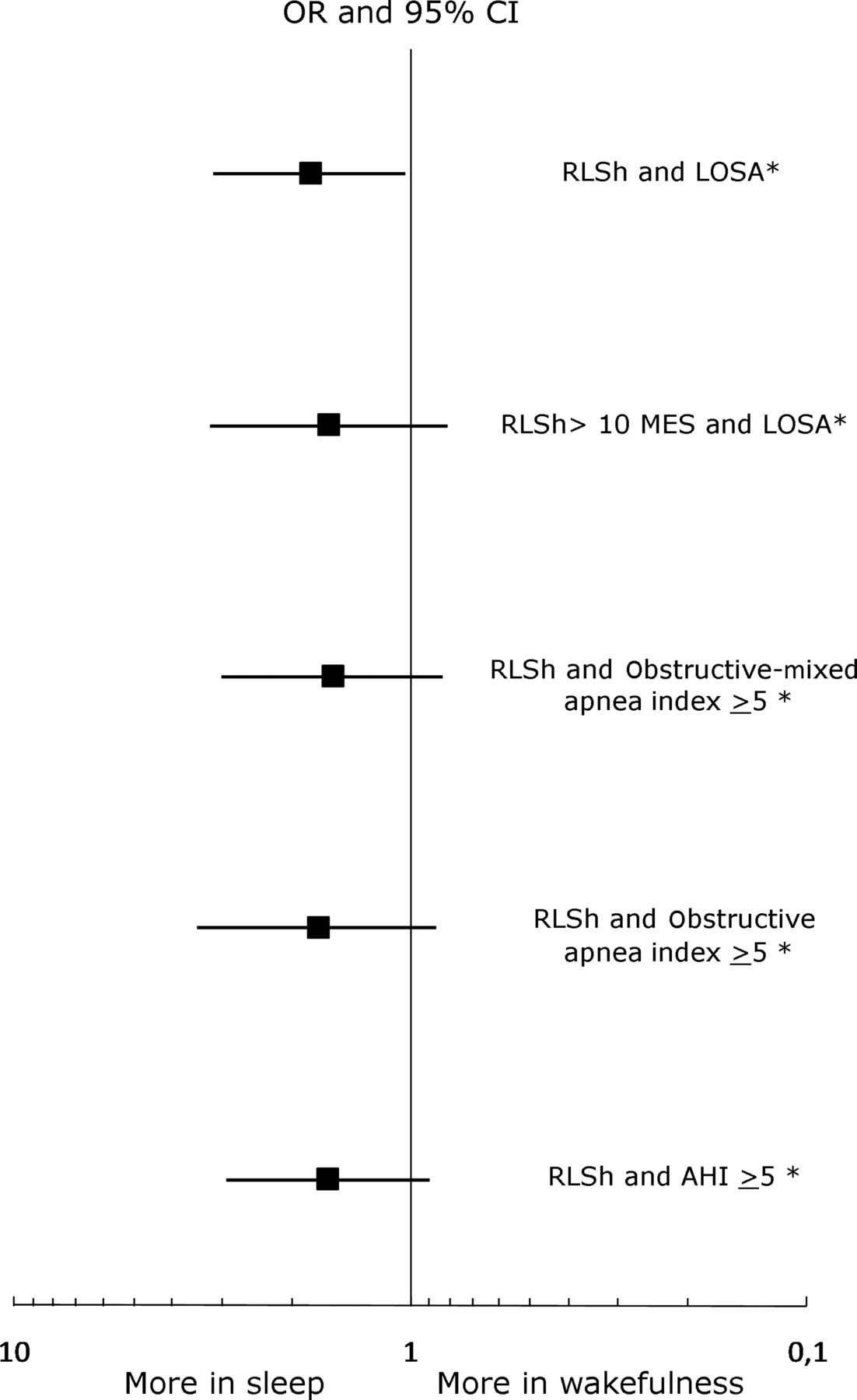
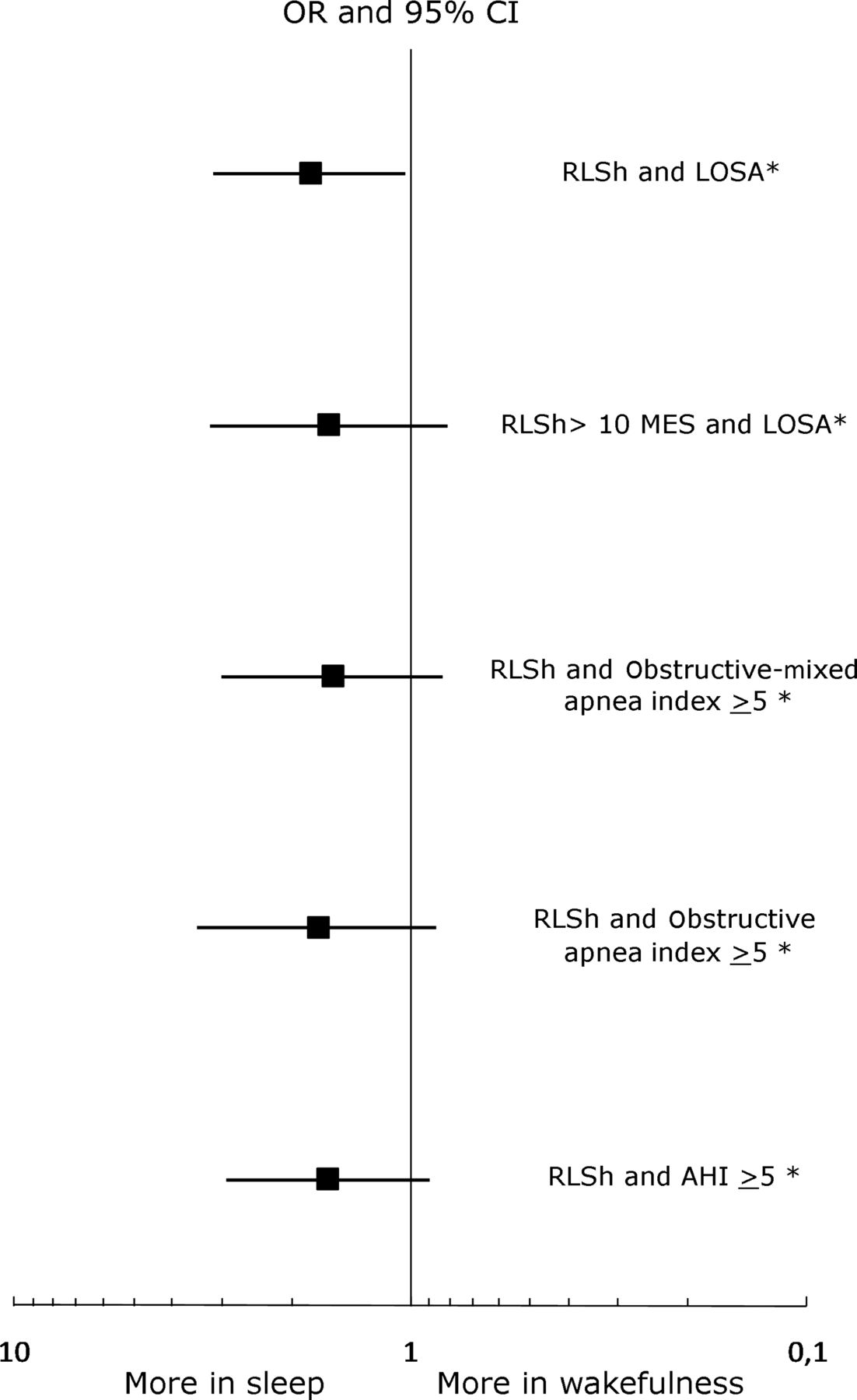
Univariate analysis found no single variable significantly associated with the event on waking (figure 2). The only variable significantly associated with the event on waking was the combination of LOSA plus RLSh (OR=1.8; CI 1.03 to 3.14) (figure 3, table 3). Univariate analysis of the combination of RLSh with other cardiorespiratory sleep study parameters confirmed that only RLSh plus LOSA significantly increased the risk of wake-up stroke (figure 3).

Results of univariate analysis. No single variable was significantly associated with the event on waking. AF, atrial fibrillation; AHI, apnoea-hypopnoea index; BMI, body mass index; F, female; LOSA, long obstructive sleep apnoea events lasting 20 s or more; M, male; N, no; NIHSS, National Institutes of Health Stroke Scale; ODI, oxygen desaturation index; RLSh, right to left shunt; SpO2, peripheral oxygen arterial saturation; Y, yes. *Per unit increase.
{kind=link}
{kind=link}
{kind=link}
Univariate analysis evaluating the combination of RLSh with different cardiorespiratory sleep study parameters. Only RLSh plus LOSA significantly increased the risk of wake-up stroke (OR=1.8; 95% CI 1.03 to 3.14). AHI, apnoea-hypopnoea index; RLSh, right to left shunt; RLSh>10MES, right to left shunt with more than 10 microbubbles. *Present or absent. LOSA, long obstructive sleep apnoea.
Frequency of the index event on waking in patients with and without the combination of RLSh and LOSA
Multivariate analysis
Considering the absence of baseline differences between patients with and without LOSA plus RLSh, we included general risk factors for stroke in the multivariate analysis.
After adjustment for hypertension, diabetes, sex, age, antithrombotic treatment (antiplatelet or anticoagulant therapy) and atrial fibrillation, the combination of RLSh with LOSA retained a significant association with the event on waking (OR=1.91; CI 1.08 to 3.38, table 4).
Adjusted OR for the risk of wake-up stroke
Discussion
The study's main finding is that the probability of detecting the association of LOSA plus RLSh is significantly higher (OR 1.91; CI 1.08 to 3.38) in patients with wake-up stroke and TIA than in patients with stroke or TIA while awake. No other risk factors were associated with a significant increase of neurological wake-up events. Therefore, the study hypothesis, based on the idea that LOSA is likely to cause paradoxical embolism through RLSh, has been confirmed. This was supported by a previous study looking at clinical clues to paradoxical embolism, which showed that wake-up stroke or TIA was more common in patients with RLSh and considered a possible relationship between OSA (whose presence was not assessed), RLSh and wake-up stroke.2 The internal consistency of the results was also supported by the greater frequency of posterior circulation stroke or TIA in patients with LOSA plus RLSh, in accordance with the higher frequency of posterior circulation involvement in case of paradoxical embolism.26 The chain of events, starting with a LOSA, that may lead to paradoxical embolism, includes a prolonged period of intra-thoracic pressure swings that sucks the blood into the right atrium, increasing venous pressure and forcing open a PFO or a pulmonary venous shunt.6 ,7 Different studies have shown progressive changes in ventricular size, pulsus paradoxus and a leftward shift of the interventricular septum related to the decrease in intra-thoracic pressure during OSA events.7 ,27 Therefore, monitoring the intra-pleural pressure during sleep would be important to quantify the respiratory effort, notably related to the haemodynamic changes,28 and to assess the physiopathological basis of our findings better.
The main inclusion criterion for our sample was that patients needed to be competent and collaborative enough to undergo a cTCD examination. As a result, the cohort mainly comprised patients with TIA and minor strokes, as reflected by the low median NIHSS and the small proportion with TACS. In fact we only enrolled a quarter of the entire population of TIA/stroke patients admitted to the stroke units. It is possible that the way we built the sample might affect the robustness of our results; however, the observed rates of wake-up events (29%), RLSh (35%) and SBD (60%), risk factors and stroke subtypes are consistent with those reported in other studies,20 ,21 ,26 ,29 ,30 and so we are confident in the reliability of our findings.
An acute stroke can cause or worsen a SBD, but in our study the LOSA events should be regarded as a cause not a consequence of the cerebrovascular accident since, as different reports have pointed out, an obstructive SBD in a patient with acute stroke usually precedes—not follows—the event as, instead, happens with sleep apnoeas of central origin.29 ,30 We focused on the OSA's duration rather than its frequency, on the basis of Beelke et al's findings.6 These authors observed that in patients with PFO an OSA event longer than 17 s was provocative of RLSh, whereas no RLSh was found in normal sleep breathing, during obstructive hypopneas or in shorter OSA. Conservatively, we took as an endpoint OSA events lasting longer than 20 s (LOSAs).
The suspicion of paradoxical embolism implies a venous source. We did not examine this as our main aim was to quantify the combination of RLSh plus LOSA as a risk factor for wake-up cerebrovascular events; however, OSA might by itself be a risk factor for venous thrombosis.31 It may have a significant effect on the mechanisms known as Virchow's triad, leading to venous stasis, altering coagulability and impairing endothelial function.32 The role of OSA as an independent risk factor for pulmonary embolism was recently suggested by Epstein et al who found a higher prevalence of snoring and higher risk of OSA in patients with acute pulmonary embolism than in patients in whom pulmonary embolism had been suspected but then ruled out.32 Interestingly, the proportion of men was not significantly higher in the LOSA plus RLSh group compared with the LOSA or RLSh or neither group, as one would expect. This might be consistent with findings obtained in a case–control study of patients with deep vein thrombosis/pulmonary embolism, in which the association of sleep apnoea and deep vein thrombosis was much stronger in women than in men.33 Further studies aimed at confirming the role of OSA as a risk factor for paradoxical embolism in patients with PFO should also check for venous thrombosis in the legs3 and pelvis.4
We quantified the presence of RLSh but did not systematically document the parallel presence of a PFO by cTEE. A cTCD by itself does not reveal the anatomic origin of the RLSh, which might be pulmonary or cardiac. The prevalence of pulmonary arteriovenous fistulas, the cause of pulmonary shunt, is not known but pulmonary RLShs is reported in up to 20% of patients with RLSh and stroke34 and 21–27% of RLSh identified with cTCD are not confirmed by cTEE,35 ,36 suggesting that at least some are pulmonary. Since paradoxical embolism during OSA events through a pulmonary rather than cardiac RLSh should be considered, cTCD assessment of RLSh, regardless of the anatomic origin of the shunt, seemed more appropriate and comprehensive for the purpose of our study. Further studies of the RLSh origin are needed, with a view to testing different therapeutic options.
Previous studies have shown that sleep apnoea is an independent risk factor for ischaemic stroke through different longstanding mechanisms.9 After adjustment for these pathogenic mechanisms in the multivariate model, the association of RLSh-LOSA retained a significant association with wake-up stroke, indicating that the combination could act as a precipitating, acute factor favouring a cerebrovascular ischaemic event on waking through a cardio-embolic mechanism.
In the univariate model the variable hypertension was almost significantly associated with wake-up stroke. Indeed, the inclusion of nocturnal blood pressure as an additional control variable might have raised the magnitude of this association; unfortunately, we did not systematically collect nocturnal blood pressure and we do not have sufficient information about the possible presence of a non-dipping blood pressure profile in subjects with a wake-up stroke.
Wake-up stroke is a clinical entity that comprises a significant proportion of all ischaemic strokes20 ,21 but its correlation with clinical features, stroke risk factors and stroke classification are still not conclusive.20 ,37 ,38 Our findings could be useful for a preventive and therapeutic strategy. The data suggest that patients with wake-up stroke should be screened for sleep apnoea and RLSh and, when both are found, also for deep vein thrombosis.
A recent randomised controlled trial showed that in patients with PFO and cryptogenic stroke or TIA, PFO closure did not offer a greater benefit than medical therapy alone for the prevention of recurrent stroke or TIA.39 However, as the authors stated, these results do not preclude a possible role for closure of a PFO in highly selected patient populations. Our data seem to identify a potential group of patients in whom the effect of PFO closure could be usefully investigated.
In conclusion, this study, suggesting that LOSA events raise the risk of wake-up stroke in patients with RLSh, supports the hypothesis that long episodes of OSAs can induce paradoxical embolism.
Should this be confirmed in future studies, it would add knowledge to the mystery of wake-up stroke and cryptogenic strokes and could have important implications for a different approach to the treatment of patients with OSA and PFO.
Acknowledgments
Sapio-Life provided all centres with the respiratory analyser Embletta and Somnologica for Embletta software. The statistical analysis was conducted by Dr Michele Nichelatti, Biostatistics Service, Hematology Department, ‘Niguarda Ca’ Granda’ Hospital, Milan, Italy.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix
Footnotes
-
Contributors AC and LN conceived and wrote most of this manuscript, which was checked and discussed with the other authors who approved the final version. DVR and PP were the clinical monitors and data managers of the D.A.RI.A. study. MN did the statistical analysis.
-
Competing interests All authors have completed the unified competing interest form at http://www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous 3 years; no other relationships or activities that could appear to have influenced the submitted work.
-
Ethics approval Ethic committees of each participant hospital.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Correction