Article Text

Abstract
Individuals with pulmonary arteriovenous malformations (PAVMs) and hereditary haemorrhagic telangiectasia (HHT) commonly have low oxygen saturations and anaemia, two parameters generally used to indicate medical fitness to fly. Using a retrospective questionnaire-based study, the authors examined in-flight complications and predictors in 145 HHT patients (96 with PAVMs) who reported 3950 flights, totalling 18 943 flight hours. Dyspnoea and thrombotic complications were less common than expected, and could not be predicted from sea level oxygen saturations or haemoglobin concentrations. Nosebleeds that can bar individuals from boarding a flight occurred in 13.6% (11.5% to 15.8%) of long-haul flights. The findings should influence preflight advice.
- Hypoxaemia
- nosebleeds
- oxygen
- stroke
- thrombosis
- pulmonary embolism
- rare lung diseases
- asthma
- bronchiectasis
- COPD pharmacology
- cystic fibrosis
Statistics from Altmetric.com
- Hypoxaemia
- nosebleeds
- oxygen
- stroke
- thrombosis
- pulmonary embolism
- rare lung diseases
- asthma
- bronchiectasis
- COPD pharmacology
- cystic fibrosis
Individuals with pulmonary arteriovenous malformations (PAVMs)1 and hereditary haemorrhagic telangiectasia (HHT)2 commonly have low oxygen saturations and anaemia, parameters that are used in the general population to indicate medical fitness to fly3–5 (and online supplementary references). There are very limited published data on flight tolerance for HHT/PAVM patients.
Using the retrospective study methodology reported in full in the online supplementary material, we received 159 replies from 308 questionnaires sent out to individuals with definite HHT (response rate 51.6%). The average age at the time of reply was 55 years (range 18–90), 12 respondents had not flown and two (pilot and cabin crew) reported more than 10 000 flights. The remaining 145 HHT-affected respondents (96 (66%) with PAVMs) reported 18 943 flight hours over 3950 flights (online supplementary table 1).
The majority (111/145; 77% (95% CI 69.6% to 83.5%)) reported no in-flight or postflight complications. Six (4.1% (0.86% to 7.4%)) reported dyspnoea, two had a deep vein thrombosis and one suffered an ischaemic stroke while flying. The most common in-flight complications were HHT-related nosebleeds (epistaxis). Complications were more frequent during long-haul flights. Many participants listed flights over several decades, but none reported an increase in the frequency or severity of complications as they got older.
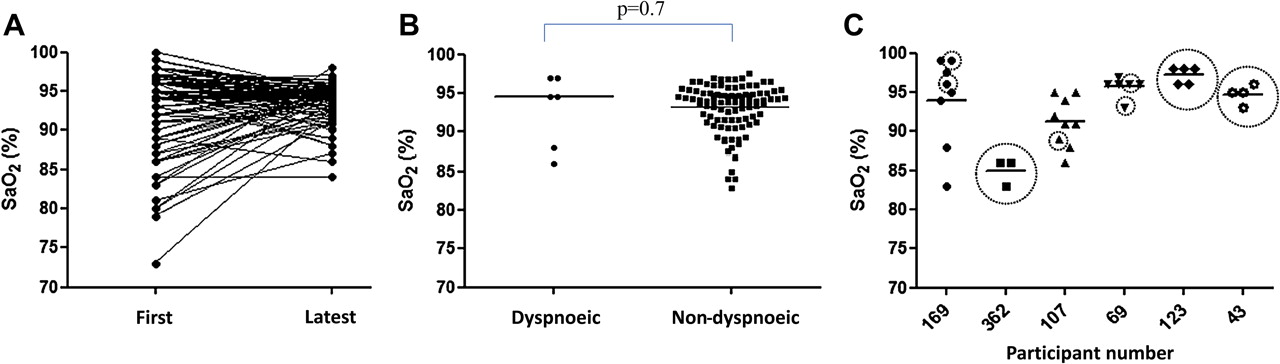
For participants with PAVMs who had not reported in-flight dyspnoea, there was a wide range in arterial oxygen saturation (SaO2) levels (figure 1A). There was no difference in median SaO2 between those who reported in-flight dyspnoea and those who did not (figure 1B). Flights where dyspnoea was reported did not correspond to times when SaO2 were lowest for that particular individual (figure 1C). Similarly, there appeared to be no relationship between dyspnoea and either haemoglobin or serum iron (online supplementary figure 1). There was also no relationship between thrombotic complications and oxygen saturations/haemoglobin (online supplementary figure 2) or between in-flight nosebleeds and basal nosebleeds frequency (if at least once per month) or haemoglobin (online supplementary figure 3).

{kind=link}
Sea level oxygen saturation in 96 participants who flew with pulmonary arteriovenous malformations (PAVMs). (A) Earliest and most recent arterial oxygen saturation (SaO2) values for PAVM patients who did not report in-flight dyspnoea (improvements were the result of PAVM embolisation). (B) Mean erect oxygen saturations (SaO2) at sea level for individuals who reported in-flight dyspnoea and those who did not. Horizontal bars denote medians. There was also no difference in earliest or latest SaO2 (data not shown). (C) Serial SaO2 in participants who reported dyspnoea over periods of 1–17 years (median 7.5). Circles indicate periods in which flights were reported to cause dyspnoea. The flight causing dyspnoea for participant 107 was the only long-haul flight taken by that individual.
In conclusion, and as discussed in more detail in the online supplementary material, the principal findings of this study were that flying appears safe for the majority of individuals with PAVMs and HHT despite abnormal oxygen saturations and haemoglobin concentrations. With the exception of nosebleeds, complications, when they occurred, were usually self-limiting. It was difficult to predict who will experience complications, with the best predictor appearing to be previous flight experience. The findings are surprising, and raise difficulties in recommendations for in-flight oxygen and prophylaxis of venous thromboemboli.
Acknowledgments
The authors thank Dr Andrew Cummin, Dr Robina Coker and Professor JMB Hughes for manuscript review and helpful comments.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Download Supplementary Data (PDF) - Manuscript file of format pdf
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Download Supplementary Data (PDF) - Manuscript file of format pdf
Footnotes
Both authors had full access to all of the data in the study, and take responsibility for the integrity of the data and the accuracy of the data analysis.
Funding This work was performed as part of an NIHR Academic FY2 post (CGM). CLS is also grateful for support from the Imperial NIHR Biomedical Research Centre Funding Scheme. The funders had no part in the study design; in the collection, analysis and interpretation of data; in the writing of the report; or in the decision to submit the article for publication.
Competing interests None.
Ethics approval Ethical approval was obtained from the London-Surrey Borders Research Ethics Committee (NRES 10/H0806/8).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The authors are fully committed to the principles of data sharing.