Article Text

Abstract
Background Heat exposure has been related to increased morbidity and mortality for several health outcomes. There is little evidence whether this is also true for COPD. This study quantified the relationship between ambient heat and hospitalisation for COPD in the Brazilian population.
Methods Data on hospitalisations for COPD and weather conditions were collected from 1642 cities during the 2000–2015 hot seasons. A time-stratified, case-crossover design was used for city-specific analyses, which were then pooled at the regional and national levels using random-effect meta-analyses. Stratified analyses were performed by sex, age group and early/late hot season. Annual change in the association was examined using a random-effect meta-regression model.
Results The OR of hospitalisation was 1.05 (95% CI 1.04 to 1.06) for every 5℃ increase in daily mean temperature at the national level, with the effect estimate stronger in the late hot season compared with the early hot season. The effect was similar in women and in men but was greatest for those aged ≥75 years. The association was stronger in the central west and southeast regions and minimal in the northeast. Assuming a causal relationship, 7.2% of admissions were attributable to heat exposure. There was no significant temporal decline in the impact of ambient heat over the 16-year study period.
Conclusion In Brazil, exposure to ambient heat was positively associated with hospitalisation for COPD, particularly during the late hot season. These data add to the growing evidence base implicating global warming as being an important contributor to the future healthcare burden.
- COPD epidemiology
Statistics from Altmetric.com
Key messages
What is the key question?
Is ambient heat during the hot season associated with increased risk of hospitalisation for COPD across the Brazilian population?
What is the bottom line?
In Brazil, exposure to ambient heat is positively associated with hospitalisation for COPD, particularly during the late hot season, with the effect estimate greatest for the elderly ≥75 years and residents living in the central west and southeast.
Why read on?
This is the first nationwide study to systematically assess the association between ambient heat and hospitalisation for COPD over the course of the hot season in a 16-year study period.
Introduction
Globally, COPD is one of the leading causes of disease burden. Annually, there are approximately 19 million new incident cases and 3 million deaths due to COPD, with 85% of cases occurring in low-income and middle-income countries.1 Moreover, as individuals with COPD, particularly the elderly, have higher risks of other comorbidities, such as cardiovascular disease,2 3 the health burden associated with COPD may be considerably larger than previously estimated.
While the causes for COPD are well established, there is emerging evidence to suggest that climatic factors, such as exposure to ambient heat, may exacerbate the symptoms of COPD and increase the risk of subsequent hospitalisation and death in affected individuals.4 5 For example, a study from Portugal reported that the risk of hospitalisation for COPD increased by over 5% for every 1℃ rise in daily mean apparent temperature in the hottest month.4 Another European study estimated that exposure to heatwaves was associated with 25% increase in COPD mortality in the summer months.5
Brazil has one of the highest annual incidence and prevalence of COPD, with approximately eight million people affected.1 The relevant hospital service utilisations have resulted in substantial stress on the freely and universally accessed public healthcare system.6 It is also one of the countries that have been most significantly affected by global warming.7 Previous studies have shown that the temperature–health relationship in Brazil and the temporal change may differ from other countries due to its unique location and climatic and geographical diversity.8 9 At present, it is unknown whether heat exposure during the hot season is associated with risk of hospitalisation due to COPD across the Brazilian population and how this association may vary over time. In this study, we used a national hospitalisation data set to explore the geographical, demographic and temporal variations in the association between exposure to ambient heat and COPD morbidity during the 2000–2015 hot seasons in Brazil.
Methods
This study followed the reporting guideline of the Strengthening the Reporting of Observational Studies in Epidemiology.10
Data collection
Data on hospitalisations for COPD were collected from 1642 cities in four Brazilian regions (northeast, central west, southeast and south) between 1 January 2000 and 31 December 2015 (online supplementary figure S1). These cities comprised 141 million residents, that is, 74% of the national population. Medical variables for each patient were extracted from the National Unified Health System (SUS), including sex, three age groups (0–64, 65–74 or ≥75 years), date of admission and primary diagnosis coded using the International Classification of Diseases-10 (J40−J44). SUS provides the Brazilian population with free and universal access to healthcare services, with both public and private hospitals joining.
Supplemental material
Data on daily minimum and maximum temperatures were collected from a national meteorological data set (0.25°×0.25° resolution).11 Data from the centre of each city were used to represent city-specific weather characteristics. Daily mean temperature was calculated as the mean of daily minimum and maximum temperatures. Data on population were collected from the Brazilian Census 2000 and 2010. Data on relative humidity were collected from 180 city-specific weather stations during 2000–2012 via the Brazilian National Institute of Meteorology.
Statistical analysis
Heat–COPD hospitalisation association
The hot season was defined as the hottest four consecutive months for each city, given the wide climatic diversity across Brazil.9 The heat–COPD hospitalisation association was estimated using the time-stratified, case-crossover design with a conditional logistic regression model.12 The principle was that each patient was treated as a stratum, where the exposure during the risk period was compared with exposures during the control periods. This within-subject comparison theoretically controls for time-constant variables at the individual patient level (eg, sex, age and socioeconomic status).13 As with other studies,13 14 control periods were defined as the same days of the week in the same calendar month of the hospitalisation. The selection of control periods from fixed time strata avoids overlap bias.15 This method can successfully adjust for long-term trend, seasonal variation and the effect of day of the week. Our initial analysis indicated that the heat–COPD hospitalisation association was linear (online supplementary figure S2; for modelling details, see the figure legend), which lasted for up to 3 days. Finally, the exposure–lag–response relationship for temperature was fitted using a distributed lag linear model, with a linear function for temperature and a natural cubic spline with 3 df for a lag of 0–3 days. The formula was as follows:  , where P is the possibility of hospitalisation for COPD; α is the vector of coefficients for strata (i is the number of hospitalisations); and
, where P is the possibility of hospitalisation for COPD; α is the vector of coefficients for strata (i is the number of hospitalisations); and  is the matrix modelled by cross-basis function by distributed lag linear model.
is the matrix modelled by cross-basis function by distributed lag linear model.
This study was performed using a two-stage approach to mitigate the computational intension on large data sets and to evaluate the heterogeneity of heat effect among cities. In the first stage, the association for each city was estimated. In the second stage, a random-effect meta-analysis with maximum likelihood estimation was applied to pool city-specific estimates at the national level. The heterogeneity of residuals of meta-analysis was evaluated using the I2 statistic.
Stratified analyses were conducted by four geographical regions, sex and three age groups. Similar to previous studies,16 17 we defined the first and last 2 months as the early and late hot seasons to examine the intraseasonal change in heat susceptibility. Meta-regression was applied to check the differences across stratified subgroups.8 13 For example, the difference between early and late heat effects was examined by setting city-specific coefficients in early and late hot seasons as the dependent variable (weighted by city-specific variances), and a binary variable representing early or late hot season as the predictor.
Attributable burden of COPD hospitalisation
For each city, daily cases attributable to heat exposure (AN) was calculated using  , where
, where  is the cumulative risk of hospitalisation (lag 0–3 days) associated with the present day’s mean temperature, compared with the risk associated with the lowest temperature value of the 2000–2015 hot seasons; and
is the cumulative risk of hospitalisation (lag 0–3 days) associated with the present day’s mean temperature, compared with the risk associated with the lowest temperature value of the 2000–2015 hot seasons; and  is the moving average of daily counts in the next 0–3 days. The attributable fraction and rate of hospitalisation were calculated by dividing the sum of daily AN by the number of hospitalisations and population size, respectively. Case-crossover design using conditional logistic regression is a special case of time-series analysis using Poisson regression,18 meaning that the value of OR from the former equates to the value of RR from the latter. We thus replaced RR with OR in this study. For some small cities, the number of hospitalisations was too small to produce stable estimates of the OR. As with previous studies,8 we applied OR pooled at the regional levels to calculate the attributable burden.
is the moving average of daily counts in the next 0–3 days. The attributable fraction and rate of hospitalisation were calculated by dividing the sum of daily AN by the number of hospitalisations and population size, respectively. Case-crossover design using conditional logistic regression is a special case of time-series analysis using Poisson regression,18 meaning that the value of OR from the former equates to the value of RR from the latter. We thus replaced RR with OR in this study. For some small cities, the number of hospitalisations was too small to produce stable estimates of the OR. As with previous studies,8 we applied OR pooled at the regional levels to calculate the attributable burden.
Long-term change in heat–COPD hospitalisation association
As with previous studies,8 19 the average annual change in the association from 2000 to 2015 was assessed using a two-stage strategy, with an assumption of linear trend. First, city-specific estimates of the heat–COPD association for each year were estimated using the conditional logistic regression model. Second, a meta-regression model was conducted, with the years entered as the linear predictor and the city-specific estimates of the heat–COPD association for each year entered as the dependent variable. Stratified analyses were performed by region.
Sensitivity analyses
The reliability of the two-stage approach was tested by comparing with the results of one-step conditional logistic regression model. The robustness of our main findings was examined by changing the maximum lag of daily mean temperature from 3 to 5 days and df of lag days from 3 to 4. The confounding effect of relative humidity was evaluated using a natural cubic spline with 3 df for 0–3 days’ moving average of station-based data in 180 cities during 2000–2012.
R software (V.3.4.1) was used to perform all data analyses. P value <0.05 (two-sided) was considered statistically significant.
Patient and public involvement
This research was done without patient or public involvement. Data on hospitalisation records were anonymised before analysis. No individuals can be identified from the anonymised data set used by the researchers.
Results
During the 2000−2015 hot seasons, the daily mean (±SD) temperature was 25.0℃±2.8℃ at the national level, declining from 25.5℃±2.6℃ to 24.6℃±2.9℃ over the course of the hot season (table 1). The temperature was lowest in the south (23.4℃±2.8℃) and highest in the northeast (27.0℃±2.1℃). During the study period, there were 523307 hospitalisations due to COPD (46% female), equating to 24 cases per 10 000 residents during each hot season. The median age of all patients was 65 years (IQR: 57–77 years).
Summary of hospitalisations for COPD and daily mean temperatures with SD in 1642 Brazilian cities during the 2000–2015 hot seasons
Regional variation
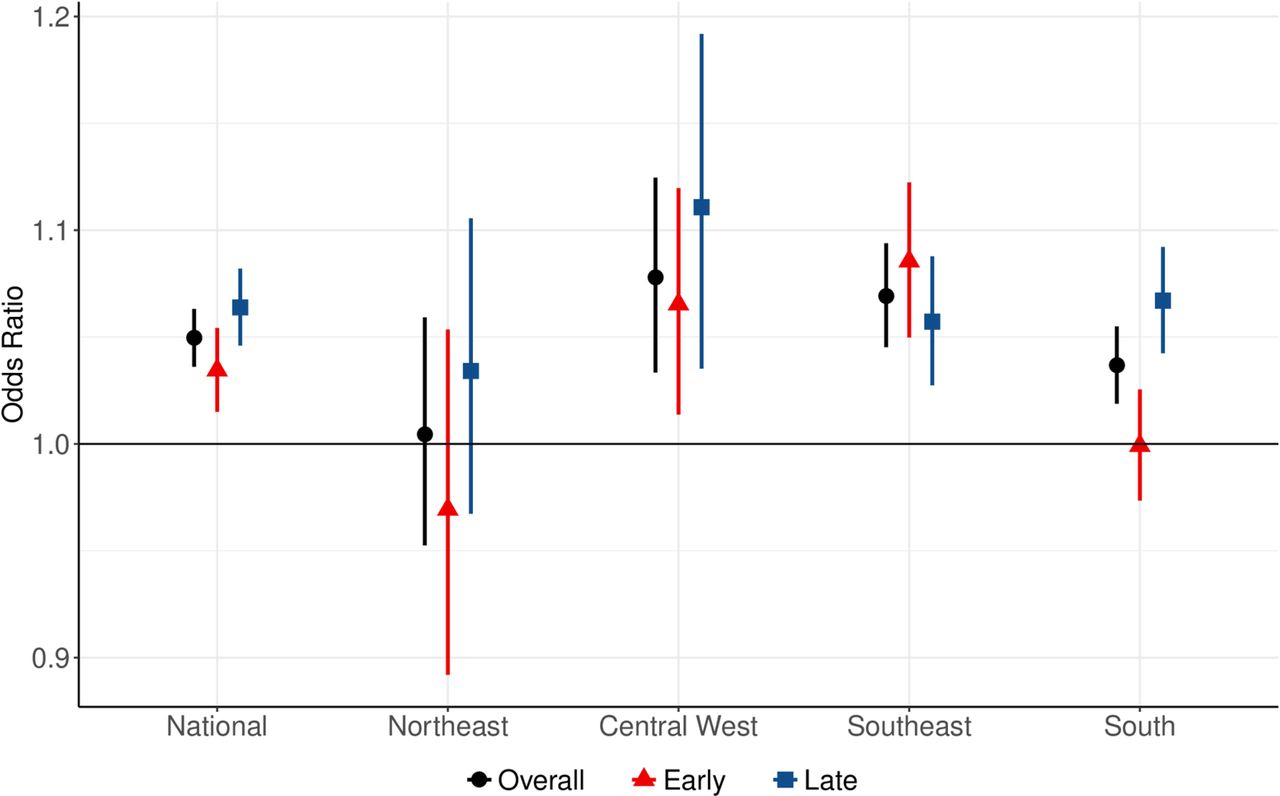
At the national level, the OR of hospitalisation due to COPD was 1.05 (95% CI 1.04 to 1.06) for every 5℃ increase in daily mean temperature during the 2000–2015 hot seasons (figure 1). The heat effect was greatest in the central west and southeast and minimal in the northeast (online supplementary table S1). The value of I2 statistic was 10.0% at the national level, ranging from 0.8% in the central west, 6.1% in the northeast, 10.3% in the south to 13.6% in the southeast. There was a stronger effect of late heat exposure at the national level and in all regions except for the southeast, but the intraseasonal change was only significant in the south (see online supplementary table S2).

OR of COPD hospitalisation for every 5℃ increase in daily mean temperature over the course of the hot seasons during 2000–2015 by region.
Demographic variation
The odds of hospitalisation were non-significantly higher for women than for men across all age groups (figure 2 and online supplementary table S3). For both women and men, the effect estimate of heat was strongest for those aged ≥75 years, while there were no significant differences between younger populations aged 0–64 years and 65–74 years. The higher effect estimate of late heat exposure was only significant among those aged ≥75 years (online supplementary figure S3 and table S2). The results of lag pattern indicated that the associations diminished within the first day after exposure to heat and were followed by hospitalisation deficit thereafter for most regions (except for the northeast) and population subgroups (see online supplementary figures S4–S5).
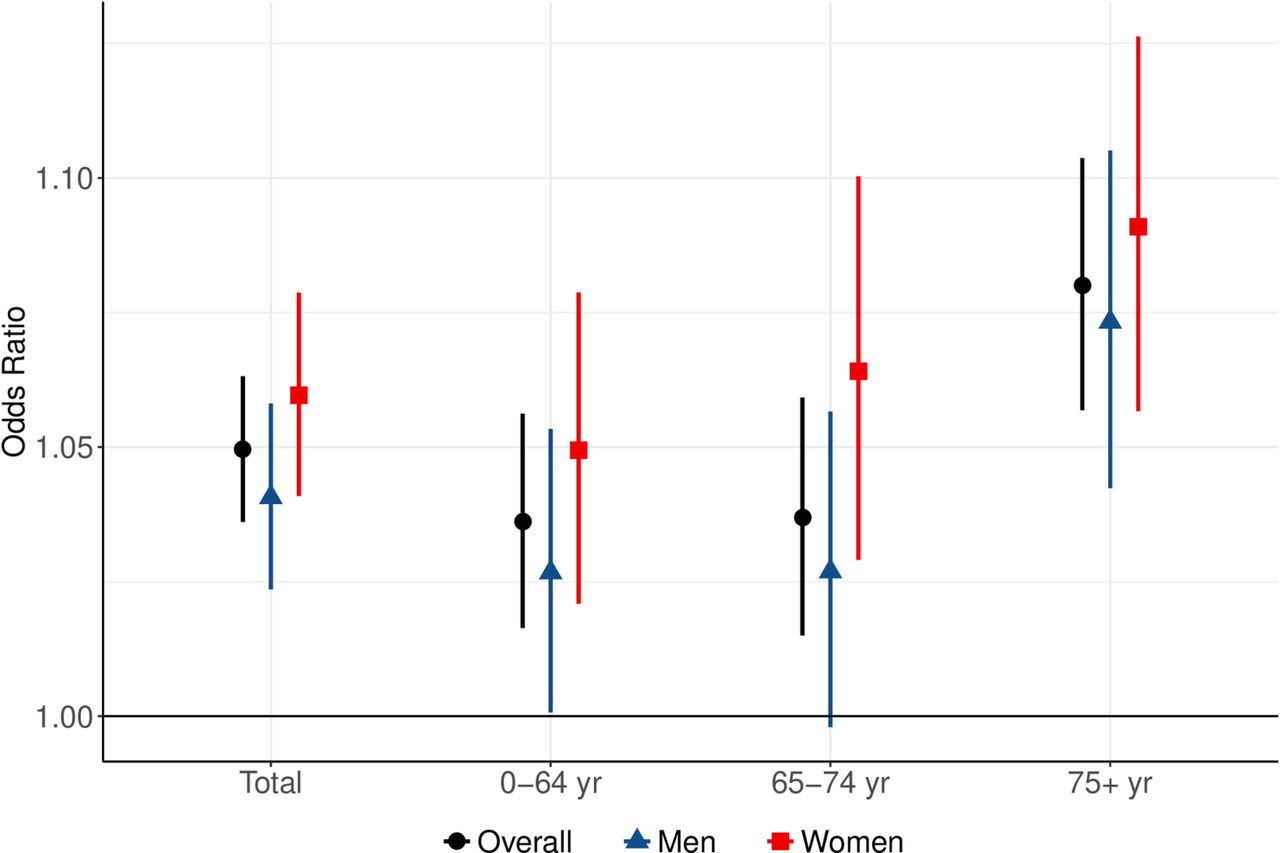
OR of COPD hospitalisation for every 5℃ increase in daily mean temperature during 2000–2015 hot seasons by sex and age group.
Attributable burden
Assuming a causal relationship, 37 824 (95% CI 17 294 to 57 386) hospitalisations were attributable to heat exposure in the 1642 Brazilian cities during the 2000–2015 hot seasons, accounting for 7.2% (95% CI 3.3% to 11.0%) of all COPD cases (table 2). The attributable fraction doubled from the early to the late hot season. At the population level, the annual attributable burden of hospitalisation for COPD was 17 (95% CI 8 to 26) cases per million residents. The geographical and demographic variations in the attributable burden were largely consistent with the estimated ORs. For example, the attributable burden for the elderly ≥75 years was the sum of that for the population <75 years. The exception was for central west and south areas; although the attributable fraction in the central west was twice as high as in the south, the attributable cases per million residents were both greatest. The geographical variation in the attributable burden is represented in figure 3. Cities with the highest attributable burden were generally located in the inlands of the central west, southeast and south regions.
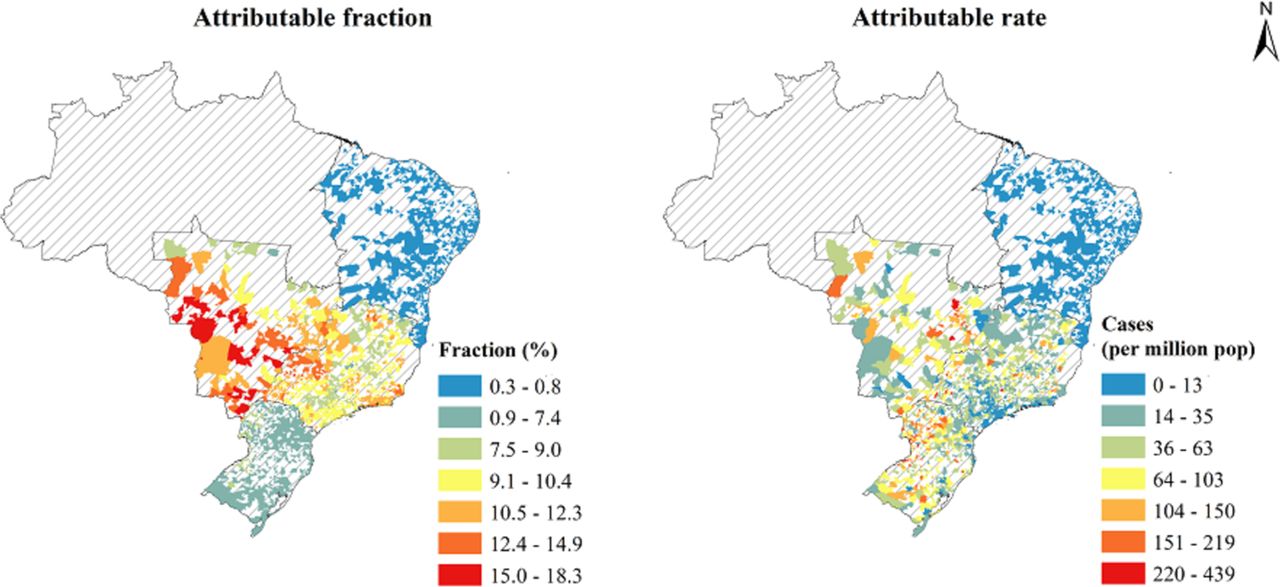
City-specific fraction (%) and rate of COPD hospitalisation attributable to heat exposure during the 2000–2015 hot seasons.
Hospitalisations for COPD attributable to heat exposure during the 2000–2015 hot seasons (with 95% CI)
Long-term change
There was no significant evidence to suggest that the association between ambient heat and hospitalisation for COPD changed from 2000 to 2015 either at the national or regional level (figure 4). The value of I2 statistic was 22.1% at the national level, 4.7% in the south, 14.1% in the central west, 18.6% in the southeast and 50.6% in the northeast.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Annual change in the heat–COPD hospitalisation association by region.
Results of sensitivity analyses
The two-stage approach was reliable compared with the performance of one-step conditional logistic regression model (online supplementary table S4). Our results were robust to a change of the maximum lag of daily mean temperature from 3 to 5 days and df of lag days from 3 to 4 (see online supplementary table S5). There was no significant difference between the effect estimates of heat exposure before and after adjustment for relative humidity using the data of 180 cities.
Discussion
This is the first nationwide study to explore the geographical, demographic and long-term variations in the association between ambient heat and hospitalisation for COPD in the Brazilian population over the course of the hot seasons between 2000 and 2015. We observed that exposure to ambient heat was positively associated with risk of hospitalisation for COPD, with the association intensifying in the late hot season. The elderly and those living in the central west and southeast regions were in particular sensitive to heat exposure. Assuming a causal relationship, approximately 7% of hospitalisations for COPD could be attributable to heat exposure during the 2000–2015 hot seasons.
Strengths and limitations of this study
This study has several strengths. First, to our best knowledge, this is the largest study worldwide to explore the association between ambient heat and COPD morbidity, by including 141 million residents. Second, this is the first study to estimate the attributable COPD hospitalisations at the population level. The city-specific results provide clear information regarding the heat-related COPD hospitalisation burden across Brazil. Third, this is also the first study to simultaneously explore the intraseasonal and long-term variations in the association between ambient heat and COPD hospitalisation in the same population. Finally, the unique location of Brazil suggests that our findings may be also pertinent to other countries that have similar climatic and geographical characteristics.
This study also has several limitations. We used grid temperature data rather than individual exposures, which may underestimate any relationship between ambient heat and COPD hospitalisation. We were unable to control for air pollution due to the lack of monitoring data in most Brazilian cities. Studies from other countries indicated that the confounding effect of air pollution may be minimal for the temperature–COPD association.20–22 However, whether this observation is also true in Brazil requires clarification by future studies when data on air pollution are available in this country. Without necessary data, we could not evaluate other potential confounders (eg, seasonal allergies and pollen counts). We were unable to calculate the age-standardised attributable rate of hospitalisation due to the limitation of Brazil Census 2000 and 2010. As a result, it is not very proper to compare the regional difference in attributable burden. However, our previous study indicated that the results should not change substantially.8 The station-based weather data from the 180 cities were the best data set we could get. The proportion of cities from the northeast in the 180 cities’ data set (40.6%) was higher than that in the 1642 cities’ data set (31.8%). Although the effect estimates of heat exposure changed non-significantly before and after adjustment for relative humidity, whether this was also true for the 1642 cities warrants further exploration.
Comparison with other studies and implications of findings
Compared with other health conditions, the relationship between ambient heat and COPD-related morbidity has not been well examined.23 24 However, our findings are consistent with the few reports that have investigated this relationship. For example, a US study reported that the risk of COPD hospitalisation for the elderly increased by 4.7% for every 5.6℃ rise in daily mean temperature in summer.20 The association was independent of air pollutants including ozone and particulate matters. Another US study suggested that for each 1℃ increase in daily mean apparent temperature above 32℃, the risk of COPD admission increased by 8% over a lag of 0–3 days during summer between 1991 and 2004, which was not influenced by levels of air pollution.25 Our study makes an important contribution to the sparse literature by reporting on the relationship in a populous lower-middle-income country that has substantial geographical and climatic diversity. The similarity in results between ours and other studies adds to the evidence base that global warming has significant consequences for an increasing number of health outcomes.
The pathophysiological mechanisms that may govern the association between exposure to ambient heat and exacerbation of COPD symptoms to the extent that they require hospitalisation are not entirely understood. Although it is beyond the scope of this paper to speculate on what these mechanisms might be, previous studies have suggested that heat-induced release of cytokines (eg, interleukin-1 or interleukin-6) may result in an inflammatory response and respiratory distress via dysregulation of cellular and vascular changes.26 27 After exposure to ambient heat, dissipating body heat through hyperventilation may trigger dynamic hyperinflation and dyspnoea in patients with pre-existing COPD.20 28 29 In addition, inhaling hot air may trigger acute bronchoconstriction of the airway through a cholinergic reflex pathway.30 31 These pathophysiological changes may also explain why the elderly are particularly vulnerable to the effects of heat exposure, as they have impaired cardiorespiratory and thermoregulatory capacity.4 25 27 Our analyses quantified that half of the attributable burden in the Brazilian population was relevant to the elderly ≥75 years. More healthcare resources are therefore needed for them to defend the impact of high temperature, considering the prolonged life expectancy and increased COPD prevalence in Brazil.1
It is plausible that populations living in hot regions may be less susceptible to heat exposure due to adaptation.20 24 32 33 Further, differences in socioeconomic indicators such as income and educational level may potentially modify any observed regional variation in the association.24 33 Similar to a US study,20 we showed that there was a non-significant effect of ambient heat in the warmest northeast. However, the strongest association was not observed in the coldest region (the south) but in areas with a more moderate climate, that is, the central west and southeast. By contrast, the difference in heat effect was minimal across US counties with similar summer temperatures as the three Brazilian regions. There was no substantial difference in the proportion of the most vulnerable population subgroup (those aged above 75 years) across the four regions, which ranged between 2.8% and 3.5%. This suggests that the distribution of population may not explain the regional difference in heat effect. However, the low effect of ambient heat in the south may be associated with region-specific socioeconomic characteristics: the south has the highest literacy rate and most balanced level of economic development compared with other parts of Brazil.34 Despite the low heat effect, the attributable hospitalisations for COPD per million residents in the south were one of the highest in Brazil, suggesting that the heat-related burden in this region was still substantial at the population level.
Findings from high-income countries have provided evidence that populations are able to adapt to the effects of ambient heat over prolonged periods of time.35 36 Possible factors responsible for this ‘adaptive response’ are unknown, but may include improved infrastructure, for example, housing insulation and air conditioning, and other factors related to greater socioeconomic development, such as more equal access to education and healthcare.36 In Brazil, we observed a non-significant decline in the heat–COPD hospitalisation association from 2000 to 2015. The lack of any significant evidence to support adaptation at the population level matches several facts: Brazil is an emerging economy which has experienced some of the greatest increases in mean temperature relative to other countries, particularly high-income countries.7 By 2016, only 16% of Brazilian households had air conditioning, which was lower than that in high-income countries such as Japan (91%) and the USA (90%).37 The value of I2 statistic of meta-regression was higher in the northeast than in other three regions, which may be largely explained by the limited COPD hospitalisations in some small cities during certain years. However, this should not change our finding of a non-significant temporal change in the northeast.
Previous studies commonly quantified the average impact of ambient heat on COPD morbidity or mortality during the hot season.4 5 20 25 Meantime, Gasparrini et al 17 reported that the risk of mortality associated with extreme high temperature declined from the early to late summer in nine countries between 1985 and 2012. Our previous study had similar findings for most cause-specific hospitalisations except for respiratory admissions.16 Some studies have explained this intraseasonal attenuation as due to less adaptation to heat effect in the early hot season or midterm harvesting effect.17 38 By contrast, our current study found that the risk of COPD hospitalisation was more associated with exposure to late heat. This finding has implications for hospitals to be aware of the increased demand of healthcare service for patients with COPD in the late hot season. However, it remains a challenge to explain the intraseasonal intensification without necessary information at the individual patient level. A hypothesis is that compared with other body systems, respiratory tract is directly exposed to ambient air. While patients with COPD or other respiratory outcomes may have adapted to the cooler temperature in the late hot season, the same level of heat exposure may impose a higher health risk than in the early hot season. However, further studies are warranted to explore the mechanisms thoroughly.
Conclusions
Exposure to ambient heat may increase the risk of COPD morbidity in Brazil, with the heat effect increasing as the hot season progresses. The elderly and those living in regions with a moderate climate are most strongly affected by heat exposure. These findings contribute to the growing evidence base indicating that global warming has significant ramifications for health outcomes, and the associated healthcare burden, particularly in countries with emerging economies.
Acknowledgments
We thank the Brazilian Ministry of Health and the Brazilian National Institute of Meteorology for providing hospitalisation and meteorological data, respectively.
References
Footnotes
Contributors YG, SL and QZ were responsible for the study concept and design. QZ did the data analysis. QZ, YG, SL, RRH, MJA, MdSZSC, PHNS and RX interpreted the data. QZ drafted the manuscript. QZ, YG and SL had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data. The corresponding authors attest that all listed authors meet the authorship criteria and that no others meeting the criteria have been omitted.
Funding QZ was supported by a Monash Graduate Scholarship, Monash International Postgraduate Research Scholarship and Monash Postgraduate Publications Award. SL was supported by an Early Career Fellowship of the Australian National Health and Medical Research Council (APP1109193). YG was supported by a Career Development Fellowship of the Australian National Health and Medical Research Council (APP1107107 and APP1163693).
Competing interests MJA holds investigator-initiated grants from Pfizer and Boehringer Ingelheim, and consultancy fee from Sanofi for unrelated research.
Patient consent for publication Not required.
Ethics approval Ethical approval was not required for secondary analysis of aggregate anonymised data from the Brazilian Hospital Information System.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.