Article Text

Abstract
The use of CPAP to control excessive daytime sleepiness in OSAHS probably also produces a substantial reduction in vascular risk. This is reviewed with particular reference to hypertension.
- AHI, apnoea/hypopnoea index
- BMI, body mass index
- CPAP, continuous positive airway pressure
- OSAHS, obstructive sleep apnoea/hypopnoea syndrome
- obstructive sleep apnoea/hypopnoea syndrome
- hypertension
Statistics from Altmetric.com
- AHI, apnoea/hypopnoea index
- BMI, body mass index
- CPAP, continuous positive airway pressure
- OSAHS, obstructive sleep apnoea/hypopnoea syndrome
Obstructive sleep apnoea/hypopnoea syndrome (OSAHS) is primarily treated to improve quality of life by controlling excessive daytime sleepiness. However, treatment of this disorder probably also produces a substantial reduction in vascular risk—which would result in OSAHS treatment improving both patient survival and quality of life. This has been an area of intense interest for over 20 years, since it has proved challenging from the methodological viewpoint and because it hints at fascinating, possibly novel, physiological mechanisms. This review discusses this area with particular reference to hypertension and hypertensive vascular risk. Heart failure and Cheyne-Stokes breathing are not discussed as they are covered in other articles in this series.
SYSTEMIC HYPERTENSION
It is clear that patients with OSAHS have, on average, higher blood pressures than age and sex matched controls, and the strength of this relationship is striking. About 40% of patients with OSAHS are hypertensive while awake according to standard criteria,1 and about 40% of patients with resistant hypertension have detectable OSAHS.2
Until recently there has been doubt as to whether this relationship is aetiological or due to a confounding association, particularly with obesity and body fat distribution. It has also been debated whether therapeutic interventions to treat OSAHS reduce blood pressure. The details of this debate are quite complex and are worth exploration since they are central to understanding the clinical dilemmas in this area, including patient treatment decisions.
OBESITY, FAT DISTRIBUTION AND OSAHS
The most difficult conundrum in understanding the link between OSAHS and blood pressure is the presence of significant obesity in most adult patients with OSAHS, and the tendency for this to be differentially distributed in the abdomen and upper body—probably producing much of its effect on sleep apnoea through the deposition of fat in the neck, narrowing the pharyngeal airway.3 This pattern of “upper body obesity” typifies male fat deposition (and is probably why OSAHS is predominantly a male disease) and is known to be a major risk factor for hypertension, insulin resistance, and hyperglycaemia—the so-called syndrome X.4,5
Most, perhaps all, of the vascular risk attributed to obesity is actually attributed to upper body fat deposition rather than overall obesity.6–8 The question is therefore whether this fat distribution pattern is actually the explanation for the raised blood pressure in patients with OSAHS rather than the OSAHS itself, or whether the OSAHS is directly the cause of the raised blood pressure (or possibly both). The usual research mechanisms for resolving such questions are the comparison of affected patients with phenotypically similar subjects without the disease but otherwise similar in their expression of confounding factors (case-control studies), or the statistical correction for the known confounders in large unselected samples (observational population sample/cohort studies). Both approaches have been applied to OSAHS and the major studies addressing these questions are summarised in table 1.
Non-randomised studies of blood pressure and OSAHS
INTERPRETATION OF NON-INTERVENTIONAL BLOOD PRESSURE DATA
There are substantial and potentially insurmountable problems for case-control and statistically corrected studies in this area. These problems relate to the ways in which OSAHS severity and body fat quantity and distribution are quantified. Whether the study design requires the selection of well matched controls or depends on the use of statistical correction for confounding, the confidence in its conclusions will depend on the accuracy with which these factors are measured (in order to select well matched controls for a case-control study), or for entry into statistical analyses in population studies. Upper body obesity is typically quantified from crude indices such as the waist to hip circumference ratio or the ratio of the waist circumference to the subject’s height.4,5,9 In both cases a rising ratio indicates an increasing upper body fat pattern. Such indices are often used in statistical analyses to determine whether there is evidence of an independent association between blood pressure and OSAHS severity after considering the effect of fat distribution (quantified as one or both of these ratios).10 A persisting relationship is then taken as evidence of independent causality.
Unfortunately, OSAHS severity is influenced by characteristics in body fat distribution which are not captured by these simple ratios, and these distribution characteristics may be differentially associated with rises in blood pressure. Neck circumference is the strongest predictor of OSAHS severity of any of the simple body dimension indices so far studied,3 and waist circumference (the main element in the crude ratio indices of upper body fat deposition) is not a robust predictor of neck size.3 It is not known whether the subtleties of fat distribution that are important in inducing sleep apnoea are also preferentially important in producing syndrome X and so raised blood pressure. It is therefore impossible to know if correction for the simple indices of fat distribution is adequate to lead one to be confident that the apparently significant residual relationships between sleep apnoea severity and blood pressure (after correcting for obesity and body fat distribution) are sufficient to prove causality.
Equally important, though likely to result in an underestimate of the importance of OSAHS in causing raised blood pressure, are the measurement problems in the quantification of sleep apnoea itself. Traditionally the severity of OSAHS has been assessed by counting the number of episodes of respiratory disturbance per hour of sleep. Unfortunately, this is at best a semi-quantitative technique. The number of respiratory episodes per hour is heavily influenced by arbitrary thresholds in defining what is significant both in terms of the amount of physiological disturbance present (does transient partial pharyngeal collapse alone count, does it count if it is associated with arousal from sleep, is some fall in airflow through the upper airway needed and if so how much, and if complete airway obstruction is needed then for how long, etc) as well as the vagaries of measurement equipment and its interaction with the patient11 and the variability in human scoring behaviour.12,13 Finally, there is a substantial variation in the severity of sleep apnoea from night to night—particularly in the mid range of disease severity. All these factors mean that the relationship between the apparently “simple” index of respiratory disturbance and the symptomatic consequences of OSAHS are very loose.14,15 This poor measurement precision, accuracy, and reproducibility will result in “noise” in the data gathered in the quantification of OSAHS which will greatly weaken its apparent correlation with other factors such as blood pressure. This will tend to result in potentially important relationships getting lost in both case-control and cohort epidemiology studies, particularly where the analyses are attempting to dissect out the contributions of factors which are already closely correlated and therefore easily confused.
This methodological problem is further worsened by limited information on which aspects of the OSAHS might be the important drivers of adverse vascular risk (particularly blood pressure). Academic attention tends to focus on the number or severity of the nocturnal respiratory events, presumably because this is relatively easily measured. In reality, any number of other factors such as hormonal disturbances, behaviour changes, or the intensity of daytime sleepiness might be the salient factors and these are certain to have weak and probably non-linear relationships with simple indices of breathing disturbance.
These methodological debates inevitably seem rather academic and dry, but the distortion they can produce in data collected with care and with the best of intentions can be very important. Here, the importance of vitamin E in vascular risk provides a salutary lesson. Lower cardiovascular risk is strongly and independently associated with higher blood levels of vitamin E in very large observational studies (of over 50 000 subjects). However, when randomised trials of vitamin E supplementation aimed at reducing vascular risk are performed, the intervention is proved to be entirely without benefit.16
INTERVENTION TRIALS OF OSAHS TREATMENT AND BLOOD PRESSURE
As the vitamin E and cardiovascular risk story emphasises, the randomised clinical trial presents the opportunity to assess properly whether correcting a physiological disturbance produces the expected (and desired) outcome. Of course, a negative trial result does not exclude an aetiological relationship between a physiological disturbance and a consequence but, provided the trial is adequately powered, it does show that the treatment is ineffective for that outcome. There are now six randomised controlled trials examining the effect of nasal continuous positive airway pressure (nCPAP) treatment for OSAHS on systemic arterial blood pressure, and these are summarised in table 2. These trials should provide sound primary data for discussion in this area.
Randomised controlled studies of blood pressure and OSAHS
Superficially there is a conflict between these trials with some being clearly positive, suggesting nCPAP reduces blood pressure in OSAHS, and some negative. However, a detailed examination of the data may provide an explanation for this disparity and perhaps also indicate which subgroups of patients with OSAHS might benefit from nCPAP therapy in terms of blood pressure control.
The first study published was a crossover trial of nCPAP versus an oral placebo from the Edinburgh group.17 Overall, this study showed a just detectable fall in blood pressure in 68 patients with, on average, moderately severe OSAHS (AHI 35/hour, Epworth sleepiness score 15). Interestingly, on a post hoc analysis this benefit occurred in the 14 subjects with more severe disease (>4% desaturation rate of >20 per hour).
The Spanish collaborative study18 was negative. In this study 55 subjects were randomised in a parallel trial to therapeutic nCPAP or subtherapeutic nCPAP (control group). Intentionally, this group studied patients with mild/moderate obstructive apnoea on respiratory criteria with little daytime sleepiness (>4% desaturation rate >30 per hour, Epworth score <11).
The Oxford study also used a parallel subtherapeutic controlled model1 but in patients with quite severe disease, having both sleepiness and marked hypoxaemia (mean >4% desaturation rate 37 per hour, mean Epworth sleepiness score 16). Overall, this study showed a significant therapeutic blood pressure response to treatment and, again, post hoc subgroup analysis showed that this was mostly limited to patients with the most severe disease (>4% desaturation rate >33 per hour). In this subgroup the fall in blood pressure was enough to reduce the theoretical risk of stroke by about 35%.
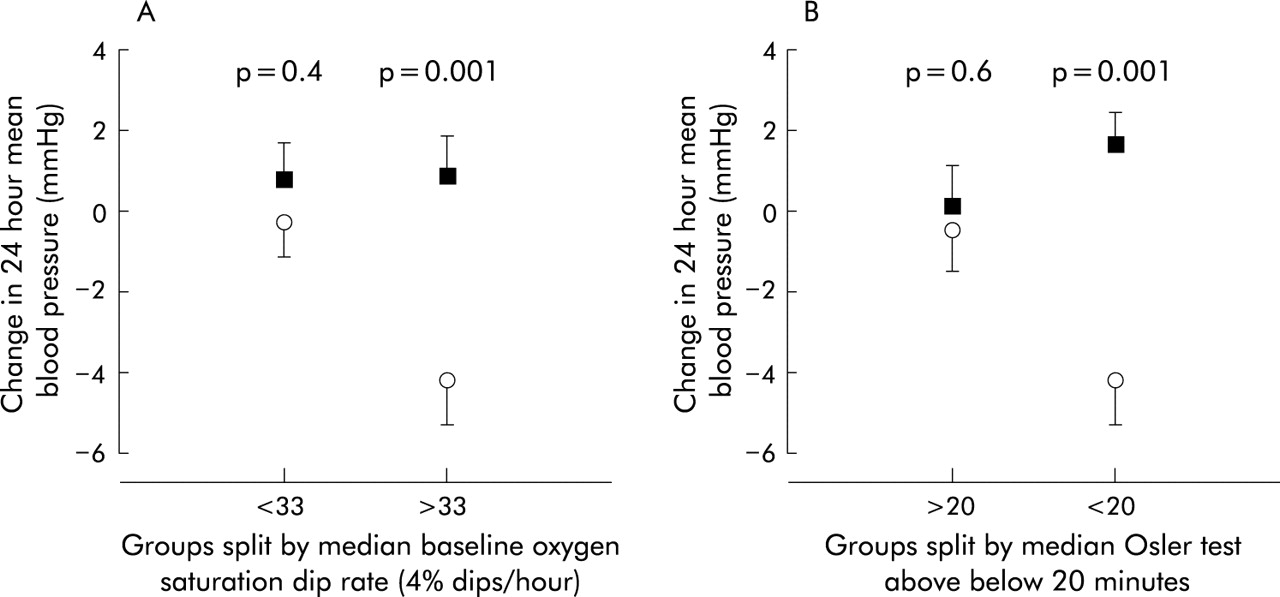
In this study there was also a relationship between the severity of the patients’ Osler (Oxford Sleep Resistance) test (a modified maintenance of wakefulness test), measured sleepiness, and the magnitude of their blood pressure fall with nCPAP.1 As shown in fig 1, this was just as powerful a predictor of the fall in blood pressure with nCPAP as was the severity of the respiratory disturbance. The change in 24 hour mean blood pressure with therapeutic nCPAP treatment is shown, with the groups split into those with a baseline 4% oxygen desaturation dip rate above or below 33 (the median dip rate) in fig 1A and with the groups split by baseline Osler test result of more or less than 20 minutes in fig 1B. The therapeutic blood pressure fall is as strongly correlated with sleepiness as it is with objective sleep apnoea severity. This shows the apparent limitation of the therapeutic benefit of nCPAP to sleepy patients with typical OSAHS, which is consistent with the collaborative Spanish study.18 Interestingly, we found that this relationship appeared partially independent of objective OSAHS severity, suggesting perhaps that the mechanisms causing the sleepiness are themselves the cause of some of the blood pressure fall with nCPAP.1

{kind=link}
Fall in blood pressure with therapeutic nasal CPAP in the Oxford randomised placebo controlled study.1 A greater fall in 24 hour mean blood pressure was seen in subjects with a baseline 4% oxygen desaturation dip rate of >33 (A) and in those with <20 minutes awake on the baseline Osler test (B).
In a recently published study by Becker et al,19 patients were randomised to receive fully therapeutic or partially therapeutic nCPAP (which reduced apnoeas by up to 50%). The large fall in day and night blood pressure seen in the therapeutic group (about 10 mm Hg) may be partly explained by the inpatient (and therefore minimally ambulant) hospital setting of the study, the severity of OSAHS studied (mean apnoea hypopnoea index 64), the longer length of CPAP treatment (9 weeks compared with 4 weeks in the Edinburgh and Oxford studies), and the fact that two thirds of those completing the study were on antihypertensive medication. In the Oxford study, antihypertensive medication also seemed to predict a large therapeutic response.1 Of interest in the study by Becker et al is the fact that no blood pressure reduction was seen in the partially treated group (the control arm) despite a reduction in AHI of up to 50%, demonstrating the importance of complete resolution of OSAHS.
The San Diego study20 showed a fall in daytime blood pressure and a lesser effect on night time blood pressure of a magnitude similar to that seen in the Oxford study. They studied a small population over 10 days, also demonstrating a reduction in daytime plasma norepinephrine levels and night time urinary norepinephrine excretion.21 A small reduction in blood pressure was also seen in the placebo CPAP group.
The randomised trial by Monasterio et al22 did not use a control intervention (nCPAP is compared with conservative care) and quantified blood pressure from office cuff recordings. These results are therefore difficult to compare directly with the other trials using more rigorous assessment methods.
In summary, these trials all show convincing falls in blood pressure in sleepy patients with severe OSAHS, and the magnitude of this benefit seems largest in patients with OSAHS which is severe on both objective (sleep study) and subjective (sleepiness) criteria and in those patients with treated hypertension at baseline. There is no benefit in subjects without daytime sleepiness.
CONFLICTS BETWEEN CLINICAL TRIAL DATA AND NON-INTERVENTIONAL DATA
There is an obvious and interesting apparent discrepancy between the interventional data discussed above and the observational epidemiology and case-control studies. Specifically, “mild” OSAHS (defined as having minimal symptoms and/or few respiratory events) does not appear to be associated with substantial therapeutic blood pressure falls following nCPAP, but is apparently independently associated with raised blood pressure in the community.
There are two likely explanations for this apparent dichotomy. Firstly, it is possible that the clinical trial data are simply underpowered to detect the therapeutic benefit in patients with mild disease. Secondly, it is possible that two separate mechanisms are present to explain the data—one responsive to nCPAP and present in subjects with severe disease and one unresponsive to nCPAP (and perhaps methodological in nature) seen in the community epidemiology studies. This is not impossible, given the plethora of potential explanations for the community data explored in the section discussing the interpretation of non-interventional trial data (above). There are as yet very few data in subjects with mild disease and specific sizeable trials are needed in this area to answer this important question.
CONCLUSION
Robust clinical trial data now show that OSAHS is independently associated with systemic hypertension and that blood pressure falls when severe sleep apnoea is treated with the most effective available therapy, nasal CPAP. There remains a conflict between the apparent size of the effect seen in mild disease in observational studies compared with the small or absent effect in the intervention trials. This may simply be due to the lack of adequately powered trials or to methodological problems with the observational data. Large intervention trials will resolve this question in due course. For the clinician, the current message is that treating a typical patient with severe OSAHS (for which the majority of nasal CPAP therapy is prescribed) produces clinically useful blood pressure reductions as well as yielding important symptomatic benefits.