Article Text

Abstract
Background Cocoa seems to exert artery dilatation via oxidative stress inhibition but the mechanism is still unclear.
Objectives To investigate whether in smokers, dark chocolate elicits artery dilatation via down-regulation of NOX2, the catalytic core of NADPH oxidase.
Methods Flow-mediated dilatation (FMD), oxidative stress (as assessed by urinary isoprostanes excretion), nitric oxide generation (as assessed by serum levels of nitrite/nitrate (NOx)), NOX2 activity (as assessed by blood levels of soluble NOX2 derived peptide (sNOX2-dp)) and serum epicatechin were studied in 20 smokers and 20 healthy subjects (HS) in a crossover, single-blind study. Patients were randomly allocated to 40 g dark chocolate (>85% cocoa) or 40 g of milk chocolate (≤35% cocoa). FMD, urinary isoprostanes, NOx and sNOX2-dp were assessed at baseline and 2 h after chocolate ingestion.
Results Smokers had lower FMD and NOx and higher sNOX2-dp compared to HS. After dark chocolate intake, urinary isoprostanes and sNOX2-dp significantly decreased and FMD and NOx significantly increased in smokers but not in HS. No changes of the above variables were observed after milk chocolate intake. Multiple linear regression analysis showed that in smokers the only independent predictive variable associated with a change in FMD was a change in sNOX2-dp. Serum epicatechin increased in either group only after dark chocolate intake, reaching values higher than 0.1 μM. Platelets from smokers (n=5), but not from HS (n=5), showed lower p47phox translocation to platelet membrane and higher NOx when incubated with 0.1–10 μM epicatechin.
Conclusion Results suggest that in smokers, cocoa enhances artery dilatation by lowering of NOX2 activation.
- Atherosclerosis
- cocoa
- flow mediated dilation
- oxidative stress
- Carotid artery disease
- oxidative stress
- endothelial function
- oxidative stress
- peripheral vascular disease
- coagulation factors
- deep vein thrombosis
- platelet activation
- platelet adhesion
- platelets
Statistics from Altmetric.com
- Atherosclerosis
- cocoa
- flow mediated dilation
- oxidative stress
- Carotid artery disease
- oxidative stress
- endothelial function
- oxidative stress
- peripheral vascular disease
- coagulation factors
- deep vein thrombosis
- platelet activation
- platelet adhesion
- platelets
Introduction
Endothelial dysfunction has been recognised as a hallmark of systemic atherosclerosis and a useful marker to stratify the risk of cardiovascular disease in patients at risk or with established clinically manifested atherosclerosis.1 Flow-mediated dilatation (FMD) has become a conventional measure of endothelial dysfunction in human atherosclerosis.1 Consistent with other clinical settings of human atherosclerosis, smokers have endothelial dysfunction, as assessed by lower FMD compared to controls,2 and a close association with coronary artery disease.3 Hence, knowledge of the mechanism(s) responsible for endothelial dysfunction may be of potential interest for developing new therapeutic approaches.
FMD is prevalently dependent on release of nitric oxide (NO),4 a potent vasodilator and anti-aggregating molecule, from the vascular wall.5 Oxidative stress plays a major role in modulating NO bioactivity inasmuch as it greatly contributes to its rapid metabolism via NO inactivation by O2−.5 Such interaction leads to formation of peroxynitrite, a potent oxidant molecule present in the atherosclerotic plaque.5 Smokers have enhanced oxidative stress,6 and reduced FMD2 and NO generation levels.7
Several epidemiological studies have suggested that cocoa exerts beneficial cardiovascular effects8–10; these effects are probably mediated by its content of polyphenols, a heterogeneous group of molecules found primarily in fruits and vegetables.10 In smokers, cocoa administration improved endothelial dysfunction but the mechanism is still unclear.7 11 A previous study hypothesised that cocoa improves endothelial dysfunction by reducing oxidative stress and eventually increases NO generation and/or synthesis.7 However, the oxidative stress-generating pathway involved in such a phenomenon is still undefined.
Several reactive oxygen species (ROS) generating enzymes, including myeloperoxidase, xanthine oxidase and nicotinamide adenine dinucleotide phosphate (NADPH) oxidase, may be implicated in artery dysfunction.12 Experimental studies performed in animal models suggest a pivotal role of NADPH oxidase in modulating artery tone.13 14 In particular, overexpression of NOX2, the catalytic subunit of NADPH oxidase, potentiates the haemodynamic response to angiotensin II.13 We have provided evidence of a major role for NADPH oxidase in modulating artery tone in humans, as patients with hereditary deficiency of NOX2, the catalytic core of NADPH oxidase, had enhanced FMD compared to controls.15 This change was associated with reduced formation of isoprostanes, a marker of oxidative stress, and an increase of NO generation, suggesting that NADPH oxidase modulates artery tone via oxidative stress-mediated NO inactivation.15 On the basis that oxidative stress is higher in smokers,6 we speculated that NADPH oxidase up-regulation could account for enhanced oxidative stress and reduced FMD; thus, we tested the hypothesis that dark chocolate could restore endothelial function in smokers via a mechanism mediated by NOX2 down-regulation.
Materials and methods
Twenty healthy subjects (HS) and 20 smokers, matched for age and gender (table 1), agreed to participate in the study, which was performed between October and December 2010. Each smoker consumed an average of 11 cigarettes per day (range 6–28). No study participant took any medication. Subjects were randomly allocated to a treatment sequence with 40 g of dark chocolate (≥85% cocoa) or milk chocolate (≤35% cocoa) in a crossover, single-blind design. There was a 1 week washout between the two phases of the study. FMD, oxidative stress (as assessed by urinary isoprostanes excretion), soluble NOX2 derived peptide (sNOX2-dp) and serum levels of nitrite/nitrate (NOx) and epicatechin (EC) were assessed at baseline, after a 24 h abstinence from food rich in polyphenols, and 2 h after ingestion of chocolate. Participants were studied after a fasting period of 8 h and, for smokers, after a smoke-free interval of at least 2 h before each experiment.
Clinical characteristics of smokers and healthy subjects (HS)
The schedule of the procedure was as follows:
8:00: first blood and urine samples were collected after a fasting period of 8 h.
8:15: first FMD was performed.
8:45: participants in the study received 40 g of chocolate (dark or milk); they had 15 min to eat chocolate.
10:45: second blood and urine samples were collected.
11:00: second FMD was performed.
No beverages were permitted during this period.
All subjects underwent a full medical history and physical examination. Subjects were excluded from the study if they had liver insufficiency, serious renal disorders (serum creatinine >2.8 mg/dl), acute cerebrovascular disease, acute myocardial infarction, dyslipidaemia, diabetes or hypertension, or were taking antioxidants. All participants received a questionnaire to evaluate their fruit and vegetable intake.16
An in vitro study was performed on blood taken from five smokers (three men and two women, mean age 32±4 years) and five HS, matched for age and gender. We analysed the effect of scalar doses of EC (0.1–10 μM) on platelet ROS, NOx production and platelet NOX2 activation.
Informed written consent was obtained from all subjects; the study conformed to the ethical guidelines of the 1975 Declaration of Helsinki and was approved by the Sapienza University of Rome Ethics Committee.
Randomisation and blinding
An individual not involved in the study assigned codes to the study treatments, randomly allocated the participants to a treatment sequence with dark or milk chocolate, and kept the key in a sealed envelope. The randomisation was carried out by a procedure based on a random numeric sequence. The authors and laboratory technicians were unaware of the treatment allocation.
FMD measurements
FMD measurement was assessed as previously described.15
Urinary PGF2α-III assays
Quantification of isoprostanes was performed by measuring urinary excretion of PGF2α-III by a previously described and validated enzyme immunoassay method.17 Intra- and inter-assay coefficients of variation were 5.8% and 5.0%, respectively.
Analysis of serum and platelet NOx
Blood samples were drawn without stasis from an antecubital vein with a 21-gauge needle, and mixed with 0.13 mol/l sodium citrate (ratio 9:1, v/v). To obtain platelet-rich plasma, samples were centrifuged for 15 min at 180 g. To avoid leucocyte contamination, only the top 75% of the platelet-rich plasma was collected. Platelet pellets were suspended in HEPES buffer, pH 7.4 (2×108 platelets/ml, unless otherwise noted) and treated with or without arachidonic acid (AA) in the presence or not of scalar doses of EC (0.1–10 μM).
After treatment the pellets were centrifuged; the supernatant was collected and stored at −80°C until measurement.
NO was measured in serum and in the supernatant of agonist-stimulated platelets by measurement of metabolic end products (Tema Ricerca)—that is, nitrite and nitrate (NOx). Intra- and inter-assay coefficients of variation were 2.9% and 1.7%, respectively.
Platelet ROS production
Platelet suspension (2 ml) was incubated with 2′,7′-dichlorofluorescin diacetate (5 mM) for 15 min at 37°C. Samples were treated with control medium or with EC (0.1–10 μM) (10 min at 37°C). After incubation, 100 μl of the sample was treated with or without AA (0.5 mM). Then 10 μl of each sample was diluted with 1 ml of phosphate-buffered saline and analysed by flow cytometry. Basal ROS level in resting platelets was expressed as mean fluorescence; AA-induced ROS production was expressed as stimulation index (SI=mean level of fluorescence in AA-stimulated platelets/mean level of fluorescence in unstimulated platelets).
NADPH oxidase activity evaluated by p47phox translocation to platelet membrane
To analyse a direct index of NADPH oxidase activation, we evaluated the effect of stimulation with AA (0.5 mM) on p47phox translocation from cytosol to membranes as reported by Pignatelli et al.18 Samples treated with scalar doses of EC (0.1–10 μM) (10 min at 37°C) and stimulated with AA were compared with samples stimulated in the presence of control medium.
ELISA detection of sNOX2-dp
NOX2-derived peptide, a marker of NADPH oxidase activation, was detected in serum by ELISA as previously described by Pignatelli et al.19 The peptide was recognised by the specific monoclonal antibody against the amino acidic sequence (224–268) of the extra membrane portion of NOX2. Values were expressed as pg/ml; intra- and inter-assay coefficients of variation were 5.2% and 6%, respectively.
Sample epicatechin
Serum (100 μl) was extracted twice with 0.8 ml followed by 0.5 ml of ethyl acetate, by vortexing for 1 min in a 1 ml vial. After centrifuging the mixture for 5 min at 3500 g, the top layers comprising ethyl acetate were removed, pooled and evaporated to dryness under nitrogen.20 The dried samples were dissolved in methanol (100 μl) before analysis by HPLC.
EC was analysed using an Agilent 1200 Infinity series HPLC system equipped with an Eclipse plus C18 column (4.6×100 mm). All analyses were performed at 25°C. An isocratic mobile phase consisting of water–methanol (80:20) was used, running at a flow rate of 1.2 ml/min; UV detection was carried out at 280 nm. The sample injection volume was 20 μl. Chromatographic peaks of analytes were identified by comparing their retention times with those of the standard.21
Statistical analysis
Sample size determination
We computed the minimum sample size with respect to a two-tailed, one-sample Student t test with Welch correction, considering: (i) a difference for FMD variation in smokers to be detected between dark and milk chocolate treatments |δ|≥2.5%; (ii) SD of the paired differences =3.0%; (iii) type I error probability α=0.05 and power 1−β=0.90. This resulted in n=18 patients, which was increased to n=20.
Statistical methods
Continuous variables are reported as mean±SD unless otherwise indicated. Comparisons between smokers and HS were carried out by Student t test and were replicated as appropriate with non-parametric tests (Kolmogorov–Smirnov (z) test in case of non-homogeneous variances as verified by the Levene test).
The crossover study data were analysed for the assessment of treatment and period effects, by performing a split-plot ANOVA with one between-subject factor (treatment sequence) and two within-subject factors (period 1 vs 2; pre- vs post-treatment). The full model was considered, allowing for the assessment of all main effects and two- and three-way interactions. Pairwise comparisons were corrected by the Bonferroni correction factor. Bivariate analysis was performed with the Spearman linear regression test. Multiple linear regression analysis was performed using a forward selection. In vitro experiments were analysed by ANOVA.
A value of p<0.05 was considered statistically significant. All analyses were carried out with SPSS V.18.0.
Results
Clinical characteristics of smokers and HS are reported in table 1. There were no differences between the two groups with the exception of smoking habit. Furthermore, we did not observe differences in fruit and vegetable dietary intake between smokers and HS.
At baseline, compared to HS, smokers had lower FMD and NOx serum levels, and higher sNOX2-dp and urinary excretion of isoprostanes (figure 1); conversely, arterial brachial diameters and EC serum levels did not differ between groups (data not shown).
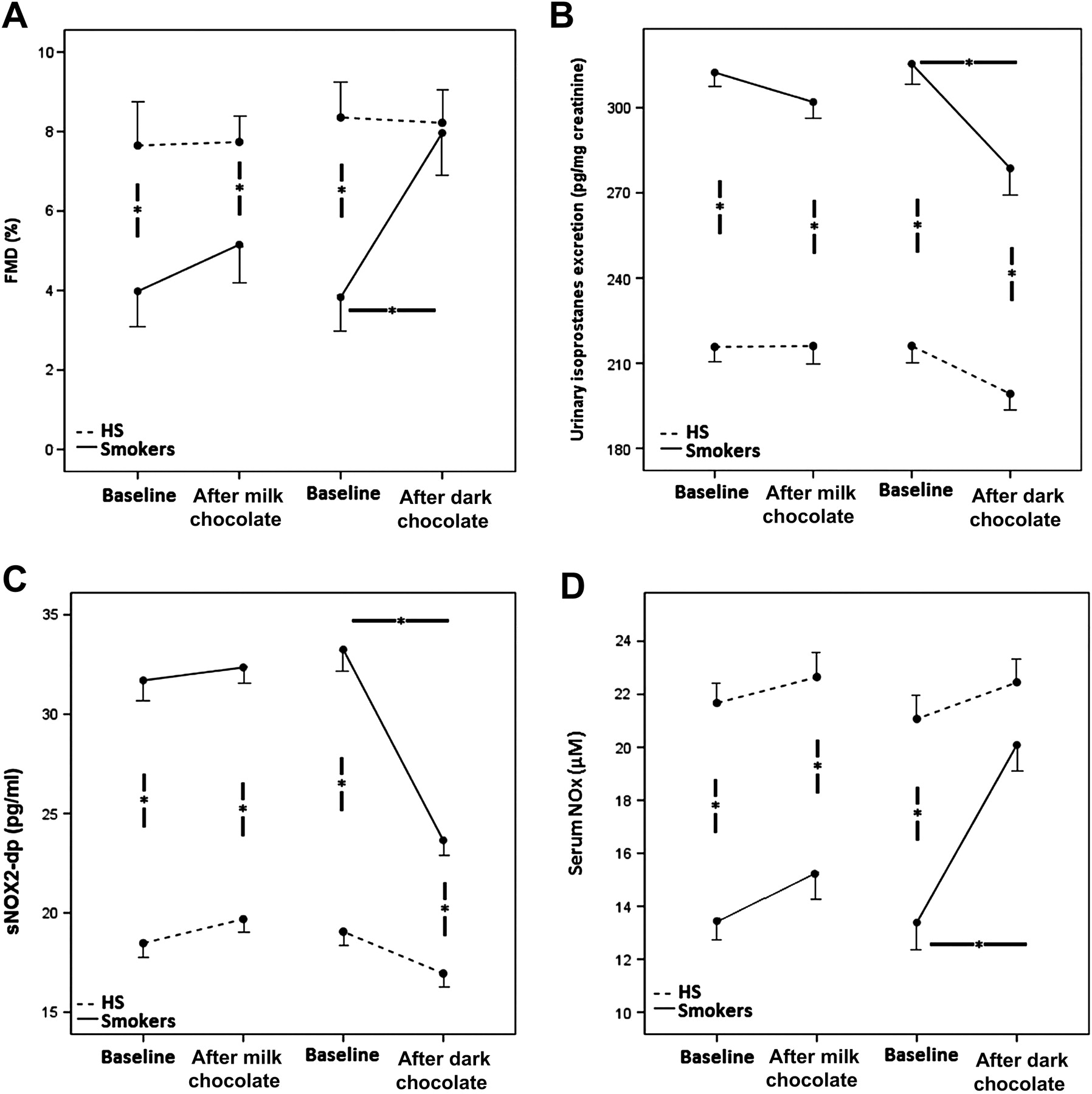
(A) Flow-mediated dilatation (FMD) before and 2 h after intake of dark or milk chocolate in smokers and healthy subjects (HS). (B) Serum nitrite/nitrate (NOx) levels before and 2 h after intake of dark or milk chocolate in smokers and HS. (C) Serum soluble NOX2 derived peptide (sNOX2-dp) levels before and 2 h after intake of dark or milk chocolate in smokers and HS. (D) Urinary excretion of isoprostanes before and 2 h after intake of dark or milk chocolate in smokers and HS. Data are presented as mean+SE.
The overall correlation analysis, carried out by Spearman test, showed that at baseline FMD directly correlated with serum NOx levels (Rs=0.565, p<0.001) (figure 2A). Moreover, FMD inversely correlated with sNOX2-dp (Rs=–0.348, p=0.002) (figure 2B) and urinary excretion of isoprostanes (Rs=−0.487, p<0.001) (figure 2C). The latter, in turn, significantly correlated with sNOX2-dp (pg/ml) (Rs=0.683, p<0.001) and with NOx (Rs=−0.734, p<0.001).
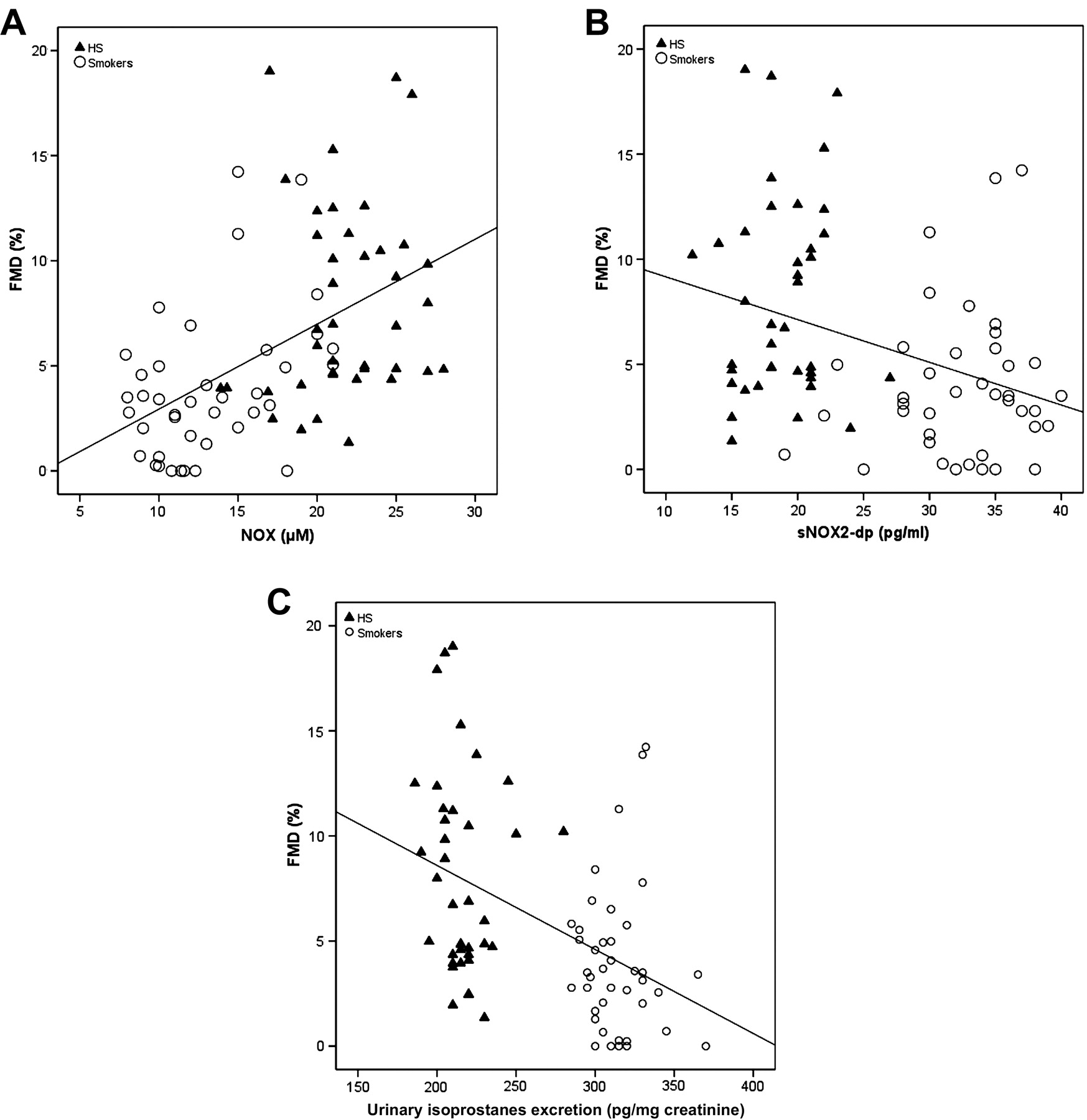
Linear regression analysis at baseline between flow-mediated dilatation (FMD) versus nitrite/nitrate (NOx) (A), FMD versus soluble NOX2 derived peptide (sNOX2-dp) (B), and FMD versus urinary isoprostanes excretion (C). HS, healthy subjects.
Compared to baseline, after milk chocolate ingestion, there was no difference between serum EC levels in HS and smokers (from 0.39±0.37 nM to 0.42±0.23 nM (NS), and from 0.40±0.36 nM to 0.43±0.30 nM (NS), respectively); conversely, a significant increase of serum EC levels was observed after dark chocolate ingestion in HS and smokers (from 0.43±0.35 nM to 118.2±53.1 nM (p<0.001), and from 0.45±0.35 nM to 120.9±54.2 nM (p<0.001), respectively).
A significant difference for treatments was found in smokers with respect to FMD (F=6.9, p=0.01; figure 1A), NOx (F=6.4, p=0.02; figure 1B), sNOX2-dp (F=7.2, p=0.01; figure 1C), and urinary isoprostanes excretion (F=9.4, p=0.006; figure 1D), from the ANOVA performed on crossover study data.
In particular, in smokers, the pairwise comparisons showed that sNOX2-dp and urinary isoprostanes excretion significantly decreased after dark chocolate (from 33.25±5.0 to 23.65±3.9 pg/ml, p<0.001, and from 315.4±20.4 to 278.65±27.2 pg/mg creatinine, p<0.001, respectively), while no changes were observed after milk chocolate (from 31.7±4.5 to 32.3±4.5 pg/ml, p=0.151, and from 312.4±18.8 to 300.7±34.4 pg/mg creatinine, p=0.069, respectively). (figure 1A,B).
Compared to baseline, in HS, no significant effect was found after dark and milk chocolate intake for FMD, urinary isoprostanes excretion, sNOX2-dp and NOx (figure 1).
A linear correlation analysis showed that Δ (expressed by difference of values between before and after chocolate intake) of FMD correlated with Δ of sNOX2-dp (Rs=−0.296; p=0.008) and Δ of serum NOx (Rs=0.287; p=0.01). Furthermore, Δ of sNOX2-dp correlated with Δ of urinary isoprostanes excretion (Rs=0.578; p<0.001). Multiple linear regression analysis showed that the only independent predictive variable associated with Δ FMD in smokers was Δ of sNOX2-dp (SE=0.117; standardised coefficient β=−0.356; p=0.02).
In vitro study
Since the interventional study suggested an interplay between dark chocolate and oxidative stress, we performed experiments to evaluate the role of EC, one of the most important components of dark chocolate,10 on ROS, NOx production and p47phox translocation in platelets from HS and smokers. AA-stimulated platelets incubated with scalar doses of EC showed a decrease of platelet ROS production (figure 3A) and p47phox translocation (figure 3B), and an increase of NOx production (figure 3C); this effect was detected in smokers but not in HS.

{kind=link}
{kind=link}
{kind=link}
Effect of scalar doses of epicatechin (0.1–10 μM) on platelet ROS (A), nitrite/nitrate (NOx) (B), and p47phox translocation (C). The experiments were performed in blood taken from 5 healthy subjects (HS) and 5 smokers. AA, arachidonic acid. *p<0.05.
Discussion
The study provides evidence that in smokers, acute ingestion of dark chocolate is associated with an improvement of FMD via down-regulation of NOX2-related oxidative stress.
Previous studies consistently showed that in smokers, the generation of ROS is enhanced and may have a deleterious effect on the dilatation of arterial walls.6 22 In accordance with these findings, smokers had reduced FMD and enhanced urinary excretion of isoprostanes, a marker of oxidative stress.23 We have reported that isoprostanes, that stem from AA interaction with ROS, are generated prevalently by NADPH oxidase15; thus, the formation of isoprostanes was significantly reduced in patients with a hereditary deficiency of NOX2, and increased in patients with NOX2 up-regulation.15 We have recently developed an assay that allows us to measure the circulating levels of a NOX2 fragment that is released on activation of platelets, leucocytes and monocytes.19 Even if the assay does not permit quantification of enzyme activation by single cell lines, it is an easy tool for measurement of activation of the enzyme by blood cells. By this assay we could demonstrate that in smokers NOX2 is overactivated and significantly correlated with urinary isoprostanes, further reinforcing the hypothesis that NOX2 activation plays a pivotal role in isoprostane formation.
In accordance with a previous report where dark chocolate was administered to heart transplant patients,24 ingestion of dark chocolate was associated with enhanced FMD and decreased oxidative stress as documented by the significant reduction of urinary isoprostane. However, it should be underscored that the effect was detected only in smokers as no changes of FMD and oxidative stress were seen in HS. These data are in accordance with a previous study where no significant increase of FMD (after 2 h) and oxidant status (after 3 h) was observed after dark chocolate ingestion in HS.25 The decrease of urinary isoprostanes was coincident with NOX2 down-regulation, suggesting that dark chocolate reduces the activation of the enzyme and in turn the formation of isoprostanes. An interesting finding of our study was that serum nitrite and nitrate, a marker of NO generation,26 significantly increased and inversely correlated with urinary isoprostane. This suggests that oxidative stress reduction favoured enhanced bioactivity and/or biosynthesis of NO. We recognise that the measure of nitrite and nitrate in the serum may be characterised by a great intra-individual variability.26 This may depend on the fact that NOx is influenced by many exogenous and endogenous factors, including dietary nitrate uptake, inhalation of atmospheric gaseous nitrogen oxides, salivary formation and renal function.26 However, the fact that NOx changed as early as 2 h after dark chocolate ingestion should exclude the possibility that such confounding factors may have influenced the results.
In contrast to dark chocolate, milk chocolate showed a trend to an increase in FMD. This may be dependent on the fact that the antioxidant effect of cocoa is attenuated if milk is added to chocolate and by the low concentration (≤35%) of cocoa contained in milk chocolate.10 27 We could not exclude, however, that a higher dosage of milk chocolate significantly affects FMD.
The vasodilatation effect of cocoa is attributed to its high content of polyphenols10; thus, ingestion of pure polyphenol is associated with arterial dilatation similar to that observed with flavonol-rich cocoa.28 Such an effect could be dependent on the polyphenol antioxidant effect that has been documented in humans by reduction of markers of oxidative stress as well as by an increase of its plasma antioxidant property.24 In vitro studies corroborated such findings as single polyphenol or a mixture of polyphenols inhibited NADPH oxidase.29 The present results further extend these findings as EC, at concentrations commonly found in the human circulation after dark chocolate administration,24 inhibited platelet ROS generated by NADPH oxidase activation and increased NO production. It remains to be established whether the increase of NO production also occurs at endothelial levels and accounts for the vasodilatation effect elicited by dark chocolate.
The study has implications and limitations. We have no evidence of the antioxidant effect of dark chocolate in a long-term follow-up. Therefore, further study is necessary to see whether, in patients with enhanced markers of oxidative stress and impaired FMD, chronic administration is clinically effective. In this context the study should be considered a proof-of-concept study aimed at analysing the intrinsic mechanism through which dark chocolate affects artery dilatation; no clinical implication can be deduced. It is relevant to underscore, however, that the antioxidant property as well as the vasodilatation property of dark chocolate were not detected in HS.
This suggests that molecules such as polyphenols or vitamins can hardly exert any antioxidant activity in patients without oxidative stress and normal antioxidant status.30 Despite the fact that this was not a double-blind study, the blinding of authors and laboratory technicians minimised such bias.
In conclusion, the study provides evidence that in smokers, but not in HS, acute administration of dark chocolate is associated with enhanced FMD. Such an effect is attributable to the inhibition of NOX2-related oxidative stress elicited by polyphenols. The study warrants further investigation to analyse the long-term effects of dark chocolate in patients at risk of cardiovascular disease.
Acknowledgments
The authors wish to thank nurses Monica Brancorsini and Daniela Salzano for their skilful cooperation.
References
Footnotes
Funding This study was supported by a grant from the University of Rome “La Sapienza” (Ateneo Federato 2009) (funds to LL and FV).
Competing interests None.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the Sapienza University of Rome Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.