Article Text

Abstract
Objective To assess the evidence for a reduced risk of acute coronary events following comprehensive smoke-free legislation.
Methods Two independent systematic reviews were undertaken using PubMed, Embase and Science Direct with no date restrictions imposed. Meta-analysis was undertaken using a random effects model to obtain a pooled estimate of the relative risk. Linear regression was used to examine possible bias and meta-regression was used to investigate possible causes of heterogeneity.
Main outcome measure Acute coronary events.
Results The 17 eligible studies (10 from North America, 6 from Europe and 1 from Australasia) provided 35 estimates of effect size. Apart from five subgroup analyses, all of the published results suggested a reduction in the incidence of acute coronary events following the introduction of smoke-free legislation. Meta-analysis produced a pooled estimate of the relative risk of 0.90 (95% CI 0.86 to 0.94). There was significant heterogeneity (overall I2=95.1%, p<0.001) but there was no evidence of small study bias (p=0.714). On univariate random effects meta-regression analysis, studies with longer data collection following legislation produced greater estimates of risk reduction and remained significant after adjustment for other study characteristics (adjusted coefficient −0.005, 95% CI −0.007 to −0.002, multiplicity adjusted p=0.006).
Conclusions There is now a large body of evidence supporting a reduction in acute coronary events following the implementation of comprehensive smoke-free legislation, with the effect increasing over time from implementation. Countries that have not yet adopted smoke-free legislation should be encouraged to do so.
- Legislation
- meta-analysis
- myocardial infarction
- tobacco smoke pollution
- smoking
- acute coronary syndrome
- public health
Statistics from Altmetric.com
- Legislation
- meta-analysis
- myocardial infarction
- tobacco smoke pollution
- smoking
- acute coronary syndrome
- public health
Introduction
In 2003 the World Health Organization ratified its first international public health treaty, the Framework Convention on Tobacco Control (FCTC) (http://www.who.int/fctc/en/). The FCTC set out a legislative framework for tobacco control including recommendations on the development, implementation and enforcement of national comprehensive smoke-free legislation. To date, 164 countries are signatories to the FCTC. Smoke-free legislation, consistent with the FCTC recommendations, has now been introduced in many countries including the Republic of Ireland, Norway, New Zealand, Italy, France and the UK, as well as a growing number of US states and Canadian provinces. Owing to its scale of coverage, smoke-free legislation has the potential to achieve vast public health benefit if it is effective in reducing the risk of smoking-related conditions such as cardiovascular disease. The effect of introducing comprehensive smoke-free legislation on acute coronary events has now been studied in a number of countries. This paper describes a systematic review and meta-analysis of the findings to date.
Methods
Two of the authors (MOI and JPP) conducted independent systematic reviews using the PubMed, Embase and Science Direct databases. Exploded search terms were applied to the titles, abstracts, MeSH terms and keywords of publications (smok* OR tobacco OR cigarette*) AND (legislation OR ban OR bans OR restriction* OR law OR laws OR smoke free OR smokefree) AND (cardiac OR cardiovascular OR myocardial OR coronary). The search was restricted to studies on humans that were published in or translated into English. No date restrictions were applied.
Eight hundred and seventy-four articles were identified, of which 477 were discarded as duplicates (figure 1). Review of the remaining 397 titles enabled us to exclude a further 107 studies as irrelevant. The abstracts of the remaining 290 were reviewed and 183 were excluded as ineligible because they examined only workplace or voluntary restrictions, focused on subgroups of the general population such as bar workers or did not provide estimates of effect size. Of the remaining 107, 16 were confirmed as eligible original studies.1–16 The other 91 publications were relevant but were review articles, meta-analyses or editorials. Their text and publication lists were checked for relevant studies not otherwise identified. This provided details of one unpublished conference abstract, a copy of which was obtained from the investigators.17 Therefore, a total of 17 original studies were suitable for inclusion in the qualitative synthesis.1–17

Flow diagram of systematic review.
Of the 17 studies that satisfied the eligibility criteria, 15 had been published in peer-reviewed journals1–11 13–16 and 2 had not.12 17 One of the latter studies could not be included in the meta-analysis because it did not provide the information necessary to calculate relative risk and confidence intervals.12 The other had only been reported as a conference abstract but was nonetheless included.17 One of the earlier studies2 was followed by a second publication with longer follow-up information in the same population.3 Only the most recent results were included in the meta-analysis.3 A study conducted in New York reported an 8% reduction in hospital admissions for acute myocardial infarction following the introduction of comprehensive smoke-free legislation.5 The investigators estimated that the decline would have been 19% had there been no prior restrictions. We used the conservative estimate of 8% in our primary analyses, but also repeated the meta-analysis using 19%. One study reported results from four Italian regions,11 one of which had already been reported individually.4 The results for the three new regions were entered separately into the meta-analysis and the fourth region was not duplicated. Where studies reported separate relative risks for different age subgroups,4 10 13 14 sexes4 9 10 13 14 or for premature and non-premature events,4 9 10 14 these were entered separately into the meta-analysis. The meta-analysis was therefore based on a total of 35 estimates of relative risk obtained from 17 studies.
Where population denominators were not provided in the paper, they were obtained from the official government censuses in the relevant country for adults aged ≥18 years in 2000. For studies conducted in the USA, data were obtained from the US Census Bureau website (http://factfinder.census.gov/home/saff/main.html?_lang=en). Italian populations were obtained from the National Institute of Statistics (ISTAT) (http://www.istat.it/english/) and the population of Saskatoon in Canada was obtained via direct correspondence with the Saskatoon Department of Health. Data on the population of Scotland were obtained from Scotland's Census Results Online (SCROL) obtained via the General Register Office for Scotland website (http://www.scrol.gov.uk/scrol/common/home.jsp and population data for New Zealand were obtained from Statistics New Zealand (http://www.stats.govt.nz/Census/2006CensusHomePage/Tables/AboutAPlace/SnapShot.aspx?id=2000060&tab=Agesex&ParentID=1000013&type=ta).
All analyses were undertaken using STATA 10.1 software. The user written “metan” command was used to produce a forest plot to illustrate the contributions of individual studies in terms of their estimated effect size and the 95% CI associated with these. The individual studies were conducted in different countries and circumstances. We therefore used a random effects model which allows for non-random variability in effect estimates between studies and adjusts confidence intervals accordingly. The studies were stratified according to the study population size, age group and sex investigated. We produced a funnel plot which allows for widening 95% CI lines with decreasing study size. In the absence of significant heterogeneity, 95% of all studies should lie within these lines and, in the absence of small study bias, the plotted results should be symmetrical. In addition to visual assessment of the funnel plot, we undertook the more formal test of Egger.18 The study characteristics that might account for heterogeneity were investigated using meta-regression via the user written ‘metareg’ command for Stata. Meta-regression analysis can be prone to type I errors because the number of studies is typically low and heterogeneity between studies is common. To reduce the risk of an erroneously large pooled estimate of effect size, we used Monte Carlo simulation to adjust all p values for multiple testing using the ‘permute’ subcommand available within the ‘metareg’ main command. A cumulative meta-analysis was undertaken to investigate the extent to which the pooled estimate may have changed over time.
Results
The systematic review identified 17 eligible studies (10 conducted in North America, 3 in Italy, 3 in Great Britain and 1 in New Zealand). Only one study employed prospective data collection.9 The case definitions used in the studies varied and included myocardial infarction,1–7 11 13–16 acute coronary syndrome,9 17 coronary heart disease including angina and heart failure,8 and myocardial infarction plus ischaemic heart disease.10 Some studies included individuals for whom myocardial infarction was recorded in the secondary position.1 2 4 7 10 Exclusion criteria varied but included patients who had previously undergone coronary revascularisation procedures,1 7 patients with comorbid conditions such as hypertension and dyslipidaemia7 and patients who had suffered a prior event over the study period.13 All of the published studies included people hospitalised for eligible events but only two studies took account of prehospital deaths.2 3 10
All of the studies included a before and after comparison of events. Seven also included a geographical comparison group from an area in which legislation had not yet been implemented.1–3 7–9 15 16 The earlier studies, predominantly from the USA, tended to focus on small geographically-isolated communities served by one or two hospitals1–3 7 8 while later studies tended to cover larger populations of over one million.4 5 9 10 14–16 The post-legislation period covered in the studies ranged from 5 to 84 months, with 12 studies reporting results to at least 12 months post-legislation.2 4–9 12–17 Two studies provided population level data on changes in smoking prevalence,4 6 but only four were able to classify individual patients by smoking status.7 9 13 17 Two studies provided population level data on changes in environmental tobacco smoke (ETS) exposure6 10 but only one had access to individual level data.9 Four studies provided subgroup analyses by age,4 10 13 14 five reported subgroup analyses by sex4 9 10 13 14 and four reported separate results for premature and non-premature events.4 9 10 14
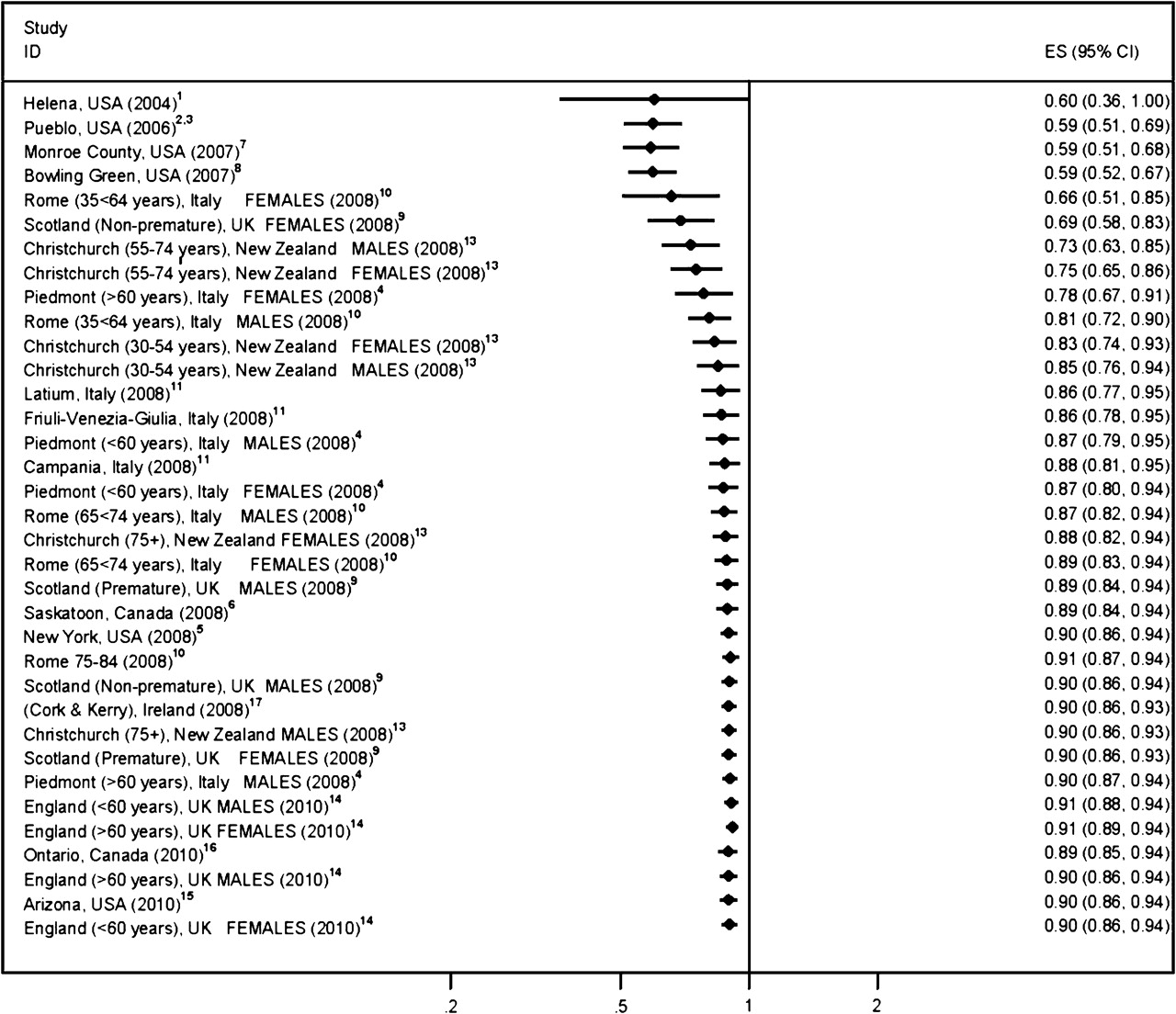
The 17 studies provided 35 estimates of relative risk. In five of the subgroup analyses (women and men >60 years in Piedmont, Italy,4 women >65 years in Scotland9 and men and women 30–54 years in Christchurch, New Zealand13) the risk of acute coronary syndrome was not reduced following implementation of smoke-free legislation (figure 2). Of the 30 results suggesting a reduced risk, 18 reached statistical significance. In the stratified random effects meta-analysis, the pooled estimate of risk reduction was 10% (95% CI 6 to 14, p<0.001, Figure 2). The overall I2 was 95.1%, suggesting significant heterogeneity (p<0.001). In the stratified analysis, heterogeneity was high in all strata except for large-scale studies that reported sex-specific results for premature events where heterogeneity was only moderate.16 The funnel plot provided additional evidence of significant heterogeneity between the studies, but there was no visual evidence of significant asymmetry or small study bias (figure 3). Formal testing confirmed that, although the smaller studies did produce larger estimates of risk reduction, the association did not reach statistical significance (Egger's regression test: bias coefficient −0.387, 95% CI −2.520 to 1.746, p=0.714). The cumulative meta-analysis showed that the early studies provided relatively large but imprecise estimates of effect size but, with subsequent studies, the pooled estimate converged to a smaller but statistically significant estimate of a 10% reduction (figure 4).

Forest plot of stratified random effects meta-analysis of studies examining the effect of smoke-free legislation on acute coronary events.
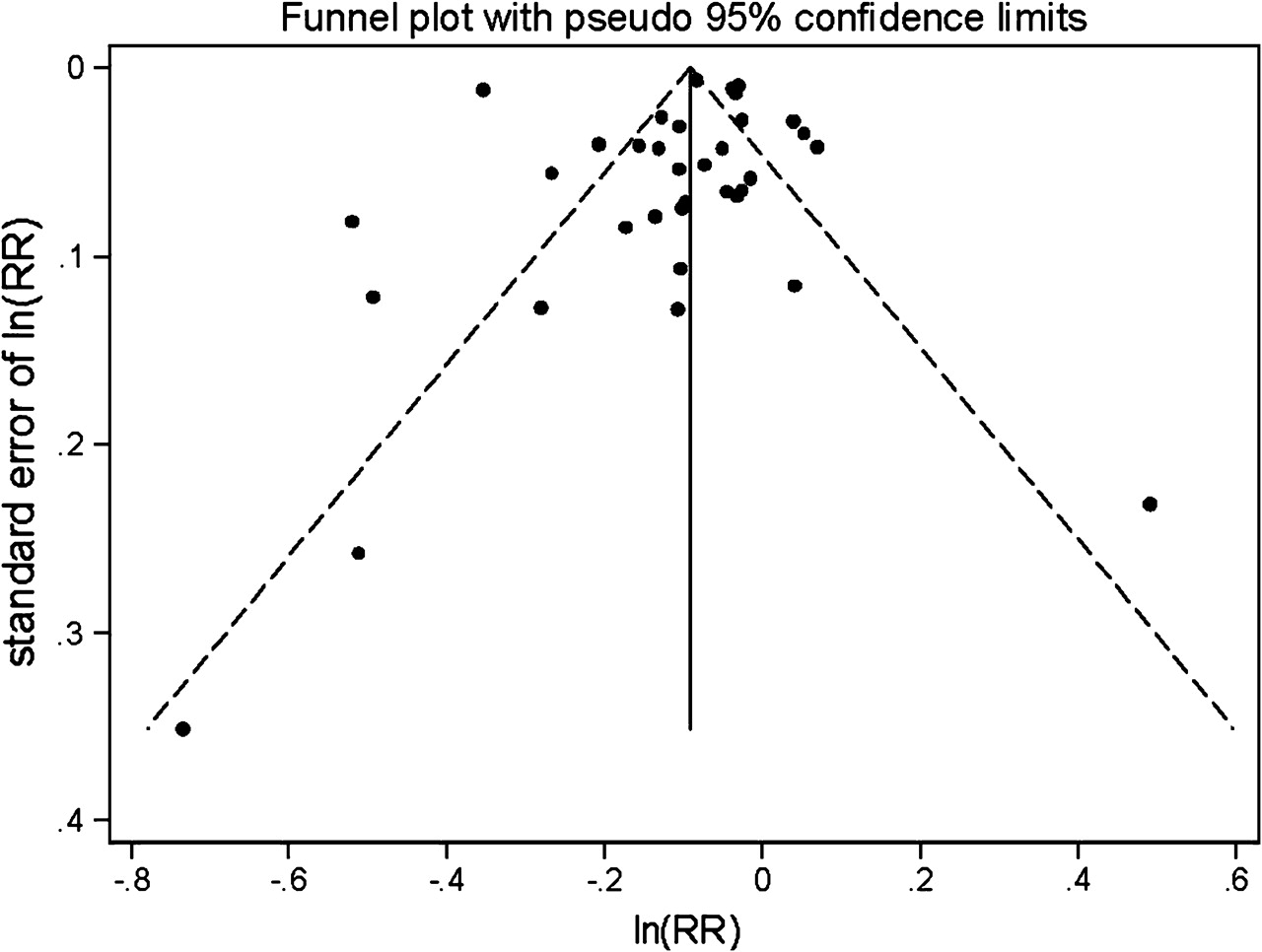
Funnel plot to illustrate possible small study bias among studies examining the effect of smoke-free legislation on acute coronary events.

Cumulative meta-analysis of studies examining the effect of smoke-free legislation on acute coronary events.
In the univariate meta-regression analysis, study location and age category were significantly associated with estimated effect size (table 1). However, they were no longer significant predictors after adjustment for other study characteristics. Length of follow-up after legislation was the only independent predictor of effect size estimate in the multivariate meta-regression analysis (table 1). There was a dose gradient whereby the longer data were collected following implementation of legislation, the greater the reduction in acute coronary events (figure 5). The adjusted R2 for the meta-regression was 57.8%. Residual variation due to heterogeneity was 72.6% after controlling for various confounders, suggesting that the remaining variation is systematic rather than due to sampling variation or chance. Remaining variance was small with τ2=0.006. When we re-ran the meta-analysis inputting the New York study as showing a 19% reduction rather than 8%, the pooled estimate changed from 10% (95% CI 6% to 14%) reduced risk to 11% (95% CI 6% to 15%).5
Random effects meta–regression analysis of studies examining the effect of smoke-free legislation on acute coronary events

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Bubble plot* of the univariate relationship between length of data collection after legislation and log relative risk (RR).
Discussion
There is now a large body of research that provides consistent evidence of the effectiveness of smoke-free legislation. The pooled information from these studies suggests that acute coronary events fall by around 10% following the implementation of legislation. Our study provides an up to date meta-analysis of the existing literature. There are now 17 studies providing 35 results, sufficient to enable us to examine the extent to which study design and geographical differences in baseline smoking behaviours, attitudes and ETS exposure may have influenced the results. Early small studies tended to produce larger estimates of effect than more recent larger studies, but we found no evidence of significant study size bias and the more robust studies conducted in recent years have nonetheless demonstrated a reduction in events. It is reassuring that, in the meta-regression analysis, the magnitude of effect demonstrated by studies was not significantly associated with the study population size, age category, sex, study location or year of publication, suggesting that the overall finding of benefit was robust. Data are now available for up to 7 years following legislation. Our meta-regression showed that the reduction in events was greatest in studies with longer follow-up, suggesting that the beneficial effect of legislation increases over time from implementation. This is corroborated by the Scottish study which demonstrated an increase in the reduction in events when comparing figures month by month from time of implementation.9
Our meta-analysis has a number of limitations. We synthesised aggregated data from individual studies. Ideally, we would have used individual level data. However, this was not feasible since a number of individual studies themselves used aggregated routine data. There are currently insufficient relevant studies for us to examine the effects of smoking status and socioeconomic status on benefit. The lack of information in these areas needs to be addressed in future studies. Ideally, we would have examined whether there was evidence for a dose effect in terms of baseline level of exposure to ETS exposure and level of compliance with the legislation. However, the necessary data are not available.
The introduction of comprehensive smoke-free legislation has resulted in an immediate fall in ETS19 20 that has been sustained over time.21 22 Two weeks after implementation of the Scottish legislation the levels of small particulate matter (PM2.5) in bars had fallen by 86%.19 Within 6 weeks following implementation of the Irish legislation, salivary cotinine concentrations among hotel workers had fallen by 69% and air nicotine concentrations had fallen by 83%.20 At 9 months follow-up, adults in the general population reported a 95% reduction in ETS exposure in bars and a 96% reduction in restaurants.23 One year after the introduction of workplace bans in Finland, air nicotine concentrations had fallen by 75–96%24 with further reductions occurring over the subsequent 2 years.22 One year after introduction of the Italian legislation <10% of the general population reported exposure to ETS in hospitality settings.25 In Scotland, compliance with the legislation was immediate19 and the most recent enforcement data available from Environmental Health Officers indicate that 97% of premises inspected were still compliant nearly 2 years after the legislation was introduced. Among the Scottish adult non-smoking population, mean cotinine concentrations fell by 39%.26 Data from California suggest that the early compliance observed among both patrons and employees increased over the 10–12 years following legislation.21
ETS is a recognised risk factor for many diseases but appears to be particularly toxic to the vascular system. Many toxic gases are present in higher concentrations in sidestream smoke than mainstream smoke. Exposure to ETS rapidly induces platelet aggregation, thrombosis, endothelial dysfunction and inflammation27 and is associated with plasma concentrations of homocysteine, C-reactive protein, fibrinogen and oxidised LDL cholesterol comparable to those in active smokers.28 Even occasional exposure to ETS increases the risk of acute coronary syndrome.28 Our results suggest that the fall in ETS that follows introduction of legislation is translated into a significant reduction in acute coronary events. Smoke-free legislation has the potential to produce immediate and significant reductions in ETS exposure across large populations. Acute coronary events remain a major cause of death and morbidity in developed countries and are increasing in importance in developing countries where smoking prevalence is also increasing. The reduction in acute coronary events demonstrated in our meta-analysis therefore translates into a large public health benefit. Countries that have not yet implemented comprehensive smoke-free legislation should be encouraged to do so.
References
Footnotes
Funding NHS Health Scotland project grant.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.