Article Text

Abstract
Background In December 2019 a novel coronavirus designated SARS-CoV-2 was identified, and the disease COVID-19 has caused many deaths. SARS-CoV-2 infection has been associated with the development of cytokine storm (including interleukin 6 (IL-6)), which can cause lung damage and lack of oxygen. Tocilizumab (TCZ) inhibits ligand binding to the IL-6 receptor and may be a potential treatment for the hyperinflammation symptoms of COVID-19. However, data regarding the efficacy of TCZ in COVID-19 are lacking. The rapid spread of the pandemic in France, especially in the Paris region, constrained us to the off-label use of TCZ in patients with severe clinical conditions.
Methods A single-centre observational cohort study of 44 patients infected with COVID-19 was carried out between 6 April and 21 April 2020 in Groupe Hospitalier Intercommunal Le Raincy-Montfermeil (GHILRM). Twenty-two patients diagnosed with COVID-19 were treated with TCZ and were compared with 22 patients not treated with TCZ matched for age, gender and length of hospital stay for COVID-19. Respiratory rate and oxygen supplementation as well as laboratory parameters (such as C-reactive protein (CRP), aspartate aminotransferase and alanine aminotransferase) were collected at baseline and during 14 days of follow-up. Our primary objective was to assess the efficacy of TCZ on respiratory clinical conditions.
Findings The average respiratory rate was lower in the TCZ group than in the control group (21.5 vs 25.5 breaths/min at day 14, 95% CI −7.5 to −0.4; p=0.03). Treated patients tended to be intubated less during the course of the disease (2/22 vs 6/22, 95% CI −0.4 to 0.1; p=0.12). In each group, 10 patients no longer required oxygen therapy. We found a significant decrease in CRP in treated patients on day 7 (p=0.04). TCZ caused cytolysis in more than half (14/22) of the patients but without clinical impact.
Interpretation There was a significant difference in the respiratory rate on day 14 of follow-up, with a greater decrease observed in the treated group. Fewer patients required mechanical ventilation in the TCZ group, especially among patients with more extensive CT lung damage, than in the control group. The same number of patients were weaned off oxygen on day 14 in the two groups, while the patients in the TCZ group had more severe impairment at inclusion. We consider that TCZ showed significant control of the biological inflammatory syndrome, suggesting that it may limit the effect of the cytokine storm. Our study seems to indicate the efficacy of TCZ, particularly in patients with severe initial pulmonary impairment. Selecting the best candidates and the best timing for TCZ therapy needs to be determined in randomised clinical trials.
- pulmonary medicine
- virology
- critical care
- pharmaceutical preparations
- clinical medicine
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Introduction
In December 2019 the Wuhan Municipal Health Committee identified an outbreak of viral pneumonia cases of unknown cause. A novel coronavirus has been designated SARS-CoV-2, and the disease caused by this virus has been designated COVID-19. This novel coronavirus spread in 3 months to all continents. The infection was declared a pandemic by the World Health Organization on 11 March 2020.
In mild cases the infection causes fever, dry cough and asthenia.1 Ageusia and anosmia also appear to be frequent clinical features in patients with COVID-19.2 However, some patients (15%) suddenly deteriorate 7–8 days after the appearance of the symptoms and develop severe pneumonia and acute respiratory distress syndrome (ARDS).3 There is growing evidence that virally-induced pro-inflammatory cytokines lead to hyperinflammation.4 An acute severe systemic inflammatory response known as cytokine storm leads to severe and critical disease. One of the cytokines involved is interleukin 6 (IL-6),5 6 which is considered to be a key mediator of the cytokine storm causing the deterioration. Raised IL-6 levels have been reported in patients with COVID-19 and are sometimes associated with disease severity.7
Currently, there is no proven treatment for patients with this novel infection. In the context of the COVID-19 pandemic and growing tensions worldwide regarding healthcare facilities, there is an urgent need for effective treatments. Many different molecules are being considered as possible treatments for COVID-19, but none have so far been found to be really effective.
Tocilizumab (TCZ) is a humanised anti-human IL-6 receptor monoclonal antibody, which may be a possible strategy for patients with cytokine storm.8 Data on this off-label use of TCZ in the treatment of COVID-19 are still preliminary.
It is currently unclear which patients may benefit from TCZ. Preliminary results from clinical trials are expected to be available soon. In March and April 2020 we used TCZ off-label in patients with severe COVID-19 based on its hypothetical benefit, and report on the experience of our general hospital.
Materials and methods
This is a single-centre observational cohort study of patients infected with COVID-19 and treated with TCZ between 6 April and 21 April 2020 at our general hospital. We recorded several data every day from admission to 14 days after injection of TCZ. Clinical parameters such as respiratory rate and oxygen supplementation were measured daily. Laboratory parameters (C-reactive protein (CRP), lymphocytes, aspartate aminotransferase (AST) and alanine aminotransferase (ALT)) were measured at the clinician’s discretion and collected from baseline to day 14.
Due to high costs, lack of knowledge and safety risks, a multidisciplinary ethics committee validated the use of TCZ for each patient . Patient consent was requested and marked in the patients’ records. Patients received TCZ after agreement by the multidisciplinary ethics committee.
The criteria for receiving TCZ were:
Hospitalised patients with a positive diagnosis of COVID-19 (by real-time PCR on nasopharyngeal swabs)
Extensive bilateral lesions in the lungs
Severe respiratory insufficiency needing oxygen supplementation (≥5 L)
Clinical aggravation
Increased CRP level
No major contraindications to the drug.
Research of infections including tuberculosis was performed before TCZ use by a test to detect the production of gamma interferon (interferon-γ release assays; Quantiferon).
We compared the parameters of hospitalised patients with a positive diagnosis of COVID-19 with a group of patients withf the same sex ratio, comparable age and with relatively similar impairment who had not been treated with TCZ. Patients were compared at similar times of disease progression compared with onset of symptoms.
However, as our study was an observational study and not a clinical trial, all patients with severe disease and without contraindications were treated. Patients in the control group therefore necessarily had more moderate impairment than the group of treated patients, although their profile was similar. This allowed us to compare the effect of TCZ versus control. The comparison with untreated patients also makes it possible to assess the events linked to the SARS-CoV2 infection itself.
TCZ was prescribed at a fixed dose of 600 mg for patients <100 kg and 800 mg for those >100 kg. These fixed doses were determined on the basis of 8 mg/kg but with a rounding which allowed the use of whole vials (Roactemra 200 mg and 400 mg). Given the high cost and the quota of this drug, this enabled us not to waste the product (opened vials are not sufficiently stable and patients are not always treated on the same day). There was no need to adjust the dose in patients with renal insufficiency. The dose was diluted to 100 mL with 0.9% sodium chloride and the intravenous infusion time was more than 1 hour. A second dose (same dose as the first injection) was given after 48 hours in cases with insufficient response to the treatment.
Analysis of data
Descriptive statistics were used for demographic, laboratory and clinical data. Continuous variables were expressed as mean (SD) and compared using the ANOVA test. Categorical variables were expressed as number and compared between the two groups by the Student t-test. A p value of <0∙05 was considered significant. The online test BiostaTGV (INSERM) was used. Statistical analysis was also performed using Microsoft Excel and RStudio Team 2019 (Integrated Development for R, RStudio, Boston, Massachusetts, USA).
Results
Population characteristics
Data were collected from 44 patients, 22 receiving TCZ and 22 not receiving TCZ. The characteristics of the patients are shown in table 1. The study population consisted of 31 men and 13 women with a median age of 65 years (range 41–82). The mean body mass index (BMI) was 28 kg/m2 (range 16–45). In the TCZ group the mean age was 64 years (range 41–80), with a male/female ratio of 16/6 and a mean BMI of 29 kg/m2 (range 22–45). In the control group the mean age was 65 years (range 41–82), with a male/female ratio of 15/7 and a mean BMI of 26 kg/m2 (range 16–33).
Patient characteristics
The groups were comparable with regard to age (95% CI −5.8 to 8.5) (p=0.70) and BMI (95% CI −0.6 to 7.3) (p=0.09).
Symptoms
The most commonly reported symptoms were fever (25/44 patients, 57%), dyspnoea (23/44, 53%), asthenia (19/44, 43%) and cough (13/44, 29%). Some patients had diarrhoea (6/44, 14%), body aches (5/44), anosmia (3/44), ageusia (2/44) and rhinitis (3/44). The mean duration between the onset of the first symptoms and hospitalisation in the TCZ and control groups was 7 days and 7.2 days, respectively.
Comorbidities
Twenty patients had hypertension. Some of the patients were overweight (14/44) or obese (11/44). Ten patients had cardiovascular comorbidities (heart failure or atrial fibrillation) and seven patients had diabetes mellitus.
In the TCZ group, hypertension (7/22) and obesity (8/22) were the most common comorbid conditions. Other cardiovascular disease (heart failure or atrial fibrillation) occurred in seven patients. Three patients had diabetes mellitus and two had no known comorbidities.
In the control group, hypertension was the principal comorbidity (13/22). The patients in this group had slightly lower BMI (three obese (BMI >30)). Four patients had other cardiovascular diseases, three patients had diabetes mellitus and three had no known comorbidities.
Lung damage
In the TCZ group the severity of lung damage on CT scanning was worse than in the control group, varying from <50% (6/22) to >50% (9/22) and >75% (2/22). Four patients had less than 25% of lung damage on the first CT scan and one patient did not have a CT scan.
In the control group most patients had less lung damage. Six patients had 25–50% lung damage on the first CT scan, four had more limited involvement (<25%), two had <10% lung damage and three were not evaluated by CT. The lung damage was more severe in seven patients (six had 50–75% and one had >75%).
Length of stay
The average length of stay for treated and untreated patients with COVID-19 was 15 and 13 days, respectively.
Other treatment
In the TCZ group, two patients had received hydroxychloroquine and azithromycin prior to treatment with TCZ and four patients had received azithromycin monotherapy. In the control group, three patients had received hydroxychloroquine and azithromycin. The majority of patients therefore did not receive any other treatment. No difference was noticed between the groups.
Tocilizumab treatment
Twenty patients received two TCZ administrations and two patients received one (one patient died and the other patient could not receive the second injection because of several complications which contraindicated a further injection (myocardial infarction)).
On average, patients received the first injection of TCZ 10 days after the onset of symptoms (range 3–21 days). We did not notice any difference in response according to the time of injection.
Clinical and respiratory data
On admission to hospital all the patients in the TCZ group had tachypnoea and the average respiratory rate was 33.7 breaths/min. In the control group 16 patients had tachypnoea when they arrived at hospital with an average respiratory rate of 31.2 breaths/min (95% CI −2.8 to 7.9) (p=0.34).
We calculated the average respiratory rate in the two groups in patients on spontaneous ventilation (excluding intubated patients) on days 7 and 14 of follow-up to analyse the variation in respiratory rate in the two groups. In the TCZ group the average respiratory rate on day 7 was 24.7 breaths/min compared with 23.7 breaths/min in the control group (95% CI −4.5 to 2.5) (p=0∙57) and on day 14 the average respiratory rate was 21.5 breaths/min in the TCZ group and 25.5 breaths/min in the control group (95% CI −7.5 to −0.4) (p=0.03).
Supplementary oxygen
We compared the two groups according to the ventilatory parameters on days 7 and 14 of follow-up.
On day 7, four patients in the TCZ group and five patients in the control group required mechanical ventilation. One patient in each group was on High Flow Nasal Oxygen Therapy (Optiflow). Thirteen patients in the TCZ group required oxygen therapy compared with nine in the control group. On day 7, fewer patients required oxygen in the control group (two patients in the TCZ group were oxygen-free compared with seven patients in the control group). The average oxygen flow rate was calculated from the flow rates required for each patient; the average oxygen flow rate of the TCZ group on day 7 was 5.76 L/min compared with 5.75 L/min in the control group.
At day 14, in the TCZ group three patients required mechanical ventilation and six in the control group. One patient in the control group was on High Flow Nasal Oxygen Therapy but none in the treated group. Six patients in the TCZ group required oxygen therapy compared with three in the control group. In each group, 10 patients no longer required oxygen therapy. However, there was a difference in the average oxygen flow between the two groups at this stage; the average oxygen flow rate was 4.3 L/min in the TCZ group and 6.3 L/min in the control group (95% CI −11.6 to 7.6) (p=0.56).
The average duration for oxygen withdrawal was 10.8 days for the TCZ group and 6.4 days for the control group (95% CI −7.2 to −1.6) (p=0∙003).
Half of the patients in the TCZ group (n=11) were weaned off oxygen in 14 days (or less) and in the control group 10 patients needed no oxygen after 14 days (or less). Four patients were receiving invasive mechanical ventilation in the treated group versus six in the control group.
Subgroup of patients with severe initial CT involvement
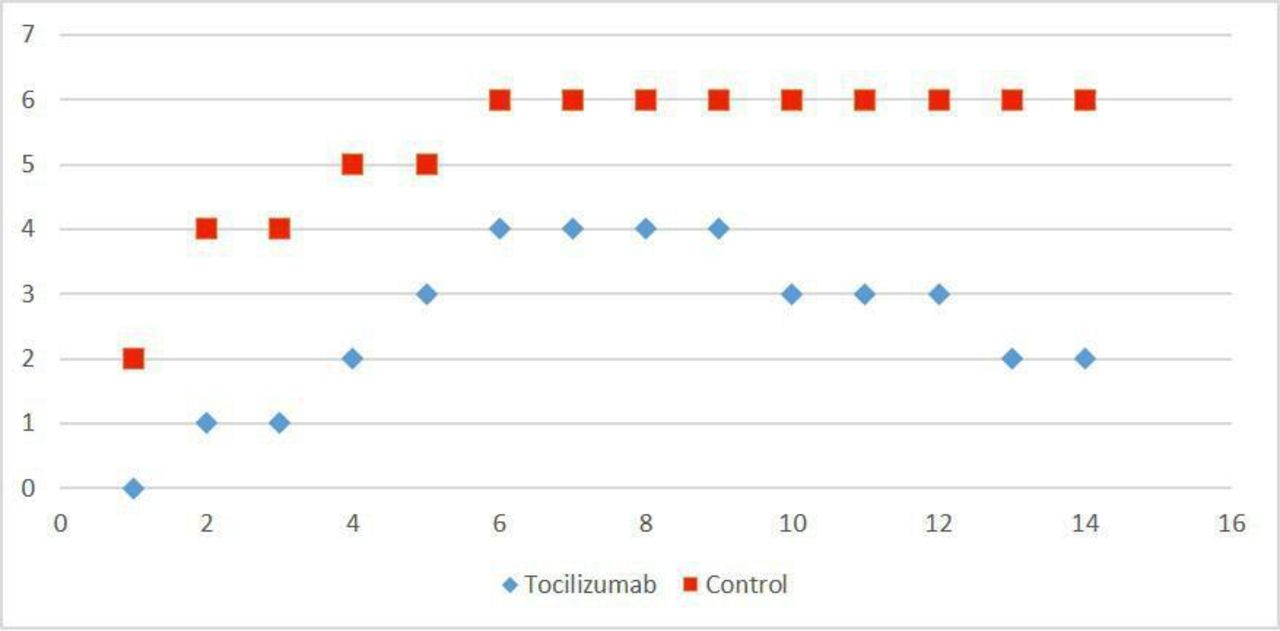
We analysed the patients according to their degree of involvement on the chest CT scan performed at the start of each patient's hospitalisation. We were interested in patients with >50% CT damage according to the recommendations of the European Radiology Society. On admission, 11 patients in the TCZ group had >50% involvement compared with seven in the control group (95% CI −0.1 to 0.5) (p=0.23). On day 14, in the TCZ group two patients required invasive ventilation compared with six in the control group (95% CI −0.4 to 0.05) (p=0.12) (figure 1).

Evolution of number of patients with >50% CT lung damage requiring mechanical ventilation.
One death occurred in the treated group and none in the control group. Three patients in the TCZ group were still requiring oxygen with an average flow of 3 L/min versus one patient in the control group with a flow of 6 L/min (95% CI −11.5 to 7.5) (p=0.55). Five patients in the TCZ group were no longer oxygen-dependent compared with none in the control group (figure 2).

Evolution on day 14 of patients with CT lung damage >50%.
Laboratory data
Lymphocytes
In the TCZ group 15 patients were found to be lymphopenic on arrival with an average lymphocyte count of 0.60 g/L (range 0.2–0.9) compared with seven patients in the control group with an average count of 0.69 g/L (range 0.2–0.9) (95% CI −0.5 to 0.1) (p=0.21).
CRP
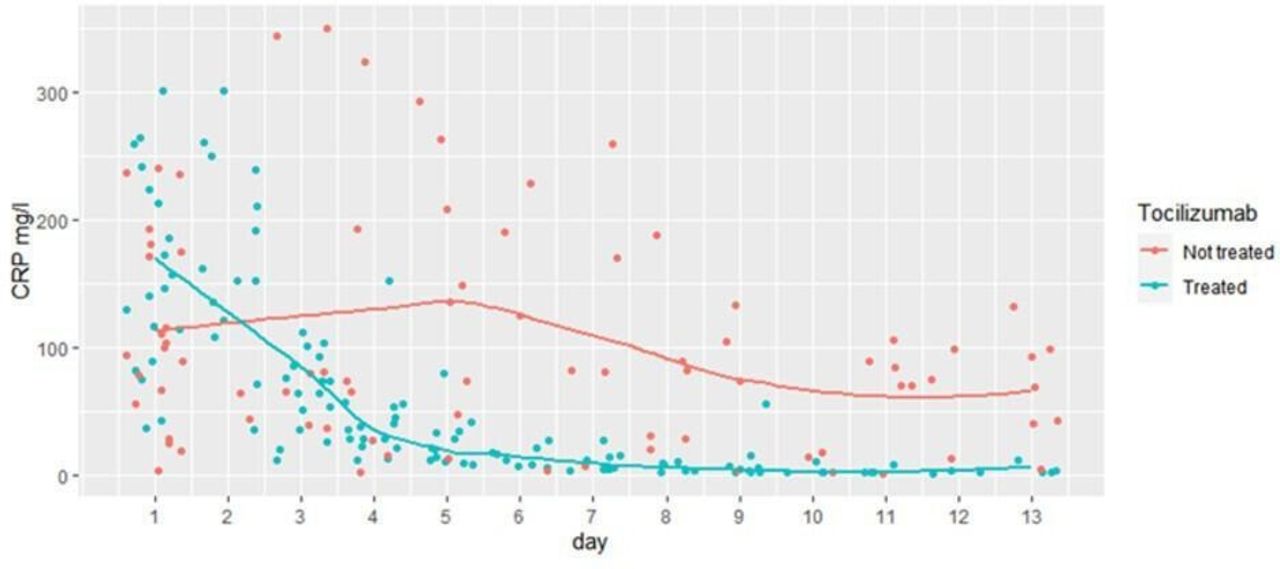
All patients had hyperinflammation with raised CRP levels when they were admitted to hospital (median value of 147 mg/L in the control group and 101.5 mg/L in the TCZ group). The CRP levels decreased significantly in patients treated with TCZ from 147 mg/L (median) to 36 mg/L in 3 days.
In the days following the injection of TCZ we noted that the treated patients had lower CRP values than the untreated patients (median 36 mg/L in the TCZ group vs 65 mg/L in the control group at day 3) (95% CI −166.6 to 50.4) (p=0.24). At day 7 the difference was significant with a median of 6.5 mg/L in the TCZ group and 56.5 mg/L in the control group (95% CI −133.3 to −0.3) (p=0.04), and this was even more marked in the following 10 days. The CRP value in the treated patients returned to the normal or near normal range within 10 days but, in the control patients, the CRP was not negative within 10 days (figure 3).
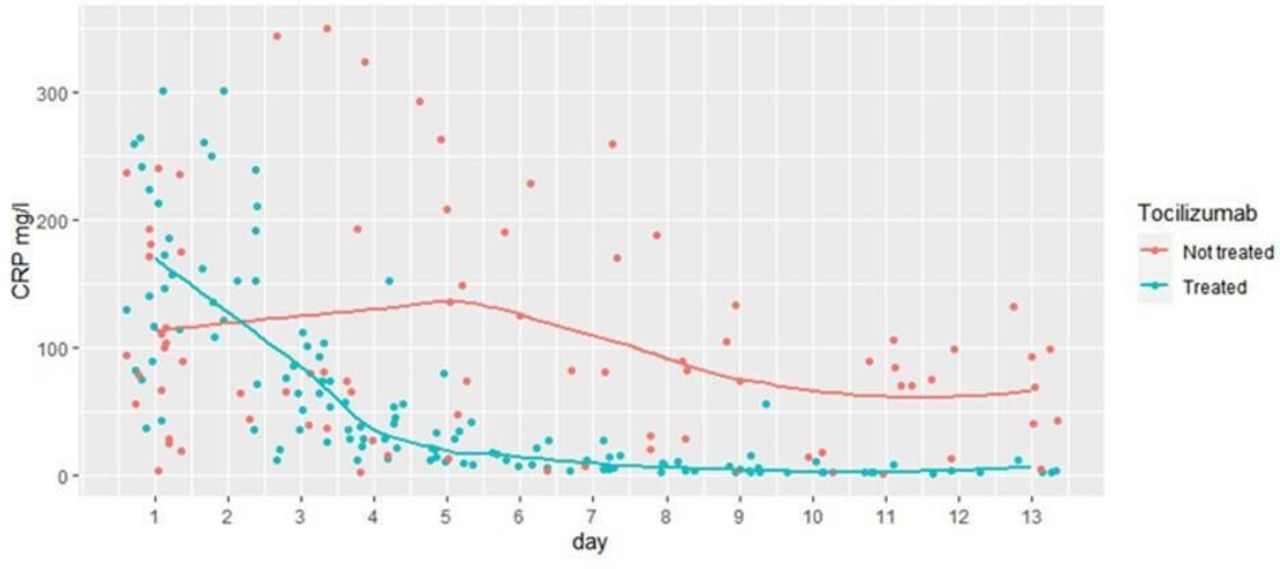
Evolution of C-reactive protein (CRP) over time.
AST and ALT
Fourteen of the 22 patients (64%) in the TCZ group developed cytolysis on days 4 or 5. The median AST level rose from 54 IU/L to 1018 IU/L in 5 days in the TCZ group while, in the control group, the median level was 44 IU/L at admission and 47 IU/L at day 5 (p<0∙002). The values returned to normal in the TCZ group at day 13. Given the chronology of occurrence and the difference between the two groups, this hepatic toxicity is attributed to TCZ and not to SARS-CoV-2 (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Evolution of aspartate aminotransferase (AST) and alanine aminotransferase (ALT) over time.
Other adverse effects
No infusion reactions were observed.
An increased risk for infection due to TCZ is an expected adverse effect, but no nosocomial infection was reported. The occurrence of secondary infection does not seem to be frequent with short-term treatment.
Patients’ outcome
Twenty patients returned home, 10 from each group. Five patients died, three in the treated group and two in the control group. Two patients were transferred to another hospital to have extracorporeal membrane oxygenation (ECMO), one from each group. Five patients in the control group were transferred for continuation of medical care in another establishment. The remaining 12 patients are still hospitalised at the time of writing this article.
Discussion
In this study we examined the effect of TCZ treatment of patients with COVID-19 in real life in our general hospital. The Chinese Health Commission included TCZ in its seventh edition of COVID-19 therapy national guidelines. In Italy, in case of rapid worsening, the national guidelines of the Italian Medicines Agency (AIFA) also support the use of TCZ. In most uses of TCZ in COVID-19 the dose is that approved to manage cytokine release syndrome (CRS) in CAR T-cell recipients—that is, 8 mg/kg up to a maximum dose of 800 mg. Some give a smaller fixed dose of 400 mg. However, Reid et al in Illinois9 proposed that potentially lower doses may be sufficient. To evaluate this hypothesis they performed a 50-person trial in April named COVIDOSE, which involves patients hospitalised with COVID-19 but not yet in need of mechanical ventilation. The patients received 80 mg or 200 mg of TCZ, depending on their risk of complications. This lower-dose strategy, if proven effective, could help address any shortages of TCZ that arise as the COVID-19 pandemic continues and could minimise the cost of the treatment. Luo et al 10 reported that repeated doses of TCZ might improve the condition of critically ill patients. They also conclude the possible effectiveness of a small dose. In another study, Sciascia et al 11 used intravenous TCZ (8 mg/kg) or subcutaneous TCZ (324 mg). This is the only study to report the subcutaneous route. No differences were observed between the route of administration in terms of mortality. The use of subcutaneous TCZ could therefore be considered.
We chose to use a fixed dose of 600 mg for patients under 100 kg and 800 mg for patients over 100 kg. Dose-banding studies have shown that the administration of a fixed dose for antibodies does not increase the interindividual variability of the response compared with a dose calculated according to a morphological parameter.11 The aim of dose-banding is to provide a single dose per weight interval. This helps limit costs and optimise the use of the number of vials, which is particularly important since TCZ is expensive and the quantities available are limited.
Our study shows that a smaller proportion of patients required the use of mechanical ventilation in the TCZ group, especially in patients with more extensive CT damage. Indeed, on day 14 of follow-up, two patients in the TCZ group required invasive ventilation compared with six in the control group. Yuan et al 12 showed that the severity of the CT scan was a predictor of mortality from COVID-19 infection. By comparing patients according to their degree of severity on the CT scan, we can objectify a clear improvement in the group who have received TCZ compared with the control group concerning the evolution of the ventilatory parameters. It may therefore be reasonable to think that the administration of TCZ in patients with severe disease (ie, with CT lesions >50%) would allow clinical improvement to be faster and more effective. Roumier et al 13 reported their experience with TCZ in 30 selected patients (23% in ICU). They also observed that TCZ significantly reduced the requirement for mechanical ventilation and the risk of subsequent ICU admission. This results in a shorter hospital stay and therefore a lower risk of a nosocomial event and a lower cost for society. In the same way, a French retrospective study collected data from 20 patients with severe COVID-19 compared with 25 control patients. They showed a significant difference in mortality and hospitalisation in ICU between the two groups, with 72% mortality or admission to resuscitation in the control group compared with 25% in the group treated with TCZ.14
In the same way, in each group in our study 10 patients no longer required oxygen therapy. However, there was a difference in the average oxygen flow between the two groups with an average oxygen flow rate of 4.3 L/min in the TCZ group and 6.3 L/min in the control group (95% CI −11.6 to 7.6) on day 14 (p=0.56). The need for oxygen was reduced in the TCZ group despite the fact that this group had more severe clinical and radiological impairment of COVID-19 at the beginning of the study.
In Italy, Toniati et al 15 concluded that the response to TCZ in patients with COVID-19 pneumonia and ARDS was rapid and associated with significant clinical improvement. In their study, overall at 10 days they reported improvement or stabilisation in 77% of patients, of whom 15 were discharged from hospital. The respiratory condition worsened in 23% of patients, 20% of whom died.
In our study we found a significant difference in the respiratory rate on day 14 of follow-up, with a greater decrease in the treated group. This coincides with the first report from China of 21 severe or critical patients treated with TCZ. The results showed that 15 patients had lowered their oxygen intake within 5 days after treatment with TCZ without control.1 In another study in Doha, Alattar et al 16 published a retrospective review of 25 patients with COVID-19 who received TCZ. Of the 25 patients, nine had been discharged from ICU at day 14, 13 were still in ICU and three died. At day 14 there were fewer patients on invasive ventilation. The proportion of patients in this study who were on invasive ventilation decreased from 84% at the time of initiation of TCZ therapy to 60% at day 7 and 28% at day 14.
We observed that the CRP levels were far above the normal range in all patients before the start of TCZ therapy. During the study a significant difference was seen in the CRP level. Patients in the TCZ group had lower CRP levels than those in the control group from day 7 after the injection (6.5 mg/L in the TCZ group vs 56.5 mg/L in the control group). Our results are in agreement with the study led by Xu et al,1 which reported that CRP decreased significantly and returned to normal in 84.2% of patients after treatment on the fifth day.
Cytokine levels would be interesting biomarkers. However, we did not have the possibility of dosing IL-6 at the beginning of the study. IL-6 measurement may be a biomarker for risk stratification and for effectiveness of TCZ.4
Our findings seem to support the effectiveness of TCZ in the control of cytokine storms induced by COVID-19 in patients with >50% CT lung damage. These results are in agreement with those of Xu et al.1 They report reduced lung complications, reduction of oxygen requirement, reduction of CRP levels and average hospitalisation length of stay of 13.5 days. Our results are also in accordance with the preliminary data of Fu et al 17 collected from 21 patients who received one or two doses (400 mg/dose) of TCZ for ARDS induced by SARS-CoV2. Fifteen patients experienced clinical improvement requiring less oxygen. They also observed a decrease in CRP levels.
Increased transaminase levels with TCZ are frequent, but rates of severe hepatic adverse events are low.18 Initiating TCZ treatment is associated with early increases in serum liver enzyme levels, which often rose to 1–3 times the upper limit of normal 2 weeks after each infusion, but decreased towards baseline by the time of the next 4-weekly administration. Clinical consequences have not been evident in clinical practice to date (according to drug labelling). In our study we observed an increase in cytolysis in the treated patients. The median AST rose from 54 IU/L to 1018 IU/L in 5 days in the TCZ group and from 44 IU/L to 47 IU/L in the control group (p<0.002). This difference, as well as the kinetics of appearance, allows us to attribute this side effect to TCZ and not to the virus itself. However, no clinical consequences were observed and this effect was reversible within 14 days of the injection.
We did not observe any nosocomial infections, which could be explained by the short and non-chronic use of TCZ.
Conclusion
In the beginning of this unique pandemic situation, global recommendations for COVID-19 were being made based on unpowered studies, and because of the chaotic urgency of the situation, drugs were prescribed off-label given the severity of the disease and the risk–benefit balance. Our study is observational and not a clinical trial. Hyperinflammation in COVID-19 looks like CRS, which suggests that therapies targeting IL-6 like TCZ commonly used to treat CRS can be used in the severe and inflammatory forms of COVID-19. This study presents the first conclusions regarding the use of TCZ in COVID-19. It appears to be effective in decreasing oxygen withdrawal time, respiratory failure symptoms, avoiding mechanical ventilation and stopping the biological inflammatory process of COVID-19 pneumonia in hospitalised patients, especially in those with >50% of initial lung lesions on CT scan. Randomised controlled clinical trials are needed to confirm the efficacy of TCZ in COVID-19.
Key messages
Fifteen percent of COVID-19 patients who suddenly deteriorate 7 or 8 days after the appearance of the symptoms develop acute respiratory distress syndrome.
An acute severe systemic inflammatory response known as cytokine storm leads to critical disease.
TCZ is an IL-6 receptor monoclonal antibody which seems to be a possible strategy for patients with cytokine storm.
In the context of the COVID-19 pandemic, there was an urgent need for effective treatments.
We used TCZ off-label in patients with severe COVID-19 in March and April 2020 based on its hypothetical benefit and report the experience of our general hospital.
Footnotes
EAHP Statement 5: Patient Safety and Quality Assurance.
Contributors LA and MS had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. JC, FB, GS, JP, DG-T, CM and MS carried out the medical care of the patients. LA and MS realized the data collection and performed data analysis. LA, MS and AR drafted and revised the paper. DG-T, CM and FF revised the paper. All authors approved the final draft of the manuscript for publication.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; internally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information. The data are available on request to the authors: albertini.laetitia@gmail.com; mickael.soletchnik@gmail.com.