Article Text

Abstract
Objective To assess in patients with acute respiratory failure (ARF) whether out-of-hospital (OOH) non-invasive ventilation (NIV) is feasible, safe and more effective compared with standard medical therapy (SMT).
Patients and Interventions Patients with OOH ARF were randomly assigned to receive either SMT or NIV.
Measurements and Results Fifty-one patients were enrolled, 26 of whom were randomly assigned to SMT and 25 of whom received NIV. Two patients were excluded because of protocol violations. OOH NIV was safe and effective in all patients. In the SMT group, treatment was not effective in five of 25 patients who required OOH mechanical ventilation (p=0.05). Patients in the SMT group were admitted to an intensive care unit (ICU) more frequently (n=17) (p<0.05) and for longer periods (3.7±6.4 days) (p=0.03) compared with patients in the NIV group (n=9, 1.3±2.6 days). Six patients in the SMT group required subsequent inhospital intubation and invasive ventilation during their hospital stays; only one patient in the NIV group required intubation (p=0.10). In contrast, patients in the NIV group received NIV more frequently (n=14) in hospital compared with patients in the SMT group (n=5) (p<0.01).
Conclusions OOH NIV proved to be feasible, safe and more effective for the treatment of ARF compared with SMT. OOH NIV promotes inhospital treatment with NIV and may reduce the frequency and length of ICU stays. Because the risks of OOH emergency intubation can be avoided, NIV should be the first-line treatment in OOH ARF if no contraindications are present.
- Acute cardiogenic pulmonary oedema
- acute respiratory failure
- chronic obstructive pulmonary disease
- emergency ambulance systems
- intensive care
- non-invasive ventilation
- nursing
- out-of-hospital
- pre-hospital
- respiratory
Statistics from Altmetric.com
- Acute cardiogenic pulmonary oedema
- acute respiratory failure
- chronic obstructive pulmonary disease
- emergency ambulance systems
- intensive care
- non-invasive ventilation
- nursing
- out-of-hospital
- pre-hospital
- respiratory
Although non-invasive ventilation (NIV) is frequently used in hospital for the treatment of acute respiratory failure (ARF), it is not known if NIV is effective and has benefits if applied out of hospital (OOH).
In patients with chronic obstructive pulmonary disease (COPD) with hypercapnia, inhospital NIV has proved to be beneficial because endotracheal intubation and invasive ventilation are associated with a higher incidence of ventilator-associated pneumonia and increased mortality.1–4 In hypoxic respiratory failure that is secondary to acute cardiogenic pulmonary oedema (ACPE), inhospital NIV reduces the need for intubation and results in the more rapid improvement of physiological parameters;5 6 its effect on mortality is currently controversial.7–9 NIV has also been used for patients who have ARF due to pneumonia, but this should only occur if immediate intubation can be assured.10
In the past, treatment of OOH respiratory emergencies was limited to either the application of supplemental oxygen supported by specific medications or invasive mechanical ventilation. Transport ventilators that can be used for OOH NIV are now available. As most patients with ARF are awake and cooperative, they would be eligible for therapy with continuous positive airway pressure (CPAP) or NIV.
Some studies have supported the use of OOH CPAP11–13 or non-invasive positive pressure support ventilation,14 but those studies were limited to patients with ACPE.
Although NIV can cause serious complications such as aspiration and haemodynamic effects or may be detrimental when applied inappropriately long,15 mortality may be reduced by avoiding OOH endotracheal intubation, as unrecognised oesophageal or endobronchial tube placement occurs frequently.16 This study was conducted to investigate the effectiveness and benefits of OOH NIV compared with standard medical treatment (SMT) in patients with ARF, irrespective of its origin.
Methods
Design
A single centre, prospective, randomised, intention-to-treat clinical trial, the study was approved by the ethics committee, complies with the Declaration of Helsinki and was registered at ClinicalTrials.gov (Protocol record 40/11/04).
To date there is no clinical experience published comparing the effects of NIV and SMT in OOH treatment of ARF. These first data will help to design an enlarged study powered to a primary endpoint.17
EMS system
The study was performed within the emergency medical system (EMS) of Goettingen, Germany, which is two tiered. The first tier is an ambulance staffed with paramedics. The second tier is a vehicle staffed with an emergency physician as well as a paramedic. National regulations require that both tiers must be dispatched immediately if symptoms of respiratory distress are present and that ambulance and emergency physicians will have to arrive on scene within 15 min. This implies that they arrive almost simultaneously on scene and that on-scene time is not extended by calling an emergency physician. Emergency physicians were residents of the Anaesthesiology Department of the university hospital with at least 1 year of experience in intensive care medicine and NIV.
Patient inclusion
All patients 18 years of age and older with respiratory distress caused by ACPE, COPD or pneumonia were eligible for the study if signs of hypoxic respiratory failure (peripheral oxygen saturation (SpO2) <90% while breathing room air) or ventilatory failure (SpO2 <90% and respiratory rate >20 breaths/min at rest) were present.
Patients were not enrolled if the initial SpO2 had not been documented by the paramedics and if SpO2 was 90% or greater with oxygen before the arrival of the emergency physician. Furthermore, patients were not enrolled if immediate endotracheal intubation was indicated due to respiratory arrest, breathing breaks, haemodynamic instability with blood pressure less than 70 mm Hgsyst, loss of consciousness with coma (Glasgow coma scale ≤8), or uncontrollable agitation.
Once a patient has been confirmed to meet the inclusion criteria and none of the exclusion criteria he/she was randomly assigned to receive either SMT or NIV. Randomisation was carried out by the emergency physician on scene using sequentially numbered envelopes with randomisation assignments provided in a 1:1 manner.
Treatment
Patients were positioned and intravenous access was obtained. SpO2, heart rate (HR), ECG and non-invasive blood pressure (NIBP) were monitored using a monitor/defibrillator unit (Lifepak 12; Medtronic GmbH, Meerbusch, Germany). If there was a suspicion of acute coronary syndrome, a 12-lead ECG was performed to rule out acute myocardial ischaemia.
Patients assigned to SMT received oxygen with maximum flow (12 l/min) by facemask with a reservoir for the treatment of severe hypoxaemia. NIV was applied as soon as possible. Using a transport ventilator (Oxylog 3000; Draeger Medical Luebeck, Germany), NIV was started with fractional inspired oxygen (FiO2) 1.0 and CPAP 5 mbar. CPAP was adjusted according to a flow chart. Pressure support was started as soon as CPAP had been adjusted (figure 1).

Flow chart for adjusting non-invasive ventilation parameters. BIPAP, bilevel positive airway pressure; CPAP, continuous positive airway pressure; PEEP, positive end-expiratory pressure; PS, pressure support (mbar) above PEEP (mbar) level; RR, respiratory rate.
Medication was administered intravenously at the discretion of the emergency physician: in ACPE furosemide and/or urapidil (if hypertensive crisis was the underlying cause) and in COPD reproterol and dexamethasone were given. Occasional opioids were given titrated.
Five minutes after patients had received their treatment in the presence of the emergency physician the efficiency of SMT or NIV was evaluated. If the SpO2 was not greater than 85% or has dropped to 85% or less and/or if the respiratory rate was not 30 or less or had increased to 30 breaths/min or more, treatment was classified as inefficient. If SMT failed, patients were either intubated for invasive ventilation or received rescue NIV. NIV failure would have also been recorded if a patient had shown insufficient cooperation and/or uncontrollable aerophagy.
The need for intubation was indicated by the ongoing deterioration of consciousness, breathing breaks, respiratory arrest, a decrease in heart rate below 50 beats/min, or haemodynamic instability with blood pressure less than 70 mm Hgsyst. The decision regarding intubation was made by the emergency physician.
Indications for intensive care unit (ICU) admission were the deterioration of vital parameters (fall in SpO2 ≤90% despite oxygen, increase of heart rate ≥100 beats/min) when NIV has been stopped or invasive mechanical ventilation and/or a need for catecholamine therapy (dobutamine–norepinephrine or epinephrine) for haemodynamic stabilisation.
Data collection
All vital parameters (heart rate (HR), non-invasive blood pressure (NIBP), SpO2, respiratory rate, Glasgow coma scale) were documented per the EMS protocol. In addition, these values and ventilator settings (CPAP, positive end-expiratory pressure (PEEP), pressure support, FiO2) were recorded every 5 min in the study documentation.
Samples for blood gas analysis were taken immediately and every 10 min until hospital admission via venous cannula using a heparinised syringe (Pico 50; Radiometer Medical ApS, Brønshøj, Denmark). Five millilitres of blood were discarded before sampling to avoid probe dilution. Probes were immediately analysed upon arrival at the hospital (Radiometer ABL 700 Series; Radiometer Medical ApS). The initial arterial oxygen pressure (PaO2)/FiO2 index was calculated from SpO2 breathing room air, and the final PaO2/FiO2 index was calculated from arterial blood gas analysis at admission and FiO2.
The simplified acute physiology score II (SAPS II), sequential organ failure assessment (SOFA) score, the incidence of intubation, respiratory therapy (invasive, non-invasive), 28 and 90-day mortality, the number of hospital and ICU days and complications were assessed.
The endpoint was the efficiency of the treatment method. Secondary endpoints were changes in SpO2 and respiratory rate, the frequency and length of ICU stay and the number of days spent in the hospital.
Statistics
Categorical clinical parameters between the two treatment groups were compared using Fisher's exact test. Metric parameters were compared either by the t test or the Mann–Whitney U test. The normality assumption for the t test was first checked by quantile–quantile plots.
Significance analysis of vital and blood gas parameters was performed by a two-way analysis of variance for repeated measurements, with analysis of group and time effects as well as their interaction. In the case of significant time effects, all data points in time were individually compared to time 0. Patients who were treated other than by randomisation of protocol were analysed according to the intention-to-treat principle.
The significance level was set to α=5% for all tests. Post-hoc tests were performed at the Bonferroni-corrected significance level. Analyses were carried out with the free software R (version 2.8, http://www.r-project.org).
Results
Treatment groups
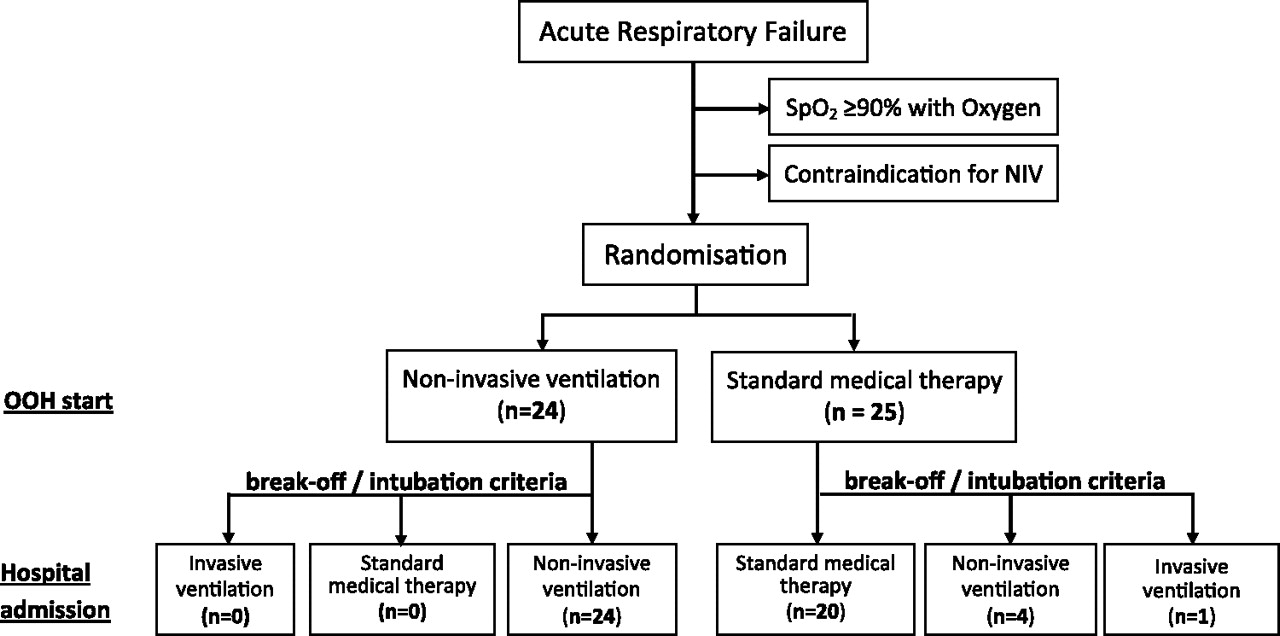
Fifty-one patients were enrolled in the study, 49 were eligible for further analysis (figure 2). One patient randomly assigned to the SMT group was excluded because OOH NIV was initiated as he was already receiving home oxygen therapy. The other patient was excluded because he was already dependent on home mechanical ventilation. Groups were comparable in terms of age, causes of ARF, severity of respiratory failure and SOFA and SAPS II scores (table 1).

Patient distribution. NIV, non-invasive ventilation; OOH, out-of-hospital; SpO2, peripheral oxygen saturation.
Baseline patient characteristics*
Effectiveness of treatment methods
According to failure rates, NIV was more effective (p=0.05) than SMT. In five of 25 patients in the SMT group, mechanical ventilation was needed OOH to prevent life-threatening hypoxaemia. One patient who lost consciousness was intubated and ventilated using intermittent positive pressure ventilation, and the other four patients received NIV (figure 2). OOH NIV proved to be effective for all patients randomly assigned to receive NIV, including for the four patients in whom SMT had failed as well as the two patients excluded from further analysis.
In the NIV group, a PEEP level of 5 mbar was used in 12 patients, PEEP was set to 10 mbar in 10 patients and PEEP was set to 15 mbar in two patients. In patients for whom NIV was used as a rescue technique, PEEP was set to 5 mbar in one patient and increased to 10 mbar in three patients.
Pressure support above PEEP was adjusted to 5 mbar in 14 patients, 10 mbar in six patients and 15 mbar in four patients. In six patients, pressure support was decreased from 5 to 0 mbar due to high tidal volumes. None of the patients required intermittent positive pressure ventilation. In the three patients in whom NIV was used as a rescue technique, pressure support was set to 5, 10 and 15 mbar.
Patients in the NIV group were treated for 4.3±8.7 h more with NIV in the hospital after admission, and no patient in the SMT group received NIV immediately after admission.
Vital parameters
Baseline vital parameters were comparable between groups (table 1). Compared with baseline values, the respiratory rate, heart rate and blood pressure were lower (p<0.01) at hospital admission in both groups, whereas SpO2 increased (p<0.01) from baseline until hospital admission in both groups (figure 3). Because there was a significant interaction between treatment and time for SpO2, the time effect was also analysed separately for the SMT and NIV groups. For both groups, the time effect remained significant (p<0.01). However, the increase in SpO2 was more rapid and stronger (p<0.01) for the NIV group than for the SMT group. In the NIV group, the SpO2 had increased to 94.3±4.4% (Δ19.6%) within 5 min and rose to 97.6±1.8% (Δ22.9%) up to the time of hospital admission. This pattern is in contrast with the SMT group, for which the SpO2 had increased to 90.8±8.1% (Δ10.1%) within 5 min and to 96.6±3.7% (Δ15.9%) up to the time of hospital admission.

Change in peripheral oxygen saturation (SpO2) in all patients stratified by time and treatment group. NIV, non-invasive ventilation; SMT, standard medical treatment.
Blood gas parameters
Venous carbon dioxide pressure (pvCO2) and pH did not differ between groups. The overall pvCO2 decrease (mean±SD) from baseline until admission was similar in both groups. In the NIV group, pvCO2 decreased from 52.7±16.8 mm Hg to 44.5±10.5 mm Hg (Δ8.2 mm Hg) compared with a change of 52.8±17.3 mm Hg to 46.1±16.5 mm Hg (Δ6.7 mm Hg) in the SMT group. Although no significant group or time effect was seen in the subgroup analysis of hypercapnic (pvCO2 >50 mm Hg) patients, the decrease of pvCO2 up to the time of admission was more pronounced in the NIV group (65.5±17.2 mm Hg to 47.8±11.2 mm Hg; Δ 17.7 mm Hg) compared with the SMT group (58.0±7.2 mm Hg to 52.6±16.9 mm Hg; Δ5.4 mm Hg). In acidotic (pH <7.35) patients, a time effect (p<0.01) was also seen, but a group effect was not detected. Furthermore, no time (p=0.12) or group (p=0.23) effect was seen for PaO2/FiO2. Nevertheless, the oxygenation index (mean) in the NIV group improved from 211.8±89.9 mm Hg to 275.3±143.9 mm Hg; no improvement (220.9±55.1 mm Hg to 219.5±69.4 mm Hg) was noted in the SMT group (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Change in oxygenation (PaO2/FiO2) index in all patients separated by treatment group. Initial: baseline values at the beginning of out-of-hospital treatment; End: values at hospital admission. NIV, non-invasive ventilation; SMT, standard medical treatment.
Clinical parameters
Although the length of hospital stay did not differ significantly between groups, SMT patients were more likely to be admitted to (p<0.05) and treated longer in (p=0.03) an ICU compared with patients in the NIV group (table 2). Eight of 17 SMT patients were treated in an ICU for further ventilator therapy compared with two of nine NIV patients. Other reasons for ICU therapy were non-ST elevation myocardial infarction (one patient each), pneumothorax (one SMT patient), pulmonary embolism (one NIV patient) or organ failure (renal failure, right or left heart failure).
Standard medical therapy versus non-invasive ventilation
Patients in the NIV group received more inhospital NIV compared with patients in the SMT group (p<0.01). Survival did not differ (table 2). One patient died of decompensated left heart failure (day one), another patient died of end-stage COPD (day 10) and a third patient died of ventilatory failure secondary to spinal muscular atrophy (day 47). In the NIV group one patient died of end-stage COPD (day 17).
Discussion
In this study OOH treatment of ARF, irrespective of its origin, was managed more effectively with NIV compared with SMT. The brief period of OOH NIV seemed to contribute to improved outcome. With NIV oxygenation improved better and SMT failed to be effective for OOH treatment of ARF in five of 25 of the patients. In four of those patients, OOH NIV proved to be a sufficient rescue strategy. In cases of hypercapnia, the decrease in pvCO2 was more pronounced with NIV. Finally, NIV proved to be safe and feasible as no complications occurred and NIV was able to be continued until hospital admission in all patients.
Our findings agree with the previously reported finding11–14 that OOH NIV is able to improve vital parameters. However, those studies were limited to patients with ACPE only. Furthermore, some studies used pure CPAP11–13 and others used NIV with PEEP and pressure support14 for treatment, despite the use of the term NIV for both treatment modalities.
SMT has a limited effect on the treatment of ARF with hypoxaemia because it is not able to reduce intrapulmonary shunt. As seen in this study, SpO2 can improve with SMT, but an improvement of the oxygenation index was not seen. Pure CPAP may help recruit alveoli and prevent cyclic alveolar collapse. However, PEEP and pressure support may be needed to increase transpulmonary pressure further and thereby reduce intrapulmonary shunt and improve oxygenation.17–21 This is supported by the findings of this study, given that the majority (85.7%) of patients in the NIV group needed a pressure support level of at least 5 mbar. Although some authors favour pure CPAP for OOH treatment of hypoxaemic respiratory failure,11–13 we believe that OOH NIV should be applied in terms of PEEP and pressure support.
Although it is important to distinguish between ACPE, pneumonia and COPD for further treatment, the assignment of patients with ARF to only one certain group, as was done in previous studies, may not reflect clinical reality. Patients with ARF may have hypoxaemia, hypercapnia or both. In this study, 13 of 22 patients with a history of COPD were both hypoxaemic and hypercapnic (pvCO2 >50 mm Hg). Of 27 patients without a history of COPD, nine patients were ‘only’ hypoxaemic, whereas 12 patients were hypercapnic and hypoxaemic.
It is difficult to identify hypercapnic respiratory failure by clinical estimation only. OOH blood gas analyses are usually not available and end-tidal carbon dioxide does not reflect arterial carbon dioxide tension in patients with intrapulmonary shunt. In hypercapnic respiratory failure, patients have rapid shallow breathing with limited efficiency for removing carbon dioxide.22 27 28 When used with pressure support, NIV allows patients to take deeper breaths with less effort and to rest their respiratory muscles.22 PEEP counterbalances the effects of dynamic hyperinflation and reduces the work of breathing at the next inspiratory effort.23 With SMT alone, a patient with rapid shallow breathing will most likely not improve. Insufficient pressure support or even CPAP alone may increase the work of breathing.23–28 Therefore, pressure support ventilation, as was applied in this study, is considered to be a first-line treatment in those patients.6
Two previous studies13 14 that applied OOH NIV also analysed patient outcomes. Plaisance et al13 found lower inhospital mortality while Weitz et al14 found no difference in mortality or the incidence of ICU treatment. In our study, mortality did not differ, but was lower than predicted. The outcome was better in the NIV group with regard to ICU treatment when compared with SMT because the patients were admitted to an ICU less often (p<0.05) and for a shorter period of time (p=0.03). We believe that there are two reasons for this improvement. NIV needs to be continued for at least 1 h before beneficial effects other than the improvement of vital parameters are seen.5 29 We agree with Plaisance et al13 that OOH NIV initiates cardiorespiratory recovery as supported by the measured variables, although the OOH treatment period is relatively short. This effect contributes to better outcome if NIV is continued immediately after hospital admission. In this study, OOH NIV seemed to promote the continuation of NIV therapy in the hospital, as inhospital NIV was applied more often (p<0.01) in the NIV group (n=14; 58%) compared with the SMT group (n=5; 20%). In addition, none of the patients in the SMT group were treated with NIV immediately after admission in contrast to patients in the NIV group, for whom NIV was continued after admission.
Limitations
While the findings in this pilot study are encouraging, they need to be replicated in a multicentre trial with a larger number of patients. Taking the data from this pilot study as basis for a larger confirmatory trial, a power of 90% could be achieved with a sample size of 46 per group.
Furthermore, all emergency physicians in this study have been familiar with NIV. The application of NIV will require at least some training for paramedics and emergency physicians who are not familiar with NIV.
Conclusions
OOH NIV is safe and feasible in the initial treatment of patients with ARF. If compared with SMT even the brief prehospital period seems to contribute to reducing the necessity of ICU treatment. NIV may be a first-line treatment in OOH ARF because no serious side effects were seen, especially if compared with OOH intubation and invasive ventilation. OOH randomised multicentre studies should be performed to substantiate the findings of this study.
Acknowledgments
The authors gratefully acknowledge the support of Draeger Medical, Luebeck, for placing the transport ventilator at their disposal for the investigation. They also wish to thank the paramedics of the fire brigade of Goettingen as well as the EMS physicians for their readiness to support the study.
References
Footnotes
Competing interests None declared.
Ethics approval This study was conducted with the approval of the ethics committee of the Georg-August-University, Goettingen.
Provenance and peer review Not commissioned; externally peer reviewed.