Article Text

Abstract
Introduction Oscillatory positive pressure devices (OPEP) can be used as adjuncts to improve sputum clearance in chronic obstructive pulmonary disease (COPD), though the evidence base is incomplete. The attitudes of physiotherapists towards these devices in the care of patients with COPD is unknown. In addition, actual use compared with the prescription of medications has not been studied.
Methods We analysed English prescribing data, obtained from OpenPrescribing.net, for a 3-year period from 2013. In addition, we conducted an online survey of members of the Association of Chartered Physiotherapists in Respiratory Care regarding awareness of devices, thresholds for treatment and device preference.
Results Out of a potential 3.2 million COPD patient-years of treatment between 2013 and 2015, 422 744 patient-years of treatment with carbocisteine, at a cost of £73 million, were prescribed, as well as 1.1 million years treatment with tiotropium. In the same period, only 4989 OPEP devices were prescribed. There were 116 responses to the survey (12% response rate), 72% in hospital practice, 28% based in the community. There were variations in respondents’ threshold for treatment with sputum adjuncts in COPD, and when asked to select either the Acapella, Flutter or positive expiratory pressure mask, preferences were 69%, 24% or 6%, respectively.
Conclusions There is a 100-fold difference between use of carbocisteine and OPEP devices in COPD, with far fewer devices prescribed than are included in the phenotypes clinicians believe them to be effective in. Variation in physiotherapist attitudes to treatment thresholds highlights the need for research into the effectiveness of OPEP devices in specific patient phenotypes.
- physiotherapy
- sputum clearance
- adjunct device
- COPD
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Sputum production is a cardinal feature of chronic obstructive pulmonary disease (COPD), though it varies between individuals,1 with many patients remaining symptomatic despite optimal medical treatment.2 Coughing to clear sputum can be tiring and uncomfortable, and patients report embarrassment coughing and disposing of sputum in public. Therapeutic approaches include smoking cessation,3 inhaled bronchodilators and corticosteroids. The active cycle of breathing technique helps patients clear sputum by ‘huffing’ rather than coughing.4 In some individuals, carbocisteine reduces sputum viscosity, making it easier to clear and reducing exacerbations.1
Handheld oscillatory positive expiratory pressure (OPEP) devices require patients to exhale against a fluctuating resistance. The positive pressure prevents airway collapse, sustaining expiratory flow. The vibration helps to mobilise sputum, making it easier to clear. A Cochrane review5 of the use of OPEP devices in COPD suggests that they can improve short-term health status and may reduce respiratory-related admissions to hospital over the longer term, as well as improving exercise capacity. However, these conclusions are based on only a few studies in small numbers of patients. Neither Global Initiative on Obstructive Lung Disease 20171 nor joint American Thoracic Society/European Respiratory Society COPD guidelines6 make any reference to sputum clearance techniques (searched using the words ‘sputum’, ‘clearance’ and ‘physiotherapy’). The joint British Thoracic Society/Association of Chartered Physiotherapist in Respiratory Care (ACPRC) recommendation is ‘consider … OPEP for patients with stable COPD who need an airway clearance technique to assist in the removal of secretions. (Grade C)’.4 ‘Need’ for an OPEP device is not defined.
We therefore analysed prescribing data for the actual usage of therapies to improve sputum clearance as well as clinicians’ attitudes to the use of OPEP devices in COPD, to help to define research questions in this area.
Methods
English prescriptions for sputum clearance treatments
English prescribing data on prescription of carbocisteine, together with that for OPEP devices for the years 2013–2015 were obtained from OpenPrescribing.net. Prescriptions for paediatric preparations of carbocisteine were excluded. We assumed that each drug item represented 1 month of treatment, multiplying item numbers by 12 to calculate treatment/years received.
Clinical attitudes to use of sputum adjunct devices
An online survey (using SurveyMonkey.com) was sent by email to members of the ACPRC. This included questions about awareness of sputum adjunct devices and likelihood of using them in patients with COPD with varying patterns of daily sputum production/tenacity and exacerbation frequency (online supplementary file 1). Options were presented in random order to avoid bias.
Supplementary file 1
Results
Prescribing data
There were 1.07 million patients with COPD on general practitioner registers in England in 2015 (via www.gpcontract.co.uk and the period 2013–2015 covers a total of 3.2 million COPD patient-years. Over this period, an estimated 422 744 patient-years of treatment with carbocisteine were prescribed (table 1) and 1.1 million years treatment with tiotropium. By contrast, only 4989 sputum adjunct devices were prescribed over the 3 years (all but seven were Flutter and Acapella). The costs for these were £73 million, £483 million and £187 000, respectively.
UK prescribing data for sputum clearance medications and devices
Survey responses
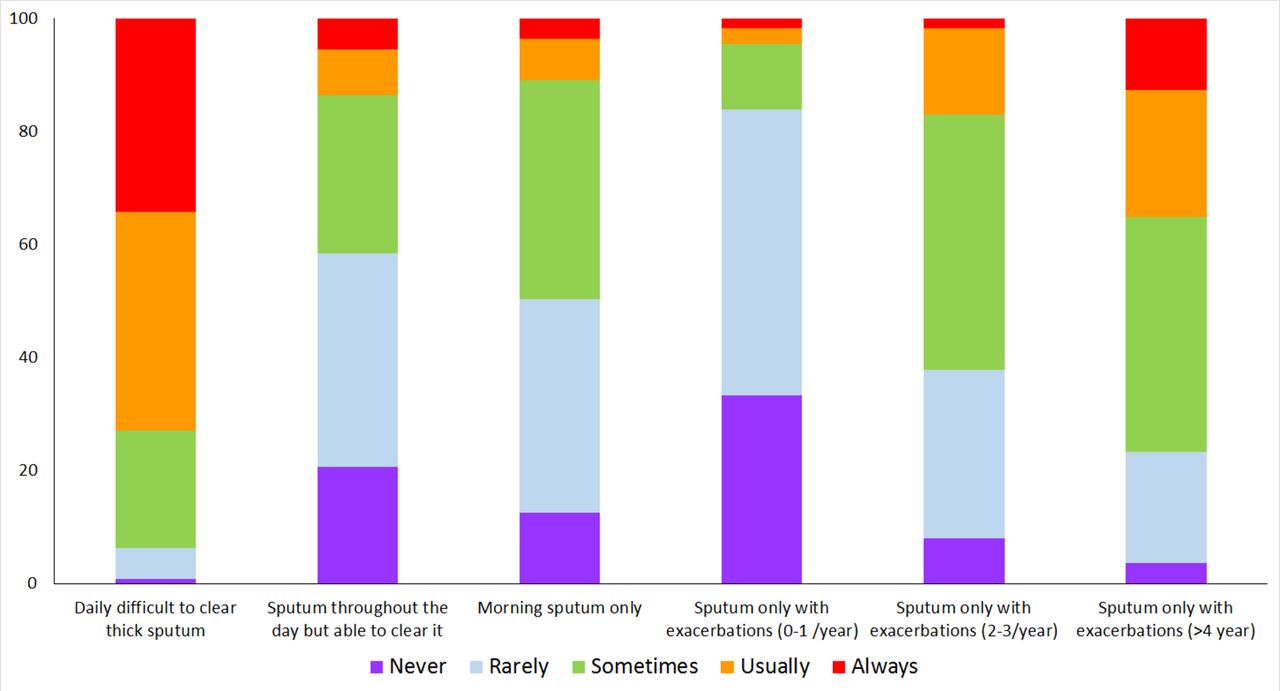
There were 116 responses (12% response rate), 72% in hospital practice, 28% based in the community (table 2). Ninety-six per cent and 95% were aware of the Acapella and Flutter, the two most commonly prescribed devices. 72.9% would usually or always advocate a device in a patient with COPD with daily, difficult to clear sputum, whereas 83.8% would rarely or never recommend one for individual-producing sputum during acute exacerbations of COPD only with 0–1 exacerbations/year (figure 1). There were significant areas of variation. 35.1% would usually or always recommend a device for individuals having >4 exacerbations per year, even if they did not produce sputum at other times. 38.7% would ‘sometimes’ recommend a device for people with morning sputum only.

{kind=link}
How often would responders recommend oscillatory positive pressure devices for sputum clearance in a patient with this chronic obstructive pulmonary disease phenotype?
Survey responses regarding the likelihood of using devices for varying clinical patterns of chronic obstructive pulmonary disease (COPD)
Asked how they would usually provide a device, 58% of respondents had devices available to give out themselves from stock, 13% were able to prescribe them, 12% advised patients to buy them, 13% did not provide them and 5% no response.
Recalling actual use in the preceding year, 21.6% had used the Acapella, 14.4% the Flutter and 1.8% the positive expiratory pressure (PEP) mask for more than five patients with COPD; 48%, 59% and 79%, respectively, replied none (table 3). Asked to choose between the Acapella, Flutter and PEP, if only one were available, preferences were 69%, 24% and 6%, respectively.
Reported frequency of use of sputum adjunct devices for patients with COPD in the preceding year
Discussion
Prescribing data reveal a striking disparity between the volume of prescription of medications for sputum clearance and use of adjunct devices; 13.2% of COPD patient-years were treated with carbocisteine, whereas the equivalent figure for sputum adjunct devices is 0.16%. Precise data on phenotypes are not available, but there is likely to be a substantial overlap between patients on carbocisteine who would benefit from OPEP devices.
The recent Royal College of Physicians COPD audit demonstrated higher use of inhaled medication compared with provision of pulmonary rehabilitation and smoking cessation,7 despite evidence that the latter are higher-value therapies.8 9 Our data raise further concern about the underutilisation of non-pharmacological therapies in COPD.
Although the 100-fold difference between use of carbocisteine and OPEP devices in COPD is likely to be broadly accurate, a number of issues limit the precision of this estimate. Some prescriptions of carbocisteine or adjunct devices will have been for bronchiectasis or other conditions. Also, we estimated each drug item as representing 1 month's treatment but they might have lasted more or less than a month depending on pattern of use. Adjunct devices were assumed to last 1 year. We are not able to capture use of devices by patients with COPD who obtained them directly from hospital or bought the devices themselves. However, the vast majority of patients are managed in primary care. As the data are based on total prescribing, we are unable to comment on what proportion of the patients taking carbocisteine had also received an OPEP device.
A Cochrane review5 of the use of airway clearance devices in COPD suggests that they can improve short-term health status and may reduce respiratory-related admissions over the longer term, as well as improving exercise capacity. However, these conclusions are based on only a few studies in small numbers of patients. A German randomised controlled trial (RCT) in 50 patients with severe COPD found that use of an OPEP device, at least three times a day for 5 min, led to significantly fewer patients (13 vs 24) needing antibiotics in comparison with controls, with fewer requiring hospital admission (5 vs 12) (OR 0.08–0.95) though the number of hospital days was the same in both arms.10 By contrast, a 1990 6-month RCT in 47 patients with a non-oscillating device did not find any impact on exacerbations.11 One study looked at exercise capacity over a longer term. In 20 patients, 3 months of OPEP was associated with an improved six minute walk distance compared with a sham device (mean difference 11 m (95% CI 66 to 156 m)).12 A 3-week OPEP device cross-over study13 in 14 sputum producers and 13 non-producers showed an improvement in St George's Respiratory Questionnaire (SGRQ), ease of bringing up sputum (PEQ score), forced vital capacity, 6MWD and a reduced 3He MRI ventilation deficit per cent in sputum producers. Another study found that short-term use of a Flutter device can reduce airways resistance even in patients with COPD with minimal sputum production.14
Thus, there are data suggesting a short-term benefit, but little information to guide long-term use or patient selection. Physiotherapists surveyed were more likely to recommend adjuncts in patients with COPD with frequent exacerbations and in those with difficult to clear sputum. However, there is significant variation in their reported thresholds for treatment, reinforcing the need for trials in specific patient phenotypes to inform clearer guidelines.
Survey respondents were self-selecting which may have introduced bias. Other sputum adjunct devices are becoming available; however, only seven of these were prescribed in 2015 so we did not include them.
Conclusion
The absence of sputum clearance devices from COPD guidelines in part reflects the dearth of long-term clinical trial data, and there are insufficient studies to recommend precise evidence-based criteria for their use. However, it is clear that far fewer devices are being prescribed than are included in the phenotypes that clinicians believe they are effective in. This suggests significant unmet need and an important disparity between actual usage and clinical consensus, highlighting the urgent need for further research regarding OPEP device usage in COPD.
Footnotes
Twitter Follow NS Hopkinson @COPDdoc
Contributors RB and NSH developed the study. AAL analysed the prescribing data. RB prepared the first draft of this paper which all authors subsequently contributed to and approved. NSH is the guarantor.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; internally peer reviewed.
Data sharing statement The data sources used for this work are publically available.