Article Text

Abstract
Study objective: To review the “protective” effects of having a higher number of siblings for the risk of atopic eczema, asthma wheezing, hay fever, and allergic sensitisation.
Method: Review of the literature (Medline since 1965 and references).
Main results: 53 different studies were identified. For eczema, 9 of 11 studies reported an inverse relation with number of siblings; for asthma and wheezing, 21 of 31 reported the inverse association; for hay fever, all 17 studies showed the effect; for allergic sensitisation or immunoglobulin E reactivity 14 of 16 studies supported the “protective” effect of a higher number of siblings. The studies emphasise a “theory” that is based exclusively on epidemiological associations.
Conclusions: Research has not yet answered the question of which causal factors explain the sibling effect. Causal factors must meet two criteria; they must vary with sibship size and they must protect against atopic manifestations. The prevailing “hygiene hypothesis” failed to explain the findings adequately. Alternative explanations include in utero programming or endocrine explanatory models. The epidemiology research into siblings and atopic disorders has entered an intellectually challenging phase. Possessing sufficient knowledge about the causal factors might prevent at least 30% of all cases of asthma, eczema, and hay fever.
- asthma
- hay fewer
- eczema
- allergy
- sibling
- wheezing
- skin prick test
- SPT, skin prick test
- IgE, immunoglobulin E
Statistics from Altmetric.com
Recent studies show that sibship size is a protective factor for allergy in both children and adults. This phenomenon, described in the literature as the “sibling effect,” was first described by Golding and Peters in a cross sectional analysis of a national cohort known as the British Birth Survey.1 The study aimed to assess health and behaviour in children in Great Britain, as well as epidemiological associations with risk factors such as household conditions, social class, smoking, etc, and attempted to contact the whole population born in one week in 1970 (n=16 567) at around their fifth birthday. Outcomes were measured by asking the mother if the child had ever had asthma, wheezing, eczema, or hay fever, and the prevalence was compared for groups with different risk factors. For asthma or wheezing, there was no association with the number of other children in the family, but for eczema and hay fever, a significant decrease in risk with an increasing number of siblings was detected. This association was later found consistently in many other studies, not only for eczema and hay fever, but also for asthma, wheezing, and sensitisation to allergens measured either by skin prick test (SPT) or by specific blood immunoglobulin E reactivity (IgE).
We consider different clinical manifestations, namely bronchial asthma, atopic eczema, hay fever, and clinical markers, that is, SPT positivity and IgE reactivity, as different expressions of the same biological pathogenesis: atopy. The term atopy describes a syndrome, which is immunologically characterised by the production of specific IgE antibodies after antigen (allergen) stimulation. To identify this process, increased IgE levels or SPT sensitisations are determined. It is assumed that after repeated allergen exposures, the syndrome becomes clinically manifest, for example, as food allergy, atopic eczema, bronchial asthma, and hay fever.2,3
Objectives are to review the literature on the sibling effect in atopic eczema, asthma, hay fever, and allergic sensitisation measured by SPT or IgE and to discuss factors that might contribute to the phenomenon.
REVIEW METHODS
The review started with a pre-existing reference library on the subject, completed with a systematic Medline search (1965–2000) for articles that reported their results on atopic disorders by number of siblings (key words: asthma, hay fever, eczema, atopic dermatitis, atopy associated with siblings, family size).
There was some ambiguity as to what the sibling effect represented. It was defined as the birth order, the number of siblings, or the family size,4 the number of older siblings,5–10 or even the number of brothers.5,11 Also, the number of younger siblings was taken into consideration (younger siblings = birth order −1). The majority of the publications provided estimates of relative risks (risk or odds ratios) for three or more siblings. Whenever feasible, we provide results showing adjusted or unadjusted risk or odds ratios for having an atopic manifestation for three or more versus no siblings. There are a few cases for which we only identify percentages or relative risk estimates for 2, or 4, or 5 and more. If only prevalences for strata with different sibling sizes were provided, the unadjusted odds ratio for three or more siblings versus no sibling was calculated, along with the corresponding 95% confidence intervals. Risk ratios and odds ratios and their 95% confidence intervals were illustrated graphically. We acknowledge that there might be some minor numerical problems comparing odds and risk ratios. The differences, however, are small because the manifestations represent rare diseases. We did not exclude any publication. However, if a study could not be included in the graphical presentations, because the outcome did not fit in one of the four categories (hay fever, asthma, eczema, or sensitisation), the effect was measured as family size, or odds ratios were not reported and could not be calculated, the results were summarised in a separate table. If one sample was used in several publications, we included results from only one article. To summarise the studies for the different manifestations, we calculated an average odds ratio weighted for the sample size.
RESULTS
A total of 53 studies dealing with atopic disorders and/or sensitisation and number of siblings were identified. The associations between atopic manifestations and siblings were summarised in figures 1 to 4 and in table 1.
Studies showing a relation between family size and atopic disease that could not be included in figures 1 to 4 (no frequencies/odds ratio reported or outcome did not fit in one of the four categories)

Eczema and number of siblings: three or more versus none. Odds ratios and 95% confidence intervals for large number of siblings (in most studies: three and more) and eczema in different studies. Odds ratios are adjusted for other risk factors, except for those marked with an asterisk. †Specialist diagnosis of atopic dermatitis, older siblings only; ‡older siblings only; §parent's report of diagnosis of atopic dermatitis, older siblings only; ¶younger siblings only.

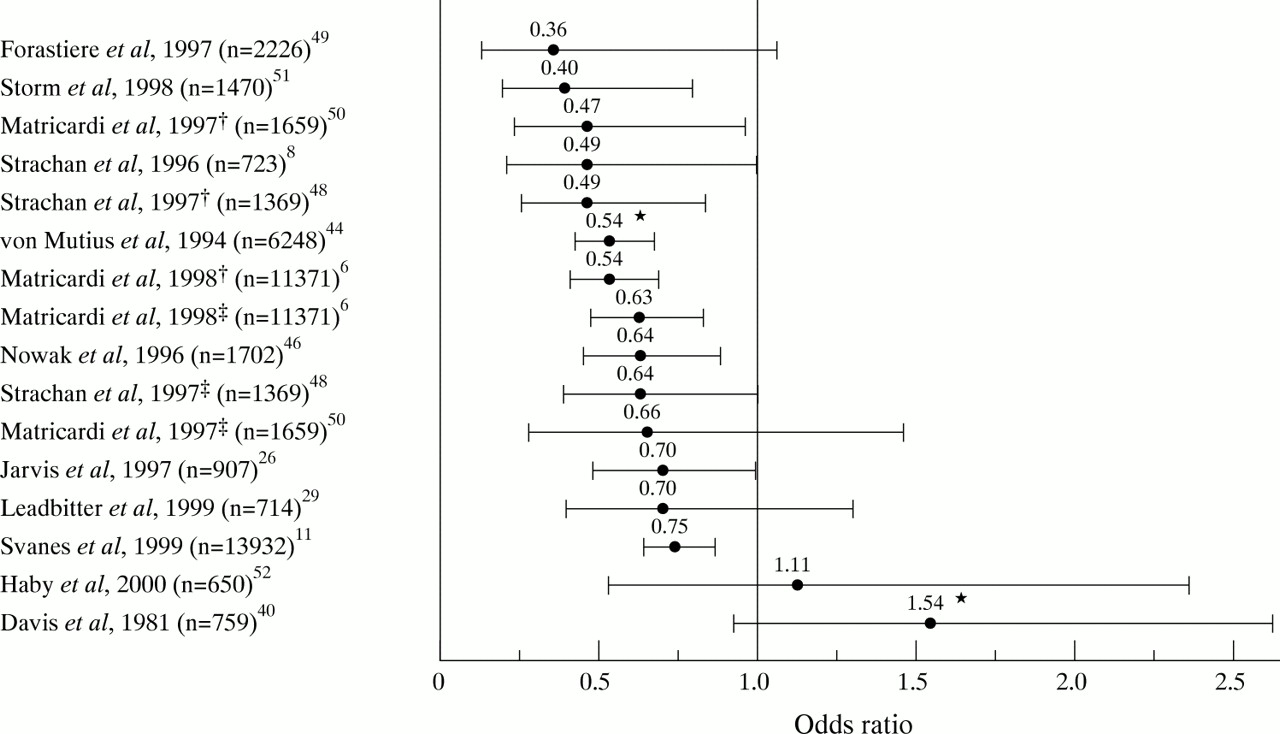
Asthma or wheezing and number of siblings: three or more versus none. Odds ratios and 95% confidence intervals for large number of siblings (in most studies: three and more) and asthma or wheezing in different studies. Odds ratios are adjusted for other risk factors, except for those marked with an asterisk. †Older siblings only; ‡1994 survey; §1986 survey; ¶all surveys; **1977 survey.

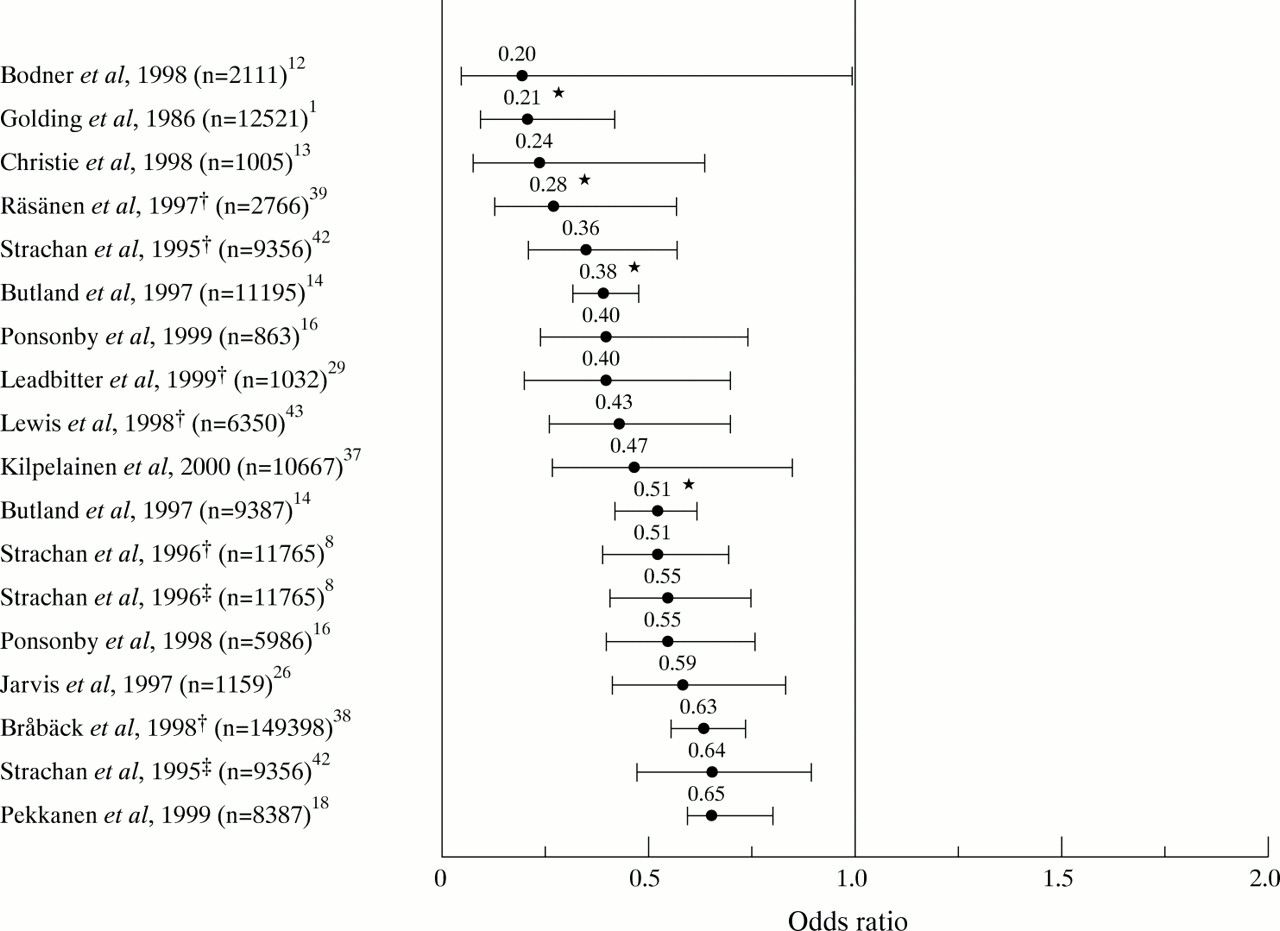
Hay fever and number of siblings: three or more versus none. Odds ratios and 95% confidence intervals for large number of siblings (in most studies: three and more) and hay fever in different studies. Odds ratios are adjusted for other risk factors, except for those marked with an asterisk. †Older siblings only; ‡younger siblings only.
SPT/IgE reactivity and number of siblings: three or more versus none. Odds ratios and 95% confidence intervals for large number of siblings (in most studies: three and more) and SPT or IgE reactivity to at least one allergen in different studies. Odds ratios are adjusted for other risk factors, except for those marked with an asterisk. †Older siblings only; ‡younger siblings only.
Eczema
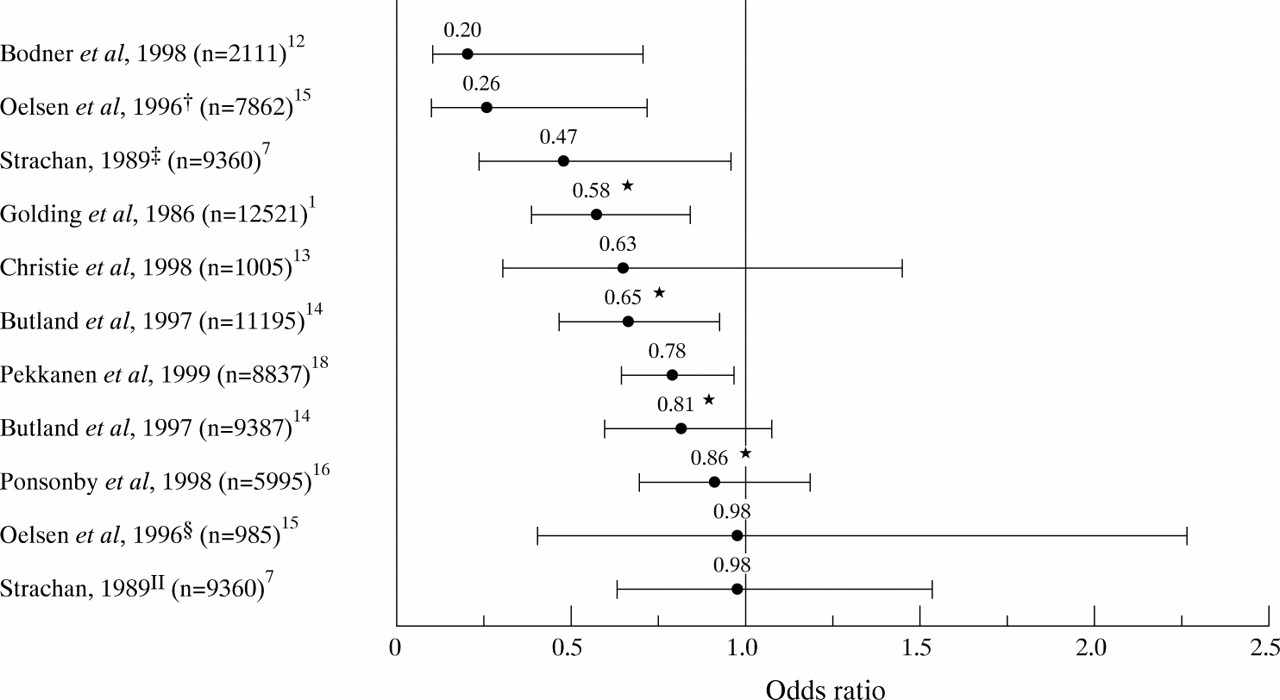
The outcomes measured were history of eczema, eczema in the first year of life, parental report of doctor's diagnosis of eczema, and specialist diagnosis of atopic dermatitis. Eleven of the reviewed studies reported results on eczema and family size (fig 1, table 1). Ten reported an inverse association with number of siblings,1,12–18 of which five were statistically significant. One found a significant inverse association for older siblings only, while for younger siblings there was no association.7 Lewis et al reported an inverse trend with an increasing number of siblings (table 1).17 Two studies reported no association between eczema and the number of siblings (table 1 and fig 1).15,19 Of the 11 studies, one is a case series that included siblings, three are cross sectional, and seven are cohort studies. The weighted average odds ratio for having eczema is 0.66 when having three or more siblings.
Asthma or wheezing
Findings were reported for the following outcomes: if the child had ever had wheezing or whistling in the chest in the past 12 months, or had ever had asthma or asthma in the past 12 months, or a doctor's diagnosis of asthma. Although the negative association between asthma or wheezing and sibling size is less consistent (fig 2), from a number of 31 studies reporting results on asthma or wheezing in relation to the number of siblings, 22 studies found a negative association, with odds ratios ranging from 0.20 to 0.84.10,13,16,18,20–24,25–37 The association reported by Wickens is based on two or more siblings.31 For Italian recruits, Attena et al reported that the firstborn child had a higher prevalence of asthma (table 1); Moyes reported the same for children in New Zealand.24,28 In 18 of the reports, the relation was statistically significant. Six studies failed to find any association to family size, including some publications that investigated an identical sample.12,17,19,23,38,39 Only one study found a positive association with having three or more siblings to asthma or wheezing.40 Weitzman et al investigated the family size, not the number of siblings, and reported a positive association with asthma and the use of asthma medication (table 1).41 Of the 31 studies, three are case-control, 21 are cross sectional, and seven are cohort studies. The average odds ratio weighted for sample size was dominated by a Swedish study of military recruits (n=148 324). Including this sample, the weighted odds ratio was 0.93, but when this study was excluded the weighted odds ratio became 0.72.
One report included results of three surveys with the same questions on respiratory symptoms repeated at three different times: 1977, 1986, and 1994.30 Each survey included schoolchildren aged 5 to 11 from the identical geographical area in the United Kingdom. Although there was a significant negative association of asthma with family size when data from all surveys are pooled, the results show that the odds ratios of asthma or wheezing by family size changed over time. In the 1977 survey, there was no association; in 1986 there was a non-significant, weak association, while in the 1994 survey the association became stronger and was statistically significant.
Hay fever
The outcomes included history of hay fever, current hay fever, hay fever in the past 12 months, and doctor's diagnosis of hay fever. The age when outcomes were measured varied between 7 and 44 years.
Of the 17 studies that reported a result on hay fever in relation to siblings, all found a significant negative relation (fig 3, table 1). The odds ratios vary between 0.20 and 0.65 for three or more siblings versus no siblings.1,8,12–19,26,29,33,37–39,42,43 Lewis et al reported associations for four children and more.17,23 Taylor et al found a prevalence ratio of 6% for the oldest and of 3.4% for children with older siblings (table 1), but did not provide the actual number of siblings.19 Some of the studies reported the results separately for older and younger siblings.8,42 In this case, the effect of older siblings was stronger than the effect of younger siblings (fig 3).
Of the 17 studies, eight had a cross sectional design, and nine a cohort design. Again, the weighted average was influenced by the large sample size of the Swedish study. Therefore, the weighted odds ratio including this study was 0.56. The odds ratio without the Swedish sample was 0.44.
SPT/IgE reactivity
In all of the reviewed studies, sensitisation was defined as a positive SPT reaction or a positive specific IgE serum antibody to any of the allergens tested. Although the definitions of positivity vary, sensitisation to specific allergens was found to be negatively associated with three or more siblings in 14 of 16 studies (fig 4, table 1).6,8,11,26,29,44–52 Of these, 10 reported statistically significant associations. Only two studies found a positive association, which was unadjusted for possible confounders.40,52 Bråbäck et al reported a significant inverse association of domestic crowding with sensitisation (table 1); Burr et al reported an insignificant negative association of number of older siblings with sensitisation.45,47
Three of the 14 studies that showed a negative relation reported their results separately for younger and older siblings. Although both younger and older siblings seemed to protect against sensitisation, in two of the three studies the association was significant only for older siblings.11,48,50 All three showed a stronger effect for older siblings. Svanes et al, however, did not identify a significant association with older or younger siblings after accounting for total number of siblings.11
Of the 16 studies, 11 were cross sectional, four were cohort studies, and one had a case-control design. The weighted average odds ratio for having SPT/IgE reactivity is 0.62 when having three or more siblings.
Table 1 shows the findings of the studies that could not be described in figures 1 to 4. Mattes et al reported an inverse association between number of older siblings and atopy in general (asthma, hay fever, eczema).9 Strachan et al found an inverse relation between number of siblings and inhalant allergy.5 Tariq et al showed a weak inverse relation of the number of siblings with atopic illness and SPT.53
DISCUSSION
From 53 studies reviewed, 48 found a negative association between number of siblings and all or some of the outcomes studied, and only three reported a positive relation. The effect is more consistent for hay fever and sensitisation than for asthma or wheezing and eczema. Most studies were from Europe, some were from New Zealand, and only a few from the US.
The studies present a variety of approaches and different types of epidemiological studies (cross sectional, case-control, and cohort). With regard to the sibling effect, different designs did not reveal different results. We focused on one common predictor, the number of siblings that has gained enormous attraction for aetiological research. The different atopic manifestations were ostensibly characterised by a common pattern of association to the number of siblings.
The pattern is more consistent for hay fever and sensitisation than for asthma or wheezing and eczema. A probable reason for the more consistent pattern is that hay fever has specific symptoms and is perhaps less likely to be misdiagnosed. Also sensitisation is measured by standard procedures and characterised by low longitudinal variability in childhood.54 Regarding asthma, variable and unspecific respiratory signs not related to asthma or atopy are frequent in children and complicate clinical diagnoses.2 Wheezing, its most important symptom, can also be associated with respiratory infections and environmental tobacco smoke exposure and is not solely a sign of atopic asthma.55 Ambiguities over the definition of asthma, especially during infancy and early childhood, thus make associations more prone to misclassification. This might explain why some studies found a sibling effect for hay fever but failed to find the same effect for asthma.13,38,39 However, in a recent study, the sibling effect on asthma was not weaker in children with transient asthma.56 Additionally, it is likely that mechanisms involved are atopic and that the weaker effect for asthma is because not all asthma cases occur through this mechanism.
The sibling effect was approached with different indicators (family size, birth order, number of siblings). Birth order equalled the number of older siblings plus one. Only a few studies did not provide estimates of the frequency of atopic manifestation for the number of siblings, and therefore could not be included in the graphical presentation (figs 1–4). The results of these studies (table 1), however, do not deviate from the ones included. Only the study of Weitzmann et al for example, focused on the family size, not the number of siblings.41 Additionally, when detailed results by number of siblings were provided, most studies indicate a dose-response relation between the number of siblings and atopy. However, we did not perform any meta-analysis, and therefore we did not analyse the overall dose-response relation.
Six of the seven analyses that investigated for different manifestations the effect of both older and younger, and that provided a relative risk estimate, showed a stronger protective effect for having older siblings.
Surprisingly, 31 of the 53 different studies did not include parental history of eczema, asthma, of hay fever, or maternal age as confounders. However, the studies that adjusted the sibling effect for maternal age and/or maternal atopy did not show different results.
A comparison by Rona et al suggested that the sibling effect for asthma attacks was stronger for more recent cohorts.30 Compared with 1977, the prevalence of asthma attacks increased from 9.5% to 13.5% in 1994 in children with three or more siblings, but from 10.4% to 17.3% in single children (fig 2).
A methodological limitation of all findings is attributable to the fact that the analyses are based on comparisons between families. Professionals and laymen claim that atopic reactions cluster in families. Thus, there is a need to analyse simultaneously within family associations, including all siblings and between family effects. If the sibling effect characterises families or lifestyles, we would expect then that “clusters” of children with atopic manifestations would occur less frequently in families with a higher number of siblings. However, if the sibling effect characterises children, we might detect an equal proportion of families with atopic children, with only the younger children being protected.
Although the magnitude and consistency of the sibling effect are remarkable, the process behind this association is largely unknown. We have to deal with findings and a “theory” that is based exclusively on epidemiological associations. If we were to identify the factors that cause the phenomenon of the sibling effect and if these factors were applied to children with a low number of siblings, then the cases in this group might be diminished by 28% for asthma (attributable proportion based on the weighted odds ratio, not including the Swedish study), 34% for eczema, 56% for hay fever, and 38% for SPT/IgE reactivity.
Several biological explanations have emerged in recent years. One major school of thought is focused on the immune maturation (protective effects or risk of infections/vaccination/hygiene, antibiotic use). Other explanations focus on in utero programming and endocrine effects (fig 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Interrelation of conflicting concepts and hypotheses that may explain the sibling effect.
On a cellular basis, the development of T lymphocyte responsiveness to allergens is a prerequisite for allergic (atopic) reactivity. The T-helper 2 cells (Th2 cells) determine the level of involvement of the mast cells and eosinophils in the host response. Through secretion of the cytokine IL4, Th2 cells regulate the synthesis of IgE antibodies, and through the cytokine IL5, they also control eosinophil differentiation and activation.57 However, if significant other cytokines, for example, interferon γ (IFNγ), which counteract the effects of IL4 are present, the reaction is assumed to be pushed toward a Th1 phenotype, which causes the secretion of IgG antibodies and the removal of the allergen.58 The Th1 phenotype is characteristic for non-atopics.
The immune maturation approach conceptualises atopic disorders as a failure of the immune deviation that should normally select for Th1 memory cells during allergen driven immune response in early life.59 It has been established that the fetal immune response is constitutively skewed away from the Th1 phenotype. This apparently represents an evolutionary adaptation designed to protect the rejection of the maternal unit. This Th2 skew seems to be maintained postnatally in atopic children.59,60
Within this framework of immune maturation, the hygiene hypothesis7 envisages that the increasing efficiency of hygiene in the (Western) developed world, coupled with lower family sizes, has reduced the contact with infections in early life (fig 5); such contact that would otherwise have promoted an immune deviation towards the Th1 pattern.44,61–63 Others named this assumption the “Westernisation” hypothesis.64–66 Within the hygiene hypothesis, different approaches specified exposures differently: history and marker infections, vaccination, antibiotic use, early day care attendance, and a childhood farm environment (fig 5). In line with these explanations are findings indicating that children with an anthroposophic lifestyle had less atopy. In this lifestyle, founded by Rudolf Steiner in the early 20th century, children are characterised by fewer mumps, measles, and rubella (MMR) vaccinations, a higher prevalence of measles history, a lower use of antibiotics, and a higher consumption of fermented vegetables that affect the intestinal flora.67
History and markers of infection
In children, measles infections seem to be protective against later development of atopy (Guinea-Bissau, allergic sensitisation: OR=0.2,68 United Kingdom, asthma: OR=0.5,12 New Zealand: 0.48,31). In a Swedish study with children from Steiner schools, no association was detected for measles, but there was a protective effect associated with no MMR vaccination.67 Also Lewis et al reported no main effects for measles infection or measles vaccination in England.43 However, the associations were evidently more complicated when taking into account the number of siblings. The authors reported that the combined effect of measles infection and/or measles vaccination in childhood and having an older sibling reduced the risk of hay fever in children.
A study from New Zealand indicated that children who received no diphtheria/pertussis/ tetanus (DPT) vaccination (n=23) had not had any reported asthma episodes, but about 23% of the other children (n=1242) had.69 This finding is supported by an English study that found an increased relative risk for atopic disease in children who received immunisation with whole cell pertussis vaccine.70 In another study from New Zealand and in a British study, however, pertussis infection was not associated significantly with wheezing or asthma in children.71,72
Tuberculin positivity at age 6 and 12 was associated with a reduction of atopic manifestations and IgE levels in Japanese children at age 12.73 The study also showed an inverse association between delayed hypersensivity to tuberculin and total IgE. Also, in African children, BCG vaccination given in infancy showed a reduced risk for positive SPT.74 A Swedish and a Norwegian study, however, did not find associations between positive tuberculin tests or BCG vaccination and the prevalence of atopy, respectively the IgE level.75,76 An aggregative study, based on a comparison of tuberculosis rates of countries in Europe, the USA, Canada, and Australia with the prevalence of wheezing in ISAAC study centres, reported an inverse relation. An increase in tuberculosis notification of 25 per 100 000 was associated with a decrease in the lifetime prevalence of wheezing of 4.7%.77
Key points
-
The sibling effect describes a phenomenon that is based exclusively on empirical findings. No comprehensive biological explanation has yet emerged.
-
For eczema, 10 of 11 studies reported an inverse association with number of siblings, 22 of 31 studies on asthma, all 17 studies on hay fever, and 14 of 16 studies on allergic sensitisation.
-
If we identify and apply the factors causing the sibling effect we could prevent at least 30% of atopic disorders.
-
The hygiene hypothesis failed to explain the findings adequately, or at least did not yet integrate essential and integrating explanations.
-
It is time to consider alternative explanations such as in utero programming or endocrine effects.
Matricardi et al found that exposure to infections, particularly to those spread by the faecal-oral route (hepatitis A and Toxoplasma gondii), were significantly less frequent in atopic cases in Italian male cadets.78 Bodner et al could not support these findings. Seropositivity for hepatitis A, Heliobacter pylori, and Toxoplasma gondii was not related to adult wheezing and atopy.35 Also, Strachan et al were unable to observe a protective effect of reported infection on the development of atopy in the first month of life.8
Antibiotic use
Antibiotic treatment in the first two years of life predicted subsequent asthma, hay fever, and eczema (OR between 2.04 and 3.19 years).70 In children with an anthroposophic lifestyle, Wickens et al found a higher risk of asthma when antibiotics were applied in infancy.71 Findings in German children also support the assumption of an increased risk of asthma in children treated with antibiotics early in life.79 In Australian children, Ponsonby et al did not find a difference in subsequent asthma or hay fever after antibiotic use.33
Day care attendance
Another specification of the hygiene hypothesis is exposure to other children in day care. Children attending day care had a higher frequency of infectious diseases.80 Krämer et al suggested that early day care attendance (6–11 months) of children from small families in Germany (up to three individuals) was protective against allergic sensitisation and hay fever in children 5–14 years of age.61 This supposition was backed by findings in Arizona, US. Attendance at day care during the first six months of life reduced the relative risk of asthma (RR=0.4.) Children with exposure to other children had more wheezing at the age of 2 years (RR=1.4), but less wheezing from the age of 6 (RR=0.8) to the age of 13 (RR=0.3). Recently, Haby et al confirmed the protective effect of early attendance at day care for the risk of allergic sensitisation in Australian children (n=650), but not for asthma, eczema, and hay fever.52 In children followed up since birth as part of the Tuscon Children's Respiratory Study, attendance at day care during the first six months of life protected against the development of asthma.34 Others were unable to observe a protective effect on the development of atopy resulting from exposure in infancy to children other than siblings. Findings by Pekkanen and coworkers in Finland (children 13–14 years of age) and by Nystad et al in Norway (children 6–16 years of age) do not support the day care hypothesis in children. Attending day care was associated with an increased risk of current symptoms of hay fever (OR=1.2 to 1.3).18,81 For children in New Zealand (7–9 years), day care attendance in the first year of life showed a non-significant increased relative risk of asthma (OR=1.81).71 In a cohort of 1369 persons born in Britain in 1958 and followed up to the age of 34–35 years, preschool nursery attendance did not protect against allergic sensitisation,48 nor did day care attendance in childhood in 13 932 adults from Europe, New Zealand, and the United States.11 Additionally, although finding a protective effect, Haby et al could not support the infection hypothesis, as infections do not explain the protective effect of day care attendance.52
Childhood farm environment
Following the infection hypothesis, studies were conducted comparing farm and urban environments. In children, farming as the parental occupation was significantly associated with lower rates of sneezing attacks, allergic sensitisation, wheezing, itchy skin rash and allergic rhinitis.82–84 Also in adults 18–24 years of age, childhood farm environment reduced the risk of allergic rhinitis.37 In other words, the old assumption that an urban environment might be a risk for atopic disease (pollution hypothesis, fig 5),85–89 was re-invented. However, the explanation changed from urban pollutants (automobile exhaust, etc) to protective factors typical for farm life. One speculation is that endotoxins from exposure to airborne bacterial products might enhance the Th1 response pattern.90 However, this conclusion also might be premature, as other studies showed that in adults, farming is associated with exposures that increase wheezing and other respiratory responses.91,92 In particular, endotoxin exposure in sawmill workers seems to contribute to respiratory problems.93
Infections as risk factors for atopy
Following an older school of thought, the bronchial susceptibility hypothesis (fig 5), respiratory infection might instigate changes that lead to asthma. In the mid-80s, a follow up study of 194 children in Massachusetts, US, suggested that respiratory illness in early life is associated with airway hyperresponsiveness as measured later in childhood.94 At the same time, a cross sectional study from Finland reported that children with infections in infancy had an increased prevalence of atopic manifestations.95 Recent studies showed that the risk of asthma was increased for children with lower respiratory tract infection, otitis media, whooping cough, mumps, and croup in the first year of life.70,96 In particular, respiratory syncytical virus infections of the lower respiratory tract were associated with an increased risk of frequent wheezing by the age of 6 (OR=4.3), but not by the age of 13 (OR=1.4). There was no association between any history of lower respiratory tract infections and the subsequent point prevalence of allergic sensitisation.97 Thus, early childhood infections are expected to trigger or induce asthmatic symptoms in non-atopic children. In this subgroup, however, children with asthma symptoms seem to have a better prognosis than children with allergic sensitisation.79 Thus, the balance of evidence does not suggest that infection, other than by the faecal-oral route, is protective. Additionally, assuming that children who have a higher number of siblings are more likely to be exposed to a mixture of infections, including respiratory infections, it is questionable whether the number of infections plays a part in the sibling effect. Furthermore, in schoolchildren both forced vital capacity and forced expiratory volume were progressively larger with an increasing number of siblings.98 This finding is difficult to explain through increased exposure to respiratory infections with increasing number of siblings, particularly as pneumonia and bronchitis in the first years of life are associated with decreased lung function in later life.99
The contradictory features of the above findings indicate that the hygiene hypothesis failed to explain the findings adequately, or at least did not yet integrate essential and integrating explanations.
The contradictory features of the above findings, or at least did not yet integrate essential and integrating explanations.
In utero and endocrine effects
The in utero programming disruption hypothesis (fig 5) is a set of explanations on atopic manifestations to which little attention so far has been drawn. There is evidence to suggest that the maternal immune system during pregnancy can enhance or inhibit the development of the feto-placental unit. Recent data support the view that some cytokines produced by both T cells and non-T cells (IL3, GM-CSF, TGFβ, IL4, IL10) favour fetal survival and growth. In contrast, other cytokines, such as IFNγ, TNFβ and TNFα, can compromise pregnancy. Cytokines favouring the maintenance of fetal survival belong mainly to the Th2 pathway, whereas the failure of pregnancy is associated with the predominance of Th1 type cytokines and/or the absence of Th2 type cytokines. This concept favours the importance of maternal immune suppression at the placental interface and the development of a Th2 response in the fetus as a consequence of maternal exposure to allergens.60
Another concept emphasises the role of hormones; progesterone and testosterone seem to promote the preferential development of Th2-like cells and induce transient IL4 production by established Th1 cells,100–102 whereas relaxin, another corpus luteum derived hormone, mainly promotes the development of Th1-like cells.103 These findings could be linked to the fact that in childhood, asthma and allergic sensitisation are more prevalent in boys.2 Strachan showed that twins have statistically significantly fewer hospital admissions for asthma, but not for other causes of respiratory diseases,104 than singletons. Studies have indicated that the endocrine conditions are different in twin pregnancies, and that this affects other health outcomes.105,106 A recent study indicated that the sibling effect is already manifested at birth. The concentration of cord blood IgE, a risk factor for subsequent atopic manifestations,107 decreased with age in children born on the Isle of Wight.108
Becklake et al reviewed the literature on gender differences and suggested that the airways in women are affected by hormonal regulation.109 Xu et al reported from a Finnish investigation that maternal age at menarche influenced the prevalence of atopic manifestations in 31 year old offspring. Adult offspring are less likely to have allergic sensitisation (ascertained by SPT) if their mother reached menarche at a later age.110 Additionally, the use of contraceptives before pregnancy increased the risk of allergic disorders among children.111
These findings suggest some influence of the in utero environment (fig 5), which is likely to change with parity, as do some of the mother's lifestyle characteristics (employment, smoking, contact with other children). Also, change in maternal lifestyle is suggested to result in variations of cord blood IgE.112
Additionally, it is possible that endocrine disruptors such as organochlorines play a part (fig 5). Firstly, the organochlorine burden seems to decrease with birth order.113,114 Secondly, placental organochlorine concentrations were related to cord blood IgE concentrations.115 And thirdly, some organochlorines seem to pose a risk for asthma and higher IgE levels.116
In conclusion, although the large body of evidence that incidence and prevalence of atopic eczema, asthma, hay fever, and allergic sensitisation are inversely related to the number of siblings, research has not yet answered the question: Which causal factors explain the sibling effect? Causal factors behind the sibling effect must meet two criteria; they must vary with sibship size and they must protect against atopic manifestations. The hygiene hypothesis might have misled research efforts. There is not sufficient covariation of infection and sibship size,52,70 and the association of markers of infections/vaccinations, and atopic manifestation is not supported by sufficient evidence. It is time to consider alternative explanations such as in utero programming or endocrine effects. The epidemiology research into siblings and atopic disorders has entered an intellectually challenging phase. The proportion of cases attributable to the sibling effect is 34% for eczema, 28% for asthma, 56% for hay fever, and 38% for developing SPT/IgE. If we possessed knowledge about the causal factors behind the sibling effect, we might prevent at least 30% of all cases of asthma, eczema, and hay fever.
Acknowledgments
The authors thank Linda Fortin for editorial support.