





Abstract
Measurement of lung function is an important component of clinical management in cystic fibrosis (CF), but has been difficult in young children. The present study aimed to characterise the utility of the forced oscillation technique for measurement of lung function in preschool-aged children with CF in a routine clinical setting.
Lung function was assessed in 56 young children (aged 2–7 yrs) with CF. Respiratory system resistance (Rrs) and reactance (Xrs) at 6, 8 and 10 Hz were measured and expressed as Z-scores. Children were classified as asymptomatic or symptomatic based on an administered respiratory questionnaire and physical examination at the time of testing. Between-test repeatability was assessed in 25 children.
Measurement of lung function using the forced oscillation technique was feasible in the CF clinic. The children with CF, as a group, had Z-scores for Rrs at 6 Hz (Rrs,6) Rrs,8, Rrs,10, Xrs at 6 Hz (Xrs,6) and Xrs,8 that were significantly different from zero. Children with current symptoms showed significantly decreased Xrs and increased Rrs,6 compared with asymptomatic children.
Measurement of lung function using the forced oscillation technique is feasible in young children with cystic fibrosis in a clinical setting. The technique has the potential to improve knowledge concerning early cystic fibrosis lung disease.
The onset of lung disease in cystic fibrosis (CF) occurs early in life, with changes in lung structure 1, 2 and function 3–6, as well as the presence of inflammation and infection 3, 5–7, in otherwise asymptomatic infants. During the preschool years, structural changes and abnormalities due to CF have been identified using high-resolution computed tomography (HRCT) 1, 8, 9. Measurement of lung function is an integral component of the clinical management of older children and adults. Spirometry is commonly used to predict pulmonary exacerbations or track responses to therapy in older children; however, alternative techniques are required for routine use in younger children.
Alterations in the respiratory function of young children with CF have been demonstrated using the interrupter technique 10–12, multiple-breath wash-out method 13–14 and impulse oscillation system (IOS) 12, 15. The forced oscillation technique (FOT) is a practical method for monitoring pulmonary function in young children that requires minimal patient cooperation 16, 17. It provides information about both respiratory system resistance (Rrs) and apparent stiffness (or reactance (Xrs)) that cannot be obtained using either the interrupter or multiple-breath wash-out techniques. The use of a FOT that employs pseudorandom noise (PRN) as a forcing signal may provide different information on respiratory dysfunction compared with the IOS, a variation of the FOT that uses an intermittent pressure impulse 18. The present study focuses on a PRN oscillatory signal and the technique is referred to as the FOT unless otherwise stated.
Studies utilising the FOT in healthy young children have demonstrated that, at frequencies of <10 Hz, measurements of Rrs and Xrs are repeatable, with a mean coefficient of variation of <10.2 and <20.5%, respectively, and an sd between two measurements over a 15-min period of <1.3 and <1.0 hPa·L−1·s, respectively 19–21. However, repeatability might be different in children with respiratory diseases, and has not yet been studied in children with CF.
The aim of the present study was to determine the utility of using the FOT for the measurement of respiratory function in a young CF population in a routine clinical setting.
METHODS
Patients
Children with CF (aged 2–7 yrs; n = 56) who underwent pulmonary function testing at the Princess Margaret Hospital for Children (Perth, Australia) as part of their clinical assessment participated in the present study. Diagnosis of CF was determined through newborn screening in 56% of patients, respiratory symptoms in 9% and failure to thrive, meconium ileus or family history in the remaining 35%. Diagnosis of CF was confirmed using the sweat test 22. Parents gave written consent for their children to participate in the study, and the study was approved by the ethics committee of the Princess Margaret Hospital for Children.
Protocol
Assessment of the children, including height and weight measurements, was performed on the day of the respiratory function tests. Children were classified as being currently symptomatic or asymptomatic at the time of consultation through a validated questionnaire administered to parents with clinician comments 23. Children were classified as currently symptomatic if a parent reported cough, sputum production or a current cold or showed signs of a lower respiratory tract infection detected by a paediatric respiratory physician. Children were classified as asymptomatic if free of respiratory symptoms and abnormal respiratory signs at the time of investigation.
Pulmonary infection data were obtained from the most recent bronchoalveolar lavage (BAL) performed as part of the routine annual assessment. Infection data were not used for 10 children as their BAL visit had been >1 yr before the FOT was performed, or the children had not undergone BAL.
Pulmonary function measurement was first attempted at the age of 2 yrs and then at every subsequent 3-monthly clinic visit in order to familiarise the children with the FOT. Once the children could produce at least three technically acceptable measurements in a single test session, measurements were recorded and retained.
Forced oscillation technique
Forced oscillatory measurements were performed according to European Respiratory Society recommendations 16, and as previously described by the authors’ group 21. Measurements of respiratory system input impedance (Zrs) were obtained using a commercially available device (I2M; Chess Medical, Ghent, Belgium) based on the research equipment prototype described by Landser et al. 17. Briefly, a loudspeaker-generated PRN forcing signal, containing integral multiple frequencies ranging 2–48 Hz, was applied at the mouth of the child via a mouthpiece containing a 0.1-μm pore-size bacterial filter (SureGard; Bird Healthcare, Melbourne, Australia). Mouth pressure and flow were recorded for 8 s per measurement at the airway opening, and Zrs spectra calculated from both the inspiratory and expiratory signals. Equipment accuracy was verified daily using known impedances, and the Zrs spectra were corrected for the impedance characteristics of the mouthpiece and bacterial filter.
The patient sat upright, wearing a nose-clip and breathing quietly through the mouthpiece. In order to minimise upper airway shunting, the patient’s cheeks and lower jaw were supported by a technician. A minimum of three and maximum of seven measurements were collected from each child. Measurements were considered technically inadequate and excluded if three or more individual frequencies showed a coherence of <0.95, leak occurred around the mouthpiece, or physical artefacts such as a cough, swallow or glottis closure were detected. Technically acceptable corrected Zrs spectra were analysed, and mean Rrs and Xrs at 6, 8 and 10 Hz recorded. The aim was to obtain within-test variability of the Rrs of <10%. However, individual measurements and the subsequent averaged Zrs data were not excluded if this criterion was not met.
In order to determine the between-test repeatability, a second set of measurements was recorded 15 min after the first set in a subgroup of children (n = 25).
Statistical analysis
Data are presented as mean±sd and were normally distributed unless otherwise stated. Differences between symptom groups were analysed using the Mann–Whitney rank-sum test. The coefficient of repeatability (1.96sd of difference between two measurements) was calculated for tests performed 15 min apart according to the methods of Bland and Altman 24, and comparison between symptom groups analysed using an independent unpaired t-test.
Baseline respiratory function (Rrs and Xrs) was expressed as Z-scores, calculated from reference values derived from a local population of 158 healthy preschool children, aged 2–7 yrs, in whom Zrs was measured using an identical FOT protocol 21. This group of healthy children had not had doctor-diagnosed or parentally reported wheeze or asthma at any time during their life and had had no acute respiratory infections within the previous 3 weeks and is described in detail elsewhere 21. Z-scores were not calculated in children with CF with a height of <92 cm as this was the lower limit in the healthy population. The test of Bartlett 25 was used to determine whether children with CF exhibited altered respiratory function compared to the healthy reference population.
RESULTS
Details of the study population are given in table 1⇓. There were no significant differences in age, height or weight between children classified as currently asymptomatic or currently symptomatic.
Patient demographics of the cystic fibrosis population
Repeatability
The between-measurement repeatability of Rrs and Xrs are shown in table 2⇓.
Between-measurement repeatability of respiratory system resistance (Rrs) and reactance (Xrs) in young chilren with cystic fibrosis
No systematic bias in between-test repeatability was observed for Rrs or Xrs (fig. 1⇓). Absolute and relative differences in lung function between tests were not dependent upon mean lung function, height or age using univariate modelling. The coefficient of repeatability between tests was <2.5 hPa·L−1·s for Rrs and <1.5 hPa·L−1·s for Xrs, equating to a difference of <3% for Rrs and <13% for Xrs (table 2⇑). Repeatability was not affected by the presence of respiratory symptoms (data not shown).

Bland–Altman plots of: a) respiratory system resistance at 6 Hz (Rrs,6); and b) respiratory system reactance at 6 Hz (Xrs,6) for two sets of mean forced oscillation measurements made 15 min apart in children with cystic fibrosis in the absence (○) or presence (•) of respiratory symptoms (–––––: mean difference; -----: limits of agreement). Δ: change.
Respiratory function
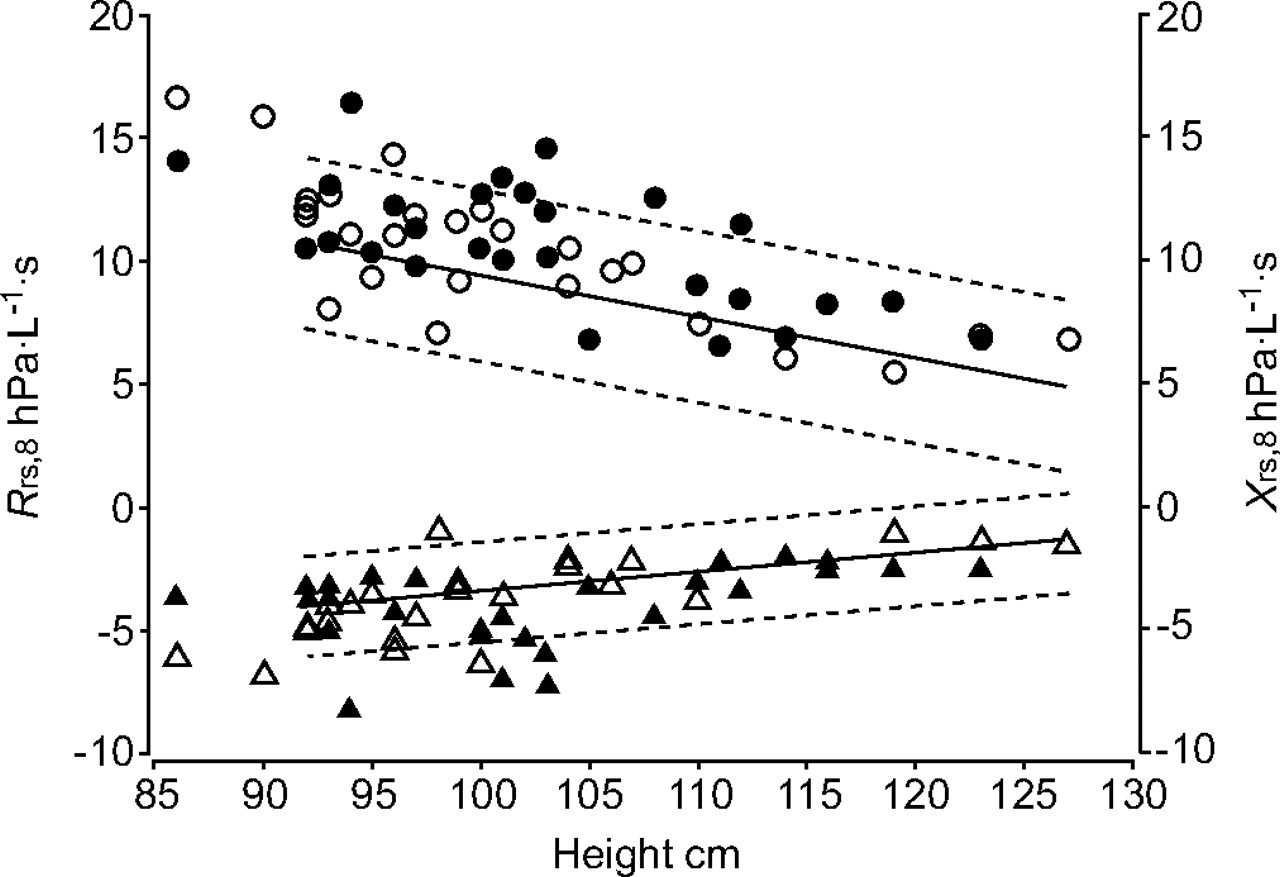
Z-scores were calculated for 53 (out of 56) children with a height of >92 cm. The distribution of respiratory function in children with CF relative to the healthy reference population is shown in figure 2⇓. Technically acceptable measurements were obtained, on average, after two or three visits. As a group, children with CF showed significantly increased Rrs compared with the healthy reference population, with Z-scores for Rrs at 6 Hz (Rrs,6; p<0.001), Rrs,8 (p<0.001) and Rrs,10 (p<0.001) that were significantly different from zero (table 3⇓). Even when children were classified as asymptomatic at the time of testing (n = 24), the Z-scores for Rrs,8 (p<0.02) and Rrs,10 (p<0.05) were significantly increased from zero.
{kind=link}
{kind=link}
Distribution of respiratory system resistance at 8 Hz (Rrs,8; ○, •) and respiratory system reactance at 8 Hz (Xrs,8; ▵, ▴) in 56 children with cystic fibrosis, when asymptomatic (○, ▵) or symptomatic (•. ▴), compared with a healthy reference population. ––––: regression line for reference population ; ------: 95% confidence interval.
Z-scores for respiratory system resistance (Rrs) and reactance (Xrs)# in children with cystic fibrosis
When compared with the healthy population, the Z-scores for Xrs in children with CF as a group were significantly different from zero for Xrs at 6 Hz (Xrs,6; p<0.001) and Xrs,8 (p = 0.01), but not for Xrs,10 (p = 0.09; table 3⇑). These differences were primarily due to the children who were symptomatic at the time of testing (table 3⇑).
DISCUSSION
In the present study, respiratory function was measured in 56 young children with CF using the FOT in a routine clinical setting, and it was demonstrated that these children showed increased Rrs and reduced Xrs compared to a healthy reference population 21. The test was easy to perform and feasible within the clinical setting. Children with current symptoms showed an increased Rrs,6 and lower Xrs (at 6–10 Hz) compared to children who were asymptomatic at the time of testing. The between-test repeatability in young children with CF was similar to that previously reported in healthy preschool-aged children 21.
Between-test repeatability
The present study characterised the repeatability of between-test measurements over a 15-min period in a young CF population, with the sd of changes for Rrs (1.07–1.25 hPa·L−1·s) and Xrs (0.67–0.74 hPa·L−1·s) lying within the ranges of short-term repeatability previously reported for Rrs (0.55–1.41 hPa·L−1·s) and Xrs (0.57–1.21 hPa·L−1·s) in healthy children 19–21, 26, 27. In the present study, between-test repeatability was not influenced by symptoms, which suggests that, in young children with CF, short-term repeatability may not be a function of disease, history or status.
Respiratory function
As a group, children with CF exhibited significantly worse lung function, with higher Rrs at 6, 8 and 10 Hz and lower Xrs at 6 and 8 Hz than a healthy reference population. However, most children with CF showed pulmonary function within the normal range, as defined by being within 2sd (±2 Z-scores) of the mean of the healthy reference population (fig. 2⇑). These data are consistent with previous reports in children with CF using the interrupter technique 10, multiple-breath wash-out method 14 and IOS 12, 15. The fact that the majority of children with CF fall into the normal range is not surprising, since, in general, these children exhibited mild disease, with <5% of children presenting to clinic with respiratory signs of wheeze, crackles or respiratory tract infection. Some children did show abnormal lung function; 13% had a Rrs,8 and 17% a Xrs,8 outside the normal range. This increased to 21% outside normal for both Rrs,8 and Xrs,8 in children with CF who were classified as symptomatic. This suggests that measurements outside the normal range may be indicative of clinically relevant disease. As measurements of pulmonary function were performed as part of the routine clinical assessment of children with CF, children were measured as they presented to the clinic. Lung function testing is used as part of the clinical assessment of children with CF.
Evidence in the literature demonstrates that lung disease begins in the periphery in young children with CF. Structural changes to the parenchyma in CF have been identified in infancy and early childhood using HRCT 1, 2, 9. Likewise, the presence of inflammation in otherwise asymptomatic individuals has been reported in young children with CF 3, 6, 7. The relationship between inflammation and tissue damping, which is reflective of respiratory tissue mechanics, has previously been shown in preschool children with CF 6.
The association between respiratory symptoms and abnormal lung function becomes more apparent in older children with CF, possibly representing the progression of lung disease with age 28. The studies in infants with CF of Brennan et al. 6 and Ranganathan et al. 4 both reported no associations with the presence or history of respiratory symptoms. Although children in this age group generally exhibit mild lung disease, and were well enough to undergo general anaesthesia in these studies, an association between a history of CF-related symptoms and worsening lung function, measured using the interrupter technique, has been reported in preschool children who were asymptomatic at the time of testing 10. However, it should be noted that the group of children with a history of CF-related symptoms was considerably smaller (n = 8) than the group of children without symptoms (n = 31), which may have affected the outcome. The present study measured the respiratory function of children with CF as part of the children’s clinical assessment during routine clinic visits. At the time of clinical assessment, the present study demonstrated that children with current symptoms showed decreased Xrs (at 6–10 Hz) and increased Rrs,6 compared to children who were asymptomatic at the time of testing. Although this association suggests potential for increasing the available clinical information, longitudinal assessments are required in order to determine the magnitude of clinically relevant changes in FOT-derived variables in individual children.
CONCLUSION
The present study shows the results of lung function measures using the forced oscillation technique in a typical clinical population of preschool children with cystic fibrosis. It was demonstrated that lung function is reduced in this group compared to a healthy reference group, and that children with cystic fibrosis with current symptoms show reduced lung function compared to children with cystic fibrosis who are asymptomatic. Measurements of lung function are an important aid to the clinical management of cystic fibrosis in older children. Further studies are required in order to characterise clinically relevant changes in forced oscillation technique variables and to determine the role of measurement of lung function using the forced oscillation technique in the clinical management of preschool children with cystic fibrosis.
Acknowledgments
The authors would like to thank the paediatric respiratory medicine clinicians and E. Balding for their assistance in completing symptom questionnaires, and T. Fukushima, K. Udomittipong, M. Verheggen, J. Oostryck and V. Starveska for their assistance in measuring lung function.
- Received January 11, 2007.
- Accepted July 19, 2007.
- © ERS Journals Ltd
References










