





Abstract
Cysteinyl leukotrienes (cystLTs) are important mediators of wheeze in atopic asthma, but the role of cystLTs in the pathogenesis of preschool viral wheeze (PVW) is unclear. Therefore, evidence for increased production of cystLTs in PVW was sought.
Urinary leukotriene E4 (uLTE4) and serum total immunoglobulin (Ig)E were measured in children (1–5 yrs) with PVW during an acute attack (n=44) and in the convalescent phase (n=19), and compared with normal controls (n=15). The effect of atopic sensitisation was assessed in a separate group of atopic controls (n=6) in whom only uLTE4 was measured.
The levels of uLTE4 were similar in normal and atopic controls and increased in acute PVW (median (interquartile range) 165 (101–285) versus 125 (82–163) ng·mM creatinine−1). Stratification by IgE showed that whereas uLTE4 was increased in 23 children with acute PVW and IgE >95th percentile (median 211 (118–312) ng·mM creatinine−1), uLTE4 was not increased in the 21 children with acute PVW and IgE ≤95th percentile. In the convalescent phase, uLTE4 fell in the subgroup with high IgE but not in the subgroup with low IgE.
It is concluded that increased cysteinyl leukotriene production during acute preschool viral wheeze is associated with high serum immunoglobulin E.
A. Oommen was funded by grant AM2/01/008 from the National Health Service National Research and Development Programme on Asthma Management. J. Grigg was funded by the Henry Smith's Charity and Medisearch.
In atopic asthma, increased production of cysteinyl leukotrienes (cystLTs) within the lung causes bronchoconstriction 1. Leukotriene E4 (LTE4) is a potent bronchoconstricting cystLT 1 and is the end product of cystLT metabolism. LTE4 is excreted in the urine and total urinary LTE4 (uLTE4) represents ∼5% of pulmonary production 2. Thus, uLTE4 can reflect disease severity in atopic asthma. For example, there is an association between uLTE4 and the degree of airflow obstruction in asthmatic children with chronic symptoms 3, and uLTE4 is increased during acute attacks of atopic asthma then falls in the convalescent phase 4. Viral colds are a common trigger for acute asthma attacks in school-age children and for attacks of wheeze in preschool children 5, 6. However, epidemiological studies suggest that most children with preschool viral wheeze (PVW) do not have atopic asthma 7. First, 60% of children with PVW will become asymptomatic by 6 yrs of age (transient wheeze), whereas wheeze will continue in only 40% (persistent wheeze) 8. Secondly, the transient pattern of wheeze is not associated with increased serum immunoglobulin (Ig)E at birth or increased atopic sensitisation at 6 yrs of age 8. It has been speculated that the different phenotypes of PVW are associated with different patterns of pulmonary inflammation 9, but to date this remains unclear.
An understanding of the pattern and timing of the pulmonary inflammation in PVW is important since it may identify subgroups that are responsive to specific therapies. In atopic asthma (where pulmonary cystLT production is increased) cystLT receptor blockade is a therapeutic option 10. By contrast, there is no consistent evidence for increased pulmonary cystLT production in acute PVW. Increased levels of LTC4 in upper respiratory tract secretions occur in infants during episodes of recurrent wheezing 11. However, Balfour-Lynn et al. 12 found no increase in uLTE4 in hospitalised infants with acute PVW. One explanation for these conflicting results is that increased upper airway cystLT production is not associated with increased production in the lower airway. Alternatively, increased pulmonary cystLT production may be limited to the subgroup of preschool children with risk factors for atopic sensitisation. Markers of increased risk for atopic sensitisation have been shown to affect the clinical severity of wheeze. For example, a high total IgE increases the risk of emergency care for rhinovirus-triggered wheeze in children 2–16 yrs of age 5. However, to date there are no data on whether increased levels of IgE influence cystLT production in PVW.
In this study, the authors sought to determine whether pulmonary cystLT production is increased in patients with PVW that was severe enough to warrant admission to hospital. To achieve this aim, uLTE4 was used as a marker for pulmonary cystLT production and IgE was measured to determine levels in the subgroup of children at increased risk for atopic sensitisation.
Methods
Patients
Children were recruited from those referred by their general practitioner to the admissions unit of the Leicester Royal Infirmary Children's Hospital (Leicester, UK) with acute PVW. The study inclusion criteria were as follows: 1) age 1–5 yrs; 2) physician-diagnosed wheeze; 3) clear symptoms of a viral cold in the 48 h preceding the wheeze attack; and 4) no wheezing in the 5 days before the clinical cold. The exclusion criteria were as follows: 1) premature birth; 2) a clinical diagnosis of bacterial infection; 3) any other chronic respiratory pathology; and 4) oral corticosteroid therapy prior to admission. On admission, each child received a single dose of oral prednisolone and “as required” nebulised salbutamol. The presence of wheeze was confirmed by a clinician, a clinical history was obtained from the parents and clinical evidence of a viral cold (i.e. rhinitis) was sought. A urine sample was then collected for uLTE4 analysis within 36 h of admission and a blood sample obtained for IgE. After discharge, some children were visited at home within 6 weeks. If there had been no respiratory symptoms in the preceding 7 days, a “convalescent” urine sample was obtained.
Two separate control groups were recruited. First, “normal controls” from a random selection of children attending hospital for an elective ear, nose and throat or ophthalmic surgery. In these, a urine sample for uLTE4 was obtained prior to surgery and a blood sample for IgE obtained immediately after induction of anaesthesia. Secondly, “atopic controls” from children with suspected food sensitivity who attended for a food challenge. These children had a history of a suspected allergic reaction to a food and at least one positive skin-prick test to food antigens. The atopic controls did not have a blood sample for IgE for ethical reasons. Controls were excluded if there was a history of either chronic respiratory disease, a previous attack of wheezing, active eczema or symptoms of a respiratory tract infection in the preceding week. The study required written parental consent and was approved by the Leicestershire Research Ethics Committee.
Sample collection and analysis
Urine samples were obtained using a bag or sterile potty. Urinary infection was excluded using the Multistix 10SG dipstick (Bayer, Newbury, UK) screening test. Urine samples were initially stored in a refrigerator, then transferred to storage at −70°C within 12 h. The uLTE4 concentration was measured in unprocessed samples by enzyme-linked immunosorbent assay kit (ACETM LTE4 ELISA kit; Cayman Chemicals, Michigan, USA), which has been previously validated against uLTE4 concentrations measured after high-performance liquid chromatography extraction 13. Briefly, urine was defrosted at room temperature and 500 µL was used in the ELISA without further processing. The assay detection limit was 25 pg LTE4·mL−1. Urinary creatinine was measured using the Dade Behring Dimension Analyser (Dade Behring, Deerfield, IL, USA) and uLTE4 levels were expressed as ng·mM creatinine−1. Serum for IgE was obtained from a venous blood sample that had clotted for 60 min at room temperature. Serum was separated by centrifugation and stored at −20°C. IgE was measured using the UniCAP Analyser machine (Pharmacia, Stockholm, Sweden) and expressed as kU·L−1.
Statistics
Data are summarised as median and interquartile range (IQR) unless specified and comparisons were performed using the Mann-Whitney U‐test and the Chi-squared test. Correlations were determined by Spearman rank correlation (rs). Paired data were analysed using the paired t‐test. p‐Values of <0.05 were considered statistically significant.
Results
A total of 44 children (32 males, 12 females) with acute PVW, 15 normal controls (nine males, six females) and six atopic controls (three males, three females) were studied. Children with PVW were slightly younger than normal controls (age 3.0 yrs (1.8–3.6) versus 4.5 yrs (3.4–5.5), p<0.01) and had higher IgE (118 kU·L−1 (23–293) versus 15 kU·L−1 (7–26), p<0.01). The median duration between a viral cold and onset of wheezing was 24 h (12–48). In eight children this was their first attack of PVW. Twenty six children with acute PVW had a history of wheezing exclusively with colds (previous attacks of PVW n=4 (2–6)) and 10 had a history of additional interval respiratory symptoms, including moderate nocturnal cough and wheeze after playing (previous PVW attacks n=7 (4–13)). In 19 children with acute PVW a convalescent urine sample was obtained.
Serum IgE of normal controls were within the 95th percentile reported for nonatopic children 14 and there was no difference in uLTE4 between the normal controls and the atopic controls (fig. 1⇓). Data from the PVW group were therefore compared with the normal controls only. When considered as a single group, children with acute PVW had higher uLTE4 compared to normal controls (165 (101–285) versus 125 (82–163) ng·mM creatinine−1, p<0.05, fig. 1⇓). The uLTE4 level of the whole group fell during the convalescent phase, to lie within the range of the normal controls (mean fall (95% confidence interval (CI)) 70 (28–112) ng·mM−1 creatinine, p<0.05, n=19 (fig. 2⇓)).

Dot plot of urinary leukotriene E4 (uLTE4) concentrations corrected for creatinine in preschool children with acute viral wheeze (n=44), normal controls (n=15) and atopic controls (n=6). Horizontal bars represent medians. LTE4 levels are significantly higher in the acute preschool viral wheeze group. *: p<0.05 versus normal and versus atopic controls.

Paired change in urinary leukotriene E4 (uLTE4) between the acute and convalescent phase of preschool viral wheeze. The fall in uLTE4 is significant. *: p<0.05, n=19, paired t‐test.
There was a moderate correlation between uLTE4 and IgE during acute PVW (rs=0.35, p<0.05). Stratification based on the 95th percentile for IgE 14 resulted in different patterns of uLTE4. The subgroup with high IgE (n=23) had elevated uLTE4 during the acute phase (p<0.05 versus normal controls, table 1⇓). The individual data plot (fig. 3⇓) shows that the effect of IgE on acute uLTE4 is apparent in children with the highest levels (>250 kU·L−1). On convalescence, uLTE4 fell in the high IgE subgroup (p<0.01 versus acute, n=14, table 1⇓), to become no different from normal controls. In contrast, uLTE4 in children with PVW and low IgE (n=21) was not elevated during the acute phase (versus normal controls) and did not change on convalescence (n=5, table 1⇓).

Urinary leukotriene E4 (uLTE4) of children with acute preschool viral wheeze categorised by serum total immunoglobulin (Ig)E. Horizontal bars represent medians. *: p<0.05, Mann-Whitney U‐test.
Comparison between children with preschool viral wheeze (PVW) after stratification for serum total immunoglobulin (Ig)E during an acute attack
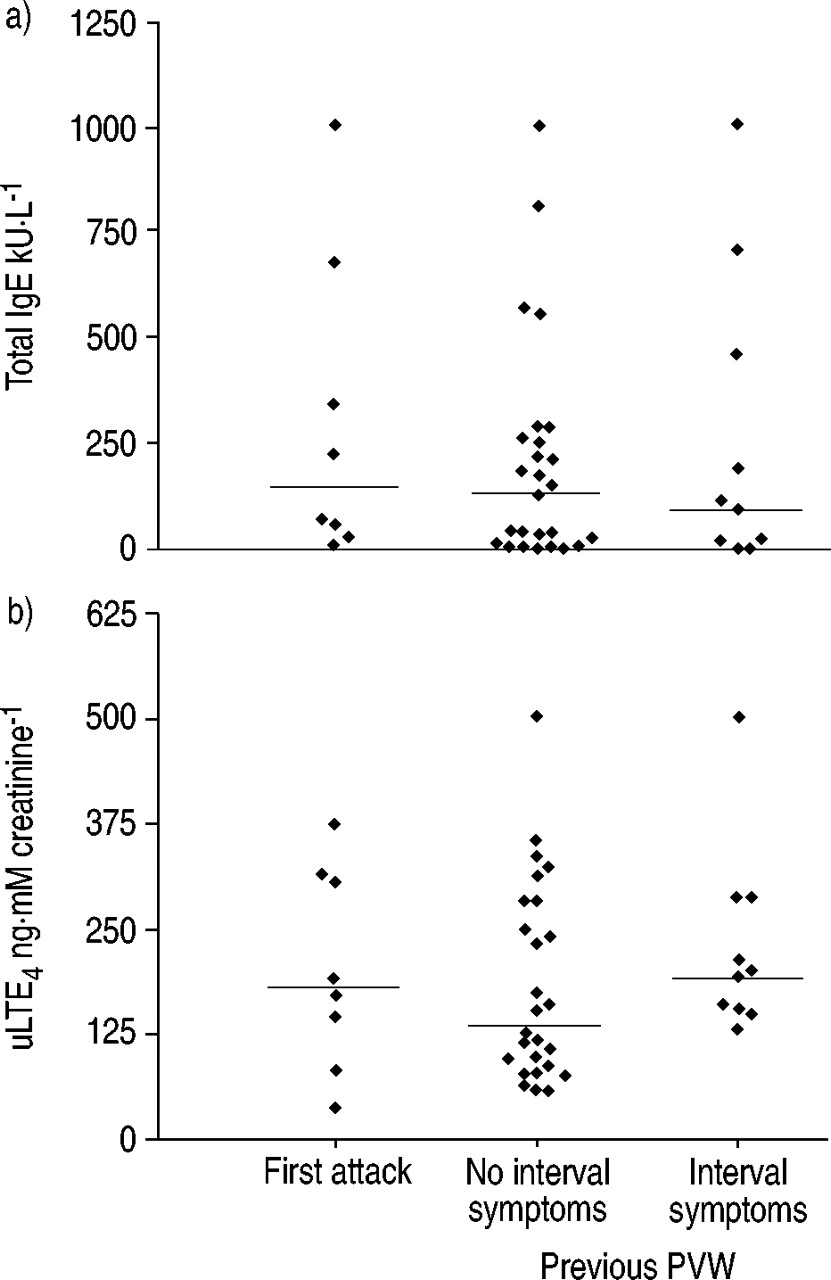
Clinical parameters in children with acute PVW were similar in the high and low IgE groups (table 1⇑). In acute PVW there was no difference in IgE or uLTE4, when categorised by previous episodes of exclusive PVW (i.e. no interval symptoms) or history of PVW and interval symptoms (fig. 4⇓). There was no correlation between uLTE4 and the time period between administration of oral steroids and urine sampling (fig. 5⇓). uLTE4 in the six children with acute PVW in whom urine was obtained before steroid therapy, was not increased compared with those (n=38) who were studied after steroid administration (fig. 5⇓).
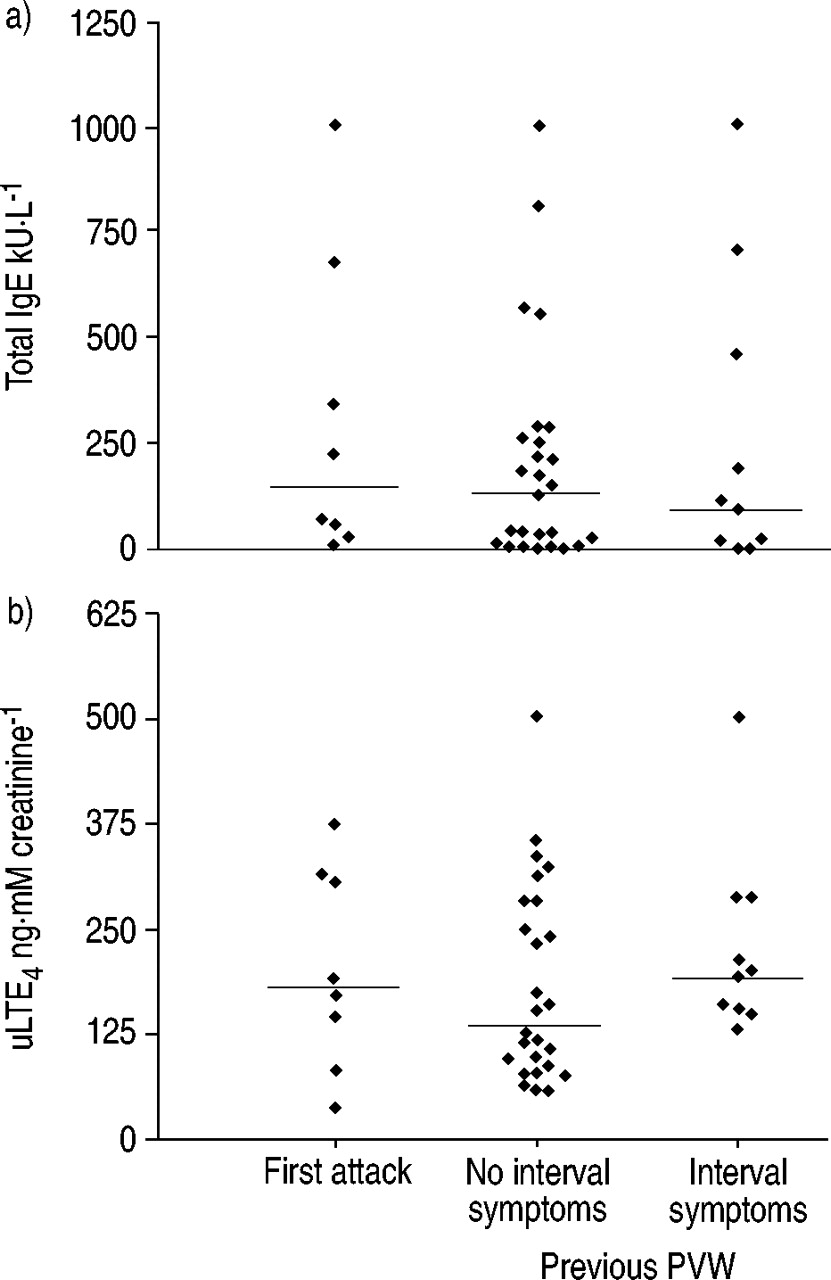
Serum a) total immunoglobulin (Ig)E and b) urinary leukotriene E4 (uLTE4) in acute preschool viral wheeze (PVW). Children were categorised as either having a first attack (no previous symptoms), no interval symptoms (previous exclusive PVW) or interval symptoms (previous PVW with interval symptoms).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Scatter plot of the correlation between urinary leukotriene E4 (uLTE4) and the duration between steroid administration and urine sampling in acute preschool viral wheeze. The zero time point represents children sampled before oral steroid therapy. There is no correlation between the two variables by Spearman rank correlation.
Discussion
The data from this study show that children admitted to hospital with acute PVW have elevated uLTE4, which falls into the normal range with resolution of symptoms. However, not all symptomatic children have increased cystLT production, since uLTE4 in the acute phase of PVW is not elevated in the subgroup with low serum IgE. In these children, perhaps similar to those studied by Balfour-Lynn et al. 12, no evidence was found that cystLTs contribute to symptoms. Increased uLTE4 was found in the whole PVW group in the present study because children were skewed towards an increased IgE. The current authors therefore speculate that differences in the published data may be due to differences in serum IgE in the children studied 11, 12.
How could high IgE predispose to increased cystLT production during acute PVW? It is unlikely that high serum IgE or atopic sensitisation per se increases uLTE4 since: 1) there was no association between IgE and uLTE4 in the normal controls; 2) increased uLTE4 did not persist in children with high IgE when asymptomatic; and 3) uLTE4 was not increased in the atopic control group. This suggests that either high IgE or a mechanism that acutely increases IgE during PVW or a variable associated with elevated IgE (such as atopic sensitisation) primes the lower respiratory tract to increase cystLT production during PVW. Since skin-prick tests were not performed in children with PVW, the atopic status of the high IgE subgroup is unknown and an interaction between atopic sensitisation (rather than total IgE) and viral colds has not been excluded.
Is the inflammatory pattern of children with acute PVW and high IgE similar to a viral-triggered attack of atopic asthma? To date, there are no data comparing inflammation between acute nonviral attacks and viral-triggered attacks of atopic asthma. However, the pattern of uLTE4 in acute PVW with high IgE has similarities to that reported during acute atopic asthma in older children 4. Like atopic asthma, uLTE4 in acute PVW with high IgE is elevated in the acute phase and falls on convalescence. In contrast to atopic asthma, uLTE4 in acute PVW falls into the normal range on convalescence 4. The data presented here suggest that increased pulmonary cystLT production during acute PVW rapidly returns to normal when symptoms resolve, a finding similar to that of Stevenson et al. 15, who found persistent airway inflammation in asymptomatic children with “intermittent” atopic asthma, but not in children with a history of “exclusive” viral-triggered wheeze.
No clinical parameters were found that distinguished children with PVW who had either increased IgE or increased uLTE4. In particular, a history of both PVW and interval symptoms was not associated with increased uLTE4. Castro-Rodriguez et al. 16 have reported a clinical index that calculates risk of developing asthma in young children with recurrent wheezing. Preschool children with one “major” risk factor (parental history of asthma or eczema) or two of three “minor” risk factors (blood eosinophilia, wheezing without colds and allergic rhinitis) are 9.8 times more likely to be diagnosed as active asthmatics at 6–13 yrs 16. It remains to be determined whether this index better defines the subgroup of PVW with elevated uLTE4.
There are two potential confounding variables. First, steroids attenuate cystLT release from the asthmatic lung 17 and most children had received a single dose of oral steroids prior to urine sampling. If children with low IgE were exquisitely sensitive to steroids, it is possible that cystLT levels had been normalised prior to sampling. If this were the case, children with low IgE who were sampled before, or just after, oral steroids should have had elevated uLTE4. However, no association was found between uLTE4 and the duration of the sampling from oral steroids, for both the low IgE subgroup (data not shown) and for the whole group (fig. 5⇑). Furthermore, uLTE4 was not different from normal controls in four children with low IgE who were studied before oral steroid therapy (data not shown). A major confounding effect of oral steroids is therefore unlikely. The second limitation is the effect of a viral cold per se on uLTE4. The current authors did not measure uLTE4 in normal children with viral colds for two reasons. First, it was ethically unacceptable to obtain blood for IgE in conscious normal children. Secondly, serendipitous blood sampling during anaesthesia was not possible during colds, since surgery was postponed. Since no increase in uLTE4 was found in acute PVW with low IgE, an effect of colds per se on uLTE4 is unlikely in this subgroup. Increased uLTE4 caused by colds per se in the high IgE group cannot be excluded and remains a significant study limitation. Future studies of uLTE4 in normal children with high IgE are required during viral colds, to assess the clinical relevance of an increased uLTE4 seen in the present study. However, a recent study has demonstrated that leukotriene receptor blocker therapy improves persistent wheeze in preschool children 18, a finding compatible with a clinically relevant role for cystLTs in this age group.
In conclusion, heterogeneity in urinary leukotriene E4 excretion in acute preschool viral wheeze was found. Elevated urinary leukotriene E4 occurred in children with the highest serum immunoglobulin E, but whether increased levels are due to viral colds per se or the consequence of inflammation causing wheeze remains unclear. The authors speculate that increased cysteinyl leukotriene production during preschool viral wheeze is clinically relevant, and immunoglobulin E or urinary leukotriene E4, or both, should be measured in trials of cysteinyl leukotriene receptor blocker therapy to prevent a potential subgroup of responders being overlooked.
Acknowledgments
The authors would like to thank R. Tomiak of MSD (UK) for a grant to purchase the leukotriene E4 kits. They would also like to thank K. Peck and T. McNally for collecting the urine specimens.
- Received March 15, 2002.
- Accepted August 2, 2002.
- © ERS Journals Ltd
References









