





Abstract
Reticular basement membrane (RBM) thickening in asthma is considered to be the result of subepithelial fibrosis. Thus, the RBM in asthma should contain an excess of fibrils identified as interstitial collagen and the ratio of fibril to matrix should be increased above normal levels.
Electron micrographs of the RBM were compared with those of interstitial collagen deeper in the bronchial wall using endobronchial biopsy specimens from adult asthmatics (aged 18–41 yrs (n = 10)), children with difficult asthma (aged 6–16 yrs (n = 10)), wheezy infants with reversible airflow limitation (aged 0.3–2 yrs (n = 10)) and age-matched nonasthmatic controls: 10 adults, nine children and nine symptomatic infants with normal lung function.
Fibrils in the RBM were significantly thinner (median (range) width 39 (30–52) nm versus 59 (48–73) nm), and fewer fibrils were banded than in the interstitial collagen (ratio of banded to non-banded fibrils 0.08 (0–0.17) versus 0.22 (0–1.3)). The ratio of fibrils to matrix in the thickened RBM of asthmatics did not differ from that of their respective controls (1.34 (0.63–2.49) versus 1.18 (0.31–2.6)).
The ratio of fibril to matrix in the thickened reticular basement membrane of asthmatics is normal, and, contrary to what is expected in fibrosis, the fibrils do not resemble those of interstitial collagen.
- Asthma
- reticular basement membrane
- subepithelial fibrosis
- transmission electron microscopy
- ultrastructure
Morphologically, the subepithelial basement membrane in human airways is composed of a basal lamina (sometimes referred to as the true basement membrane), to which the epithelium is attached. Extending externally from the basal lamina is a lamina reticularis (henceforth referred to as the reticular basement membrane (RBM)). Immunohistochemistry demonstrates that type IV collagen is a major component of the basal lamina 1. However, without immunostaining, the basal lamina can be visualised only by electron microscopy, since its width (∼80 nm) is below the resolution of the light microscope. By contrast, the RBM is considerably thicker (∼4 μm in healthy adults) and can be seen using light microscopy. The RBM is characteristic of normal humans and other primates, such as monkeys 2. Histological sections stained with haematoxylin and eosin demonstrate that the RBM is present in all normal healthy individuals, but also that it is homogenously thickened and hyaline in appearance in asthma 3, 4.
The abnormal thickening of the RBM begins early in asthma, as early as 4 yrs of age, and is already maximally thickened in children aged 6–16 yrs with severe asthma 5–7.
As immunohistochemistry demonstrates the presence of epitopes for collagen subtypes I, III and V in the RBM, the abnormal thickening of this layer in asthma has been thought to result from a fibrotic process sometimes described as subepithelial fibrosis 8. However, these epitopes are part of a morphologically heterogeneous family of glycoproteins that includes both amorphous and fibrillar forms, collectively termed collagen. Fibrosis, as seen in fibrotic lung diseases, is defined on the basis of the accumulation of abnormal amounts of interstitial collagen, or scar tissue. Although the process of interstitial pulmonary fibrosis (IPF), in the lung parenchyma, is considered irreversible, thickening of the epithelial RBM in asthma can be reversed, at least partially, following anti-inflammatory treatment 9 or removal of the asthmatic from an occupational cause 10. To date, there has been no objective quantitative examination of this key aspect of remodelling in asthma.
Interstitial collagen, and that associated with pulmonary fibrosis, is composed of fibrils of defined width, each with an ultrastructurally characteristic pattern of periodic banding 11. These criteria were used to test the hypothesis that RBM thickening in asthma, in adults and children, is the result of fibrosis and would, therefore, exhibit an increased ratio of fibril to matrix, in which the fibrils would have the ultrastructural characteristics of interstitial collagen. The aim of the present study was to compare the ultrastructural appearance and width of RBM fibrils to those of interstitial collagen deeper in the bronchial wall. The ultrastructural features and ratio of fibrils to matrix were compared with age-matched controls for adult and paediatric asthmatics and wheezy infants with reversible airflow obstruction. In order to confirm the proposition that interstitial collagen in the bronchial wall and collagen in IPF have a similar ultrastructure, fibril width and banding were also investigated in lung biopsy specimens from five adult cases with cryptogenic fibrosing alveolitis (CFA).
METHODS
Subjects
Adults
Ten nonsmoking adults (median (range) age 27 (18–41) yrs) with mild steroid-naive asthma were compared with 10 healthy nonsmoking nonatopic controls (age 33 (21–42) yrs). Details of these patients have been provided previously 3, and are summarised in table 1⇓. Collagen ultrastructure in open lung biopsy specimens from five adults with histologically diagnosed CFA was also assessed; the clinical details are summarised in table 2⇓.
Clinical details of adults, children and infants with and without asthma
Clinical details of patients with cryptogenic fibrosing alveolitis
Children
Ten children (age 10 (6–16) yrs) with difficult asthma were compared with nine nonasthmatic paediatric controls (age 11 (7–16) yrs) undergoing bronchoscopy for other respiratory indications, as previously described 5. Difficult asthma was defined as persistent symptoms requiring rescue bronchodilator therapy on >3 days·week-1 despite >1,600 μg·day-1 inhaled budesonide (or equivalent) and long-acting β2-agonists and/or regular oral steroids.
Infants
Asthmatic infants were as previously described 12. Asthma in this group was defined as persistent symptoms of wheeze and/or cough and reduced airways conductance with bronchodilator reversibility. Lung function was measured by whole-body plethysmography. The infant controls were also symptomatic, but exhibited normal lung function. Ten asthmatic infants (age 12 (4–24) months) and nine control infants (age 11.5 (3–24) months) were included.
Bronchoscopy and endobronchial biopsy specimens
Flexible bronchoscopy was performed in the adults and children, and endobronchial biopsy specimens were taken from the subcarinae of the right lower lobe. Details of the procedures have been described previously for both children 5 and adults 3. Rigid bronchoscopy was performed in the infants under general anaesthetic as previously described 12. Informed consent was obtained from the adults and the parents of the infants and children to use the biopsy specimens for research purposes.
Biopsy specimen processing
Biopsy specimens were fixed in 2.5% glutaraldehyde in 0.05 M sodium cacodylate buffer (pH 7.4), post-fixed in 1% osmium tetroxide (in the same buffer), and dehydrated and embedded in epoxy resin (Araldite®). Plastic sections (1-μm thick) were stained with alkaline toluidine blue. An area of the section that contained epithelium, RBM and subepithelium was selected. Ultra-thin sections (70 nm) were cut, placed on high-transmission 200-mesh thin-bar copper grids and stained with uranyl acetate and lead citrate. Micrographs were obtained using a Hitachi H7000 (Hitachi, Nissei Sanyo, Tokyo, Japan) transmission electron microscope.
Quantification
From each ultra-thin section, two micrographs were taken of areas of RBM immediately below the basal lamina and two were taken at random from subepithelial areas deep below the RBM and at least 100 μm deeper than the basal lamina, the latter representing areas of interstitial collagen. Each micrograph was taken at a magnification of ×15,000. Micrographs were coded and assessed by a single observer who was blind to patient details and the area of the biopsy that had been photographed. The technique of point-counting morphometry was used to assess fibril banding and the ratio of fibril to matrix. A sampling grid of points, arranged 1 mm apart in a triangular array, was used 13. The hexagonal area associated with each point represented ∼0.75 μm2. Four randomly selected fields with ≥200 points per field were counted on each micrograph 14. Assessment was made of whether each point was positioned on a fibril or matrix. Furthermore, if the point was on a fibril, an assessment of whether the fibril appeared banded or not at any position along its length was made (fig. 1⇓). Points positioned on the border of fibril and matrix were counted separately, and were divided equally between fibril and matrix counts in the final analysis. In order to assess collagen fibril diameter, four fields each of an area representative of RBM and interstitial collagen were photographed for each patient (magnification ×45,000). All micrographs were developed in a similar manner in order to ensure that the contrast remained similar. Five collagen fibrils per field were selected randomly and the width of each fibril was measured using Image Pro 4 software with a threshold autotracer (Media Cybernetics, Inc., Silver Spring, MD, USA). Twenty fibrils were measured in areas representing RBM and interstitial collagen, and the results expressed as a mean.
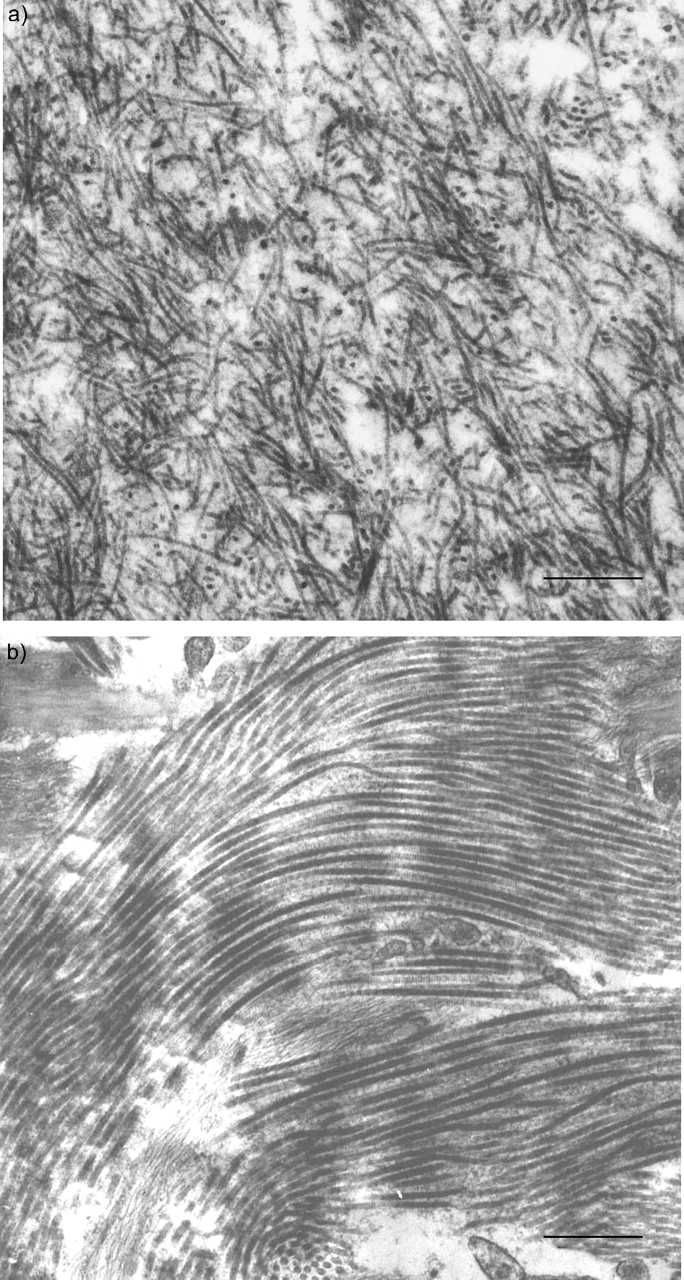
Electron micrographs showing the ultrastructural appearance of the bronchial: a) reticular basement membrane (RBM); and b) deeper interstitial collagen. The collagen fibrils are more obviously banded and thicker than the RBM fibrils. Scale bar = 500 nm.
In the CFA patients, collagenous areas of lung parenchyma with preserved alveolar architecture were selected and electron micrographs and measurements were made using the methods described previously.
Statistical analyses
The ratio of banded to nonbanded fibrils was calculated for the RBM and interstitial collagen, and the ratio of fibrils to matrix was calculated for the RBM in each age group. Nonparametric tests were applied to test for inter-group differences. Comparison between all groups was made using the Kruskal–Wallis test, followed by a Mann–Whitney U-test if a significant difference (p<0.05) was found. The Bonferroni correction was introduced for multiple comparisons. Variability of counts was calculated using the percentage coefficient of variation.
Variability
The intra-observer error of repeat measurement of performing three separate counts of fibril banding on the same micrograph on different occasions was <5%. Intra-section variability, assessed by taking up to six micrographs from a region and calculating the cumulative mean of counts of the micrographs, revealed that two micrographs provided data representative of fibril banding. The percentage coefficient of variation for the ratio of fibril to matrix measured on the same micrograph on separate occasions was 2.4% for RBM and 2.7% for interstitial collagen.
RESULTS
Two features of fibril ultrastructure were evaluated, fibril width and banding (fig. 1⇑). These features in RBM and interstitial collagen were compared in all age groups.
Fibril width in the RBM and interstitial collagen
Fibril widths were significantly lower in the RBM compared with interstitial collagen in all age groups in both asthma and controls. Infant median (range) fibril width was 47 (37–50) nm in the RBM versus 59 (48–69) nm in interstitial collagen (p<0.001). In children, fibril width was 36 (31–42) nm in the RBM versus 54 (48–69) nm in interstitial collagen (p<0.001). Adult fibril width was 36 (30–49) nm in the RBM versus 61 (48–74) nm in interstitial collagen (p<0.001; fig. 2⇓).

Fibril width in the reticular basement membrane (RBM) compared with interstitial collagen (IC) in infants, children and adults. Horizontal bars represent medians. ***: p<0.001.
Ratio of banded to nonbanded fibrils
There were significantly fewer banded fibrils in the RBM compared with interstitial collagen in all age groups in both asthma and controls (fig. 3⇓).

Ratio of banded to nonbanded fibrils in the reticular basement membrane (RBM) and interstitial collagen (IC) in infants, children and adults. There are more banded fibrils as the ratio increases. Horizontal bars represent medians. #: p<0.03; ***: p<0.001.
Ratio of fibrils to matrix in the RBM
The ratio of fibrils to matrix in the RBM of the adult, paediatric and infant asthmatics was similar to that of the age-matched controls. The median (range) ratio in adult asthmatics versus controls was 0.94 (0.60–1.46) versus 0.64 (0.47–1.10) (p = 0.09). The ratio in paediatric asthmatics versus controls was 1.24 (0.63–2.49) versus 1.31 (0.50–2.57) (p = 0.96) and the ratio in infant asthmatics versus controls was 1.67 (0.68–3.08) versus 1.29 (0.31–2.96) (p = 0.74; fig. 4⇓).

Ratio of fibrils to matrix in the reticular basement membrane in asthmatics compared with age-matched controls (all ages together). There are more fibrils as the ratio increases. Horizontal bars represent medians.
Ratio of fibrils to matrix in bronchial interstitial collagen
In order to assess whether a pattern of a more classical interstitial fibrosis was present within the submucosa of asthmatic tissue, the ratio of fibrils to matrix in the deeper interstital collagen was compared in the adult asthmatics and controls. There was no difference in the ratio of fibrils to matrix in the deeper interstitial collagen between adult asthmatics and controls (1.21 (0.71–1.78) versus 1.18 (0.81–2.15) (p = ns)).
Fibril width and banding in bronchial interstitial collagen and parenchymal collagen in CFA
At all ages, interstitial collagen fibril width was similar to that of the parenchymal collagen of CFA patients. The median (range) collagen width in infants was 59 (48–69) nm versus 54 (48–69) nm in children, 61 (48–74) nm in adults and 55 (43–63) nm in CFA (p = ns; fig. 5⇓). All collagen fibrils in CFA patients were banded.

Interstitial collagen fibril width in infants, children and adults compared with adults with cryptogenic fibrosing alveolitis (CFA). Horizontal bars represent medians. A: asthma; C: control.
Fibril width in RBM in asthma and parenchymal collagen in CFA
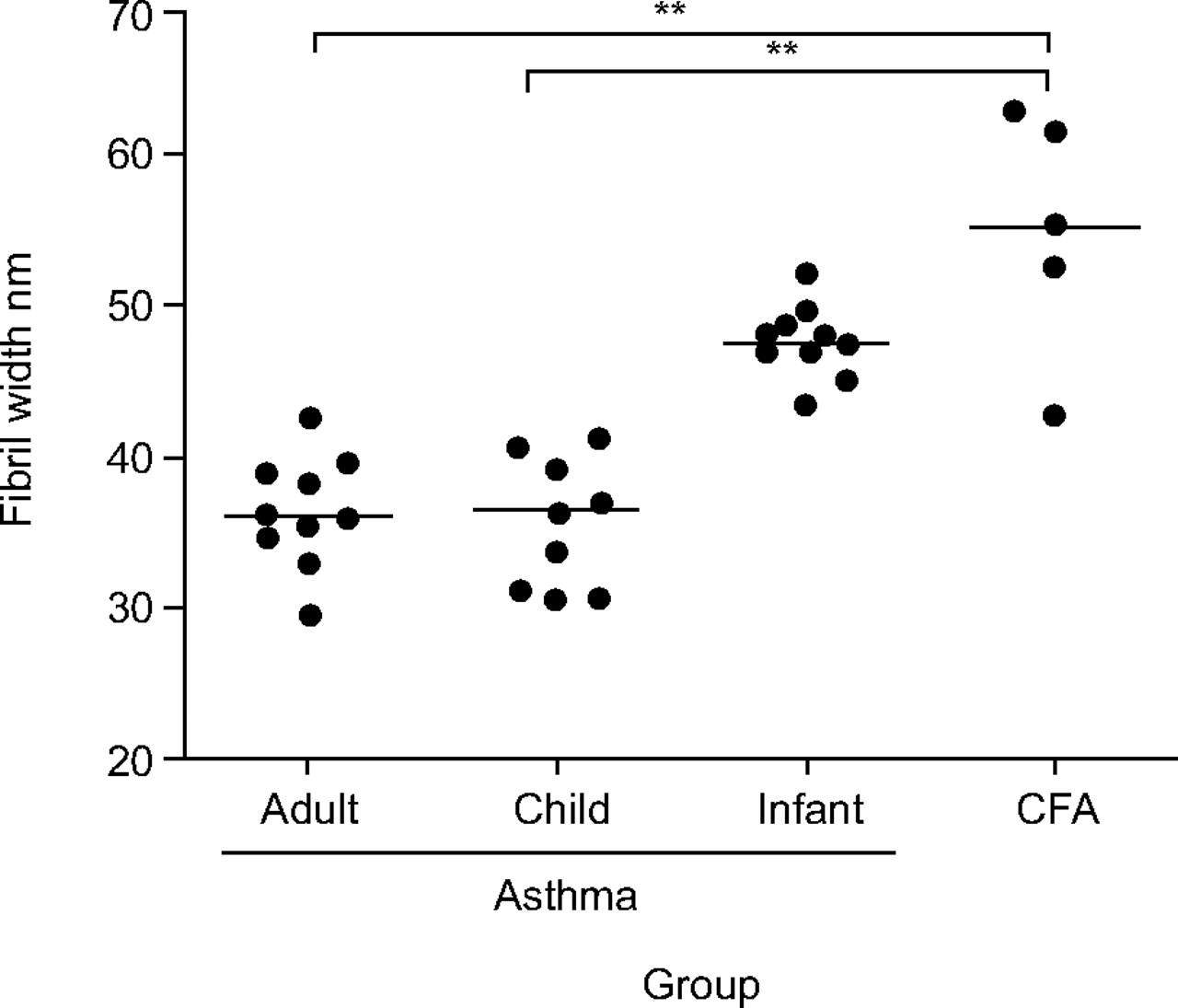
The RBM fibril width, in both adult and paediatric asthmatics, was significantly lower than the parenchymal collagen fibril width of CFA patients (36 (30–43) nm in adult asthma versus 37 (31–41) nm in child asthma and 55 (43–63) nm in CFA (p<0.01 for adult and child asthma versus CFA)). The RBM fibril width was also lower in infants than the parenchymal collagen fibril width of CFA patients, but this difference was not significant (48 (43–52) nm in infants versus 55 (43–63) nm in CFA (p = ns)) (fig. 6⇓).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Reticular basement membrane fibril width in asthmatics of all ages compared with parenchymal collagen fibril width in adults with cryptogenic fibrosing alveolitis (CFA). Horizontal bars represent medians. **: p<0.01.
DISCUSSION
The present study has shown that the ultrastructure of the RBM is distinct to that of bronchial interstitial collagen, the latter being similar to the alveolar wall collagen of pulmonary fibrosis. Even when the RBM is thickened, as in asthma, the fibrils are thinner and less obviously banded than those of airway wall interstitial collagen. Moreover, the ratio of fibrils to matrix in asthma, at all ages, remains unchanged compared with nonasthmatic controls. The present ultrastructural data do not support the hypothesis that thickening of the RBM in asthma results from the same fibrotic process as that seen in fibrotic lung disease.
Collagen is a universal term applied to a family of glycoproteins and includes distinct structural forms such as interstitial collagen, reticulin and constituents of basal laminae 1. In mammals, the fibrils of interstitial collagen are thicker, with a diameter ranging 10–500 nm (mean 60 nm), than those of reticulin and usually follow a wavy course without branching 11. Additionally, interstitial collagen contains fibrils that each have characteristic transverse bands termed D-periodicity with a repetitive band frequency of ∼64–70 nm 15. In contrast, reticulin is composed of fibrils that form a relatively tangled loosely packed network of fine fibrils with a diameter of ∼20–40 nm and absent or at least much less obvious D-periodicity 16. The term subepithelial fibrosis has been suggested and is variously applied by different investigators to describe the characteristic thickening of the RBM layer in asthma 8. To many, the term implies that it is the addition of interstitial collagen that contributes to the RBM thickening, suggesting a fibrotic process similar to that described in IPF.
A previous quantitative study assessed the RBM electron microscopically, but only to determine its thickness in asthma compared with controls 17; none have assessed its ultrastructural composition. The present authors acknowledge that the descriptor reticular of RBM per se already implies a distinction from interstitial collagen. However, it has been demonstrated for the first time, using quantitative and ultrastructural techniques, that the composition of the normal bronchial RBM, as well as of that which is thickened in asthma, is ultrastructurally different from the banded thicker fibrils of interstitial collagen characteristic of fibrotic scarring and that seen in parenchymal collagen from IPF patients. This ultrastructural distinction, together with the lack of a relative increase in the fibrillary component and the nonprogressive nature of the thickening, which has previously been shown to be already maximal in asthmatic children 5, indicates that the process of RBM thickening in asthma is different to the fibrosis characteristic of IPF.
Experimental studies provide support for the present interpretation. In allergen-challenged mice, silver stains (designed to highlight reticulin) demonstrate that subepithelial reticulin in the airways increases three-fold compared with that of sham-challenged mice and that it is this component that contributes to the increased RBM thickness in this animal model of asthma 18. Moreover, it has additionally been shown that both fibrils and matrix increase in equal proportion in human asthma such that the thickened RBM in asthma, in the child or adult, has the same ultrastructural appearance as that of age-matched controls. It has previously been shown that the RBM is present and thickened in both adults 3 and children with asthma 5, 6, and it has recently been reported that the RBM is developed, but not yet thickened, in infants aged <24 months 12. In the present article, it has been shown that age does not influence the ultrastructural composition of the RBM, in either asthmatics or nonasthmatic controls. Also, the ultrastructural appearance of the RBM might differ in patients with more severe disease, defined by the presence of persistent airflow limitation 19. In the present study, this was addressed in children, who all exhibited difficult asthma. Although numbers were small (six with and four without persistent airflow limitation), there were no differences in RBM ultrastructure between the subjects with and without persistent airflow limitation.
One potential criticism of the present study is that the RBM was assessed using only transmission electron microscopy and without the application of immunohistochemical and silver staining techniques to identify reticulin. To apply these, in repetition of previous studies 20, would have required additional biopsy specimens, processed using different techniques to those used for electron microscopy. Sufficiently large numbers of biopsy specimens, particularly from children, were neither available nor ethically approved. Neither was it considered that this was required to reach the present conclusions, since electron microscopy so clearly distinguishes reticulin from fibrils of interstitial collagen without need for special stains 21. Many studies have used immunohistochemical staining techniques to assess which collagen subtypes are increased in the RBM in asthma 17. These researchers have shown that the main components of the RBM are collagen subtypes III 8, 22 and V 8, 17, which is in keeping with increased reticulin, since, immunohistochemically, reticulin fibrils express the epitopes for collagen types III 21, 23 and V 24, whereas interstitial collagen fibrils most closely resemble collagen type I 1, 23. A recent study has reported increased collagen subtype III in both adult and paediatric asthmatics 25. This is probably not due to an increased density of type III collagen, but rather the result of an increase in the total thickness of the RBM. Moreover, such a light microscopic study, in which immunostaining is performed, does not permit assessment of the ratio of fibrils to matrix in the thickened asthmatic RBM; for this, electron microscopy is required. As undertaken previously, but using snap-frozen material 8, immunostaining of paraffin wax-embedded biopsy specimens was performed for collagen subtypes I, III and V in cases in which tissue was available; this was in addition to the ultrastructural assessment of all plastic-embedded biopsy specimens. The clear discrimination that was observed between RBM reticulin and deeper interstitial collagen by electron microscopy was not reflected by similarly distinct distributions of collagen type III. Also, the variability associated with staining for collagen types I and V in the biopsy specimens that had been processed into paraffin wax made their interpretation unconvincing.
Thus, although it is acknowledged that the epithelial RBM of asthma stains for the epitopes that mark collagen, the present authors consider that electron microscopy is a technique which offers an additional and novel means of examining and comparing the structural components of the RBM and interstitial collagen in asthma, and that there are marked differences in structure between the composition of the RBM and deeper bronchial or parenchymal interstitial collagen, the latter taken from patients with fibrosing lung disease.
Finally, myelofibrosis is a condition involving increased bone marrow deposition of collagen and reticulin 26. In bone marrow disease, the term reticulin fibrosis or collagen fibrosis is used 27, and a variable response of reticulin fibrosis to corticosteroids has been reported 27. Even in patients with CFA, variable amounts of both type I and III collagen are present, and patients with a larger proportion of type III collagen show a better response to steroid therapy 28. This is consistent with evidence that long-term steroid therapy can result in a reduction in RBM thickness in asthma 29. The present authors suggest that a distinction between reticulin fibrosis and collagen fibrosis be recognised in asthma, and that that the former term would be more appropriate and specific than the term subepithelial fibrosis. Alternatively, the term reticular basement membrane thickening, although less specific, is accurate, less likely to confuse and implies an as yet equivocal mechanism for explaining its thickening in asthma.
In summary, it has been shown, by ultrastructural examination, that reticular basement membrane thickening in asthma represents not interstitial collagen but rather increased deposition of reticulin and matrix in equal and normal proportion. These findings, in children and adults, led to the conclusion that the reticular basement membrane thickening in asthma represents an increased quantity of lamina reticularis of the same composition as that found in healthy individuals. Although immunostaining identifies epitopes usually associated with collagen, the present ultrastructural data demonstrate distinctions from the interstitial collagen associated with fibrosis and challenge the notion that the reticular basement membrane and its thickening in asthma are the result of a fibrotic process of the kind seen in fibrotic lung disease.
Acknowledgments
The authors would like to thank A. Dewar and the Dept of Histopathology (Royal Brompton Hospital, London, UK) for their help in identifying the subjects with cryptogenic fibrosing alveolitis.
- Received May 12, 2005.
- Accepted April 11, 2006.
- © ERS Journals Ltd
References










