





Abstract
A disease-related, corticosteroid-insensitive increase in the expression of epidermal growth factor (EGF) receptor (EGFR) tyrosine kinase in asthmatic bronchial epithelium has been shown previously by the current authors. To determine whether this is associated with enhanced intracellular signalling, the aim of this study was to evaluate epithelial tyrosine phosphorylation.
Bronchial biopsies were analysed for the presence of phosphotyrosine by immunohistochemistry. Bronchial epithelial cells were exposed to EGF, hydrogen peroxide or tumour necrosis factor-α in vitro for measurement of tyrosine phosphorylated signalling intermediates and interleukin (IL)-8 release.
Phosphotyrosine was increased significantly in the epithelium of severe asthmatics when compared with controls or mild asthmatics; however, in mild asthma, phosphotyrosine levels were significantly decreased when compared with controls. There was no significant difference between phosphotyrosine levels before or after 8 weeks of treatment with budesonide. Stimulation of bronchial epithelial cells resulted in tyrosine phosphorylation of several proteins, including EGFR, Shc and p42/p44 mitogen-activated protein kinase. In the presence of salbutamol, a transient partial suppression of EGFR phosphorylation occurred, whereas dexamethasone was without effect. Neither salbutamol nor dexamethasone inhibited EGF-stimulated IL-8 release.
These data indicate that regulation of protein tyrosine kinase activity is abnormal in severe asthma. The epidermal growth factor receptor and/or other tyrosine kinase pathways may contribute to persistent, corticosteroid-unresponsive inflammation in severe asthma.
- β2-Adrenoceptor agonist
- bronchial epithelium
- corticosteroid
- epidermal growth factor receptor
- intracellular signal transduction
- tyrosine kinase
Asthma is a chronic inflammatory disorder, characterised by bronchial hyperresponsiveness to a wide variety of environmental factors 1. In addition to inflammation, asthmatic airways show features of “remodelling”, including deposition of extracellular matrix proteins, epithelial damage, goblet cell hyperplasia and smooth muscle hyperplasia 2, 3. Whether these features occur as a consequence of, or in parallel with, the inflammatory response is not known, but increasingly it is being appreciated that many of the structural elements of the airways are themselves altered to produce cytokines, growth factors and mediators that may contribute to sustaining the inflammatory response 4.
Epithelial damage and activation is a characteristic feature of asthma 5–8. This can account for its altered phenotype 9, 10, with enhanced expression of heat shock proteins 11 and the cyclin-dependent kinase inhibitor p21waf 12, activation of transcription factors 13–15, and increased expression and release of cytokines and mediators 16, 17. The extent of epithelial injury in asthma is reflected by changes in expression of the epidermal growth factor (EGF) receptor (EGFR; HER1, ErbB1), the levels of which are increased in proportion to asthma severity and are refractory to corticosteroid therapy 18. The EGFR has intrinsic tyrosine kinase activity, which, when activated, catalyses phosphorylation of a variety of intracellular substrates, leading to activation of a cascade of signalling moieties that may themselves possess kinase activity (e.g. components of the extracellular signal-related kinase (ERK)/mitogen-activated protein kinase (MAPK) pathway). The EGFR plays a pivotal role in epithelial cells by virtue of its ability to be activated not only by its cognate ligands, but also to be transactivated by G-protein-coupled receptors and stress stimuli, such as oxidants, ultraviolet radiation and mechanical injury 19. Hence, the EGFR acts as a conduit that mediates cellular responses to many external stimuli. In addition to the EGFR and its downsteam pathways, the bronchial epithelium expresses a variety of other receptor-linked tyrosine kinases that have the potential to be activated in asthma. For example, the current authors have shown previously that human bronchial epithelial cells respond to interleukin (IL)-4 and IL-13 with tyrosine phosphorylation of STAT (signal transducer and activator of transcription)6 mediated by members of the JAK (Janus kinase) family 20. Bronchial epithelial cells also respond to environmental stress and endogenous cytokines, such as tumour necrosis factor (TNF)-α and IL-1β through activation of p38 MAPK 21 and jun N-terminal kinase (JNK) 22.
Recognising that the asthmatic bronchial epithelium displays an activated phenotype, it was hypothesised that this would be reflected by an increase in tyrosine phosphorylation due to the activation of stress signalling pathways. Therefore, the extent of tyrosine phosphorylation in bronchial biopsies was compared in this study using immunohistochemistry. In parallel, likely substrates for epithelial tyrosine kinases were examined in vitro. Finally, the influence of corticosteroids and β2-adrenoceptor agonists on tyrosine phosphorylation linked to proinflammatory mediator release was examined.
MATERIALS AND METHODS
Subjects
Archival biopsies were used for assessment of phosphotyrosine levels. These were from: eight nonatopic subjects without asthma (three males and five females), with a mean age of 21.4±0.9 yrs and forced expiratory volume in one second (FEV1) of 103±2.4% predicted; nine atopic subjects with mild asthma (two males and seven females) with a mean age of 29.2±9.5 yrs and FEV1 of 90.9±7.6% pred; and nine subjects (of whom four were atopic) with moderately severe asthma (five males and four females) with a mean age of 40.8±15.5 yrs and FEV1 of 51.4±19.2% pred. The mild asthmatics were using short-acting β2-agonists only to control their disease, whereas those with moderately severe asthma were also using inhaled corticosteroids. To assess the effects of corticosteroids, archival biopsies were used from 15 atopic mild-to-moderate asthmatic subjects (eight males and seven females) before and after 8 weeks of treatment with inhaled budesonide (400 μg twice daily); mean age was 27.7±1.9 yrs and mean FEV1 was 93.2±3.4 L before treatment and 96.3±2.8 L after treatment. Primary bronchial epithelial cells were established from bronchial brushings obtained from 12 atopic asthmatic subjects (five males and seven females) with a mean age of 40.7±5.2 yrs and mean FEV1 of 78.2±4.0 L.
All subjects were nonsmokers and had not experienced recent symptoms of upper respiratory tract infection within the previous 4 weeks. Atopic status was confirmed by skin-prick testing to a panel of common aeroallergens and assessment of asthma severity was in accordance with GINA (Global Initiative for Asthma) guidelines 23. The studies were approved by the Southampton Joint University and Hospitals Ethics Committee (Southampton, UK) and the University of Umeå Ethics Committee (Umeå, Sweden). All subjects had given their written consent after being fully informed about the nature and purpose of the study. Fibreoptic bronchoscopy and bronchial biopsy or brushings were performed as previously described 24, following the most recent guidelines 25.
Immunohistochemistry
Biopsies embedded in glycol methacrylate resin were immunostained using a streptavidin-biotin-peroxidase detection system 26 with primary mouse monoclonal antibodies against phosphotyrosine (clone PY20, biotinylated), inducible nitric oxide synthase (iNOS; Transduction Laboratories, Oxford, UK) and nitrotyrosine (clone 1A6; TCS Biologicals, Buckinghamshire, UK); isotype-matched antibodies (including a biotinylated antibody as control for PY20 antibody) were used as controls. The specificity of the phosphotyrosine antibody has been reported previously 27. Epithelial phosphotyrosine, iNOS and nitrotyrosine in two nonserial sections were quantified by computer-assisted image analysis based on RGB (red, blue, green) colour balance 18. Immunostaining was expressed as percentage of total intact epithelial area. All measurements were performed by an observer who was blinded to the clinical group from which the biopsy was derived. The number of phosphotyrosine-positive cells in the submucosa were counted and expressed as the total number cells per mm2 of submucosal tissue.
In vitro studies using bronchial epithelial cells
Primary epithelial cells were cultured in bronchial epithelium growth medium (Clonetics, San Diego, CA, USA) and characterised as previously described 28. To analyse tyrosine phosphorylation, cells were grown to 70% confluence and serum-starved for 24 h. They were then treated with EGF, hydrogen peroxide (H2O2), TNF-α or IL-1β for up to 1 h. For direct analysis by SDS-PAGE and Western blotting, cell lysates were harvested into an SDS-containing sample buffer; for immunoprecipitation, cells were harvested into denaturing lysis buffer and phosphotyrosine-containing proteins immunoprecipitated using PY20 agarose 18. Levels of immunoreactivity were quantified by densitometry using GeneTools (Syngene Bio-imaging Systems, Cambridge, UK). IL-8 release in response to EGF stimulation was measured by ELISA 29.
Statistical analyses
Data were not normally distributed, and are expressed as medians and interquartile ranges. Comparisons between groups were made using the Mann-Whitney U-test and within groups using Wilcoxon's rank-sum test. A p-value of <0.05 was regarded as statistically significant.
RESULTS
Protein tyrosine phosphorylation in normal and asthmatic bronchial mucosa
Immunohistochemistry using a biotinylated phosphotyrosine-specific antibody revealed that the bronchial epithelium was a major site of tyrosine phosphorylation (fig. 1a–c⇓). Normal subjects showed immunostaining around the nuclei of columnar epithelial cells, while staining of the basal cells was restricted to the region in contact with the basement membrane (fig. 1a⇓). Biopsies from mild asthma exhibited weak staining of the columnar cells with little staining in the proximity of the basement membrane (fig. 1b⇓). Severe asthmatics showed higher levels of tyrosine phosphorylation than normal subjects or mild asthmatics, with staining present throughout the epithelium in both columnar and basal epithelial cells. Immunostaining was particularly strong around cell membranes, suggesting membrane-bound receptor tyrosine phosphorylation (fig. 1c⇓). Cells in the submucosa also showed some evidence of tyrosine phosphorylation, with both cytoplasmic and membrane immunostaining evident in all subject groups. There was no obvious partitioning of epithelial phosphotyrosine immunostaining within a specific cell type (e.g. goblet cells). The specificity of the PY20 antibody was confirmed using a biotinylated immunoglobulin G2b isotype-matched control antibody, which showed no immunoreactivity (fig. 1d⇓).

Phosphotyrosine immunostaining in human bronchial biopsies. Representative immunostaining of 2-μm sections from bronchial biopsies from a) normal, b) mild and c) severe asthmatic subjects analysed using the PY20 antibody. The arrow indicates phosphotyrosine-positive cells in the submucosa. d) A biotinylated isotype-matched control antibody was used to immunostain a representative section, and shows no staining. Scale bars = 40 μm.
Using computer-assisted image analysis, protein tyrosine phosphorylation was found to be significantly increased in the bronchial epithelium of severe asthmatics (% epithelial staining 20.6 (13.6–56.3)) when compared with normal controls (12.8 (2.5–41.3), p = 0.02) or mild asthmatic subjects (2.4 (0.6–13.9), p = 0.001). However, tyrosine phosphorylation was significantly decreased in the bronchial epithelium of mild asthmatics when compared with normal controls (p = 0.005) and severe asthmatics (p = 0.001, fig. 2a⇓). The number of phosphotyrosine-positive cells in the submucosa was not found to differ significantly between any of the subject groups (fig. 2b⇓).

Quantitation of phosphotyrosine levels in normal and asthmatic bronchial biopsies. Phosphotyrosine immunostaining in the bronchial biopsies of nonasthmatic (n = 8), mild (n = 9) and severe (n = 9) asthmatic subjects was assessed using an image analysis system. a) Epithelial staining, b) the number of phosphotyrosine-positive cells in the submucosa and c) phosphotyrosine levels in bronchial epithelium of 15 asthmatic subjects before and after 8 weeks of treatment with inhaled corticosteroids. Box and whisker plots show median value, interquartile range and 5–95% confidence intervals. Statistical significance was determined using the Mann-Whitney U-test. #: p = 0.60; ¶: p = 0.14; +; p = 0.11; §: p = 0.02; ***: p = 0.001; ƒ: p = 0.005; ##: p = 0.307.
The effect of corticosteroids on protein tyrosine phosphorylation
To assess whether the difference in tyrosine phosphorylation between mild and severe asthmatics was due to use of corticosteroids, bronchial biopsies were taken from 15 mild-to-moderate asthmatic subjects before and after treatment with inhaled budesonide (400 μg twice daily for 8 weeks) and analysed for phosphotyrosine immunoreactivity. As peroxynitrite, which is formed by the combination of superoxide anions and nitric oxide, is elevated in corticosteroid-naive asthmatics 30, iNOS expression and nitrotyrosine, as well as phosphotyrosine, were analysed to investigate whether nitration of tyrosine residues by peroxynitrite might interfere with the ability of tyrosine kinases to phosphorylate protein tyrosine residues.
Of the 15 subjects studied, 10 showed increased levels of phosphorylation after corticosteroid treatment; however, overall phosphotyrosine levels as a per cent epithelial staining were not significantly different pre- or post-treatment (pre-treatment 1.8% (0.4–7.3), post-treatment 2.6% (0.4–11.9), p = 0.307, fig. 2c⇑). There was a trend for decreased levels of iNOS after corticosteroid treatment (4.2% (0.4–7.9) and 3.3% (0.1–8.14) pre- and post-treatment, respectively), with 10 out of the 15 subjects showing a decrease in iNOS levels; however, this failed to reach statistical significance (p = 0.211). Similarly, nitrotyrosine levels were not significantly affected by corticosteroid treatment (2.8% (0.4–6.1) and 2.3% (1.1–6.9) pre- and post-treatment, respectively, p = 0.609).
Analysis of protein tyrosine kinase substrates in bronchial epithelial cells
Whilst the PY20 antibody detected phosphotyrosine residues in the bronchial epithelium, it did not identify specific substrates. Several phosphospecific antibodies were assessed for their ability to detect specific substrates (e.g. phospho-JNK and phospho-p38 MAPK). However, these failed to give a signal detectable above background; characterisation of five phospho-EGFR antibodies showed that each produced considerable nonspecific immunoreactivity on Western blotting, preventing specific evaluation of EGFR phosphorylation in the biopsies.
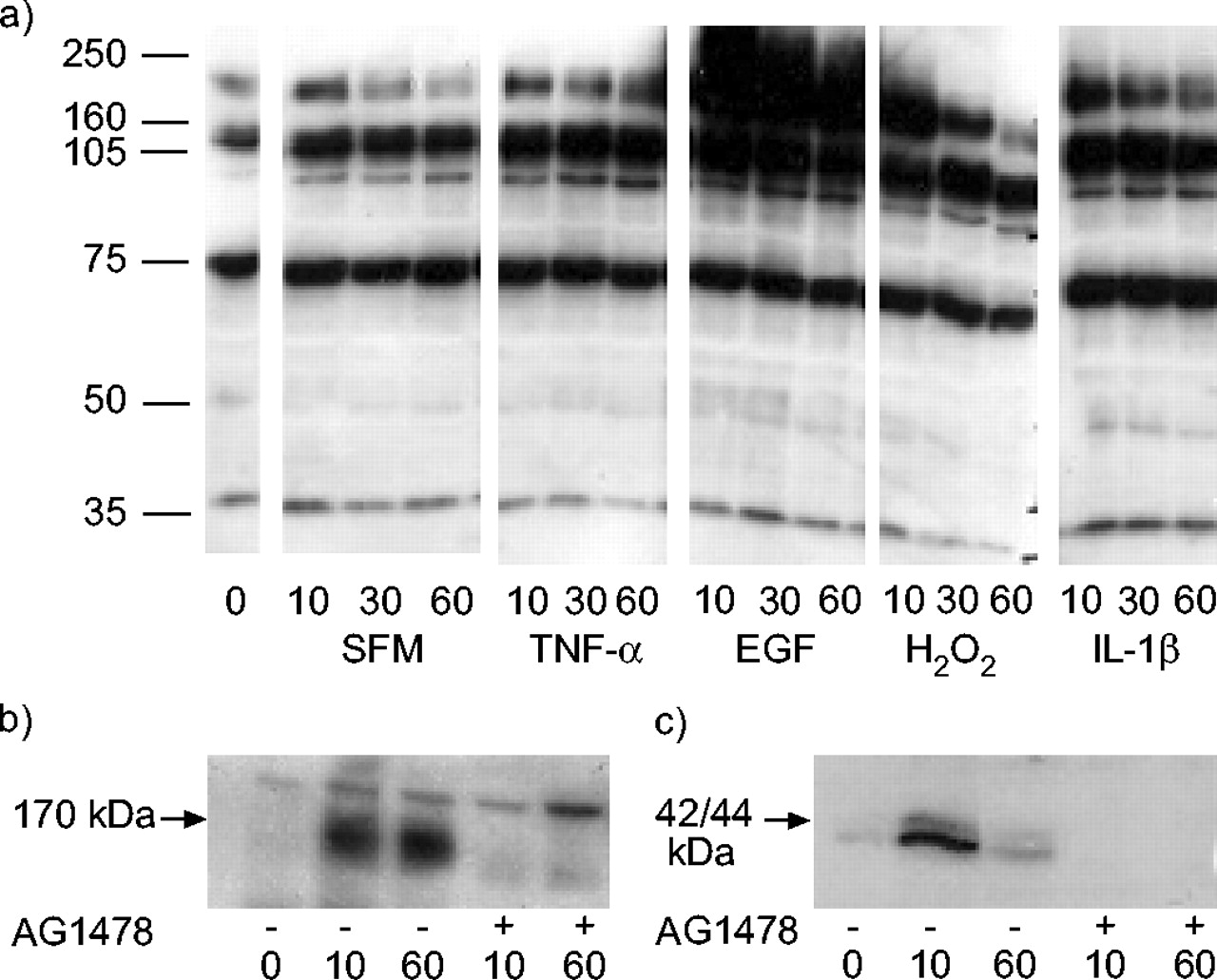
To identify potential substrates for epithelial tyrosine kinases, in vitro studies were conducted using H292 and primary bronchial epithelial cells, with similar results being obtained in each case. Cells were treated with a variety of relevant stimuli, including the growth factor EGF, the pro-inflammatory cytokines TNF-α and IL-1β, and the oxidant H2O2; phosphotyrosine levels in cell lysates were analysed by SDS-PAGE and Western blotting. When compared with lysates of untreated cells, the most active stimuli were found to be EGF and H2O2, both of which caused an overall increase in tyrosine phosphorylation, with a marked increase in phosphorylation of a band at 170 kDa, consistent with being the EGFR (fig. 3a⇓). EGF caused a large increase in tyrosine phosphorylation of this protein for up to 1 h. H2O2 caused an immediate but transient increase that returned to baseline by 1 h. Phosphorylation of the 170-kDa protein was inhibited by the EGFR-selective tyrphostin AG1478, consistent with its identification as the EGFR (fig. 3b⇓). Additional weakly phosphorylated proteins were detected at 42–44 kDa, 52 kDa and 66 kDa, consistent with the molecular weights of the ERK–MAPK and two of the three Shc isoforms, respectively. These were confirmed by immunoprecipitation and Western blotting (for Shc; data not shown) or with the use of a phosphospecific antibody (p42/44 MAPK; fig. 3c⇓).

The effect of stimuli on tyrosine phosphorylation in bronchial epithelial cells. H292 or primary asthmatic bronchial epithelial cells were treated with a control, serum-free medium (SFM), tumour necrosis factor (TNF)-α, epidermal growth factor (EGF), hydrogen peroxide (H2O2) or interleukin (IL)-1β for 10, 30 or 60 min as indicated. a) Tyrosine-phosphorylated proteins in H292 cells were detected by SDS-PAGE and Western blotting using PY20 antibody. EGF-stimulated primary cells in the absence or presence of 1 μM tyrphostin AG1478 were probed with b) a PY20 antibody and c) a phospho-extracellular signal-related kinase/mitogen-activated protein kinase-specific antibody. Data are representative of a minimum of three independent experiments.
As previously reported, EGFR expression levels are insensitive to corticosteroid therapy 18; therefore, the effect of dexamethasone on EGFR activation was assessed by measuring tyrosine phosphorylation of the 170-kDa band. Untreated H292 cells had a basal level of tyrosine phosphorylation that was unaffected by the addition of 1 μM dexamethasone (data not shown). In the presence of EGF, there was an increase in tyrosine phosphorylation of the 170-kDa band and this appeared to be slightly enhanced by 1 μM dexamethasone, although this change failed to reach statistical significance (38±25%, p>0.05, n = 4, fig. 4a⇓). Confirmation that the band was the EGFR was obtained by immunoprecipitation and Western blotting with monoclonal and polyclonal anti-EGFR antibodies (fig. 4b⇓). Dexamethasone also failed to significantly affect the levels of phosphorylated EGFR (40±33%, p>0.05, n = 5) or phospho-ERK–MAPK in primary bronchial epithelial cells (fig. 4c⇓ and d).

The effect of dexamethasone on epidermal growth factor (EGF)-stimulated tyrosine phosphorylation in bronchial epithelial cells. H292 or primary asthmatic bronchial epithelial cells were treated with EGF for 10 or 60 min in the absence or presence of dexamethasone (Dex.; 1 μM). Tyrosine-phosphorylated proteins were detected by SDS-PAGE and Western blotting using a PY20 antibody (a and c, H292 and primary cells, respectively). b) H292 cells were lysed into denaturing lysis buffer and tyrosine-phosphorylated proteins immunoprecipitated using PY20 agarose. After SDS, the resulting immunoprecipitate was analysed for the presence of the EGF receptor. c) The effect of 1 μM dexamethasone on asthmatic primary bronchial epithelial cells was assessed using PY20 antibody and d) phospho-extracellular signal-related kinase (ERK) was analysed using a specific phospho-ERK–mitogen-activated protein kinase antibody. Data are representative of a minimum of three independent experiments.
Since phosphotyrosine levels were decreased in mild asthma, it was also investigated whether β2-agonists had any inhibitory effect on EGFR tyrosine phosphorylation. In this case, addition of the selective β2-adrenoceptor agonist, salbutamol, caused a partial but significant (55±5%, p<0.05) suppression of EGF-stimulated phosphorylation of the 170-kDa band, which was more evident at the early time point (fig. 5⇓).

The effect of salbutamol on epidermal growth factor (EGF)-stimulated tyrosine phosphorylation in bronchial epithelial cells. Asthmatic primary bronchial epithelial cells were treated with serum-free medium (SFM) or EGF for 10 or 60 min in the absence (▪) or presence of salbutamol (1.0 μM (□) and 0.1 μM (▪), respectively). Tyrosine-phosphorylated proteins were detected by SDS-PAGE and Western blotting using PY20 antibody. Phosphorylation of the EGF receptor was quantified by densitometry and normalised to SFM at zero time point. Data are presented as mean±sd (n = 5). *: p<0.05 compared with EGF alone at 10 min.
Effects of corticosteroids and β-agonists on EGF-stimulated epithelial responses
As it has been shown that EGFR expression is increased in asthma and correlates with epithelial IL-8 expression, the effects of dexamethasone and salbutamol on EGF-stimulated IL-8 release from primary cultures of asthmatic bronchial epithelial cells were investigated. Exposure to EGF caused IL-8 release from the cells, but this was corticosteroid insensitive (fig. 6⇓). EGF-stimulated IL-8 release was also insensitive to the presence of salbutamol, either alone or in combination with dexamethasone (data not shown), even though a requirement for EGFR tyrosine kinase activity was confirmed using the selective inhibitor, tyrphostin AG1478.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The effect of dexamethasone and salbutamol on epidermal growth factor (EGF)-stimulated interleukin (IL)-8 release. Primary bronchial epithelial cells from asthmatic subjects were cultured and treated for 24 h with serum-free medium (▪) or EGF (▪) plus or minus 1 μM dexamethasone (Dex.), 1 μM salbutamol (Salb.) or 1 μM AG1478. IL-8 release was measured by ELISA. Each condition was repeated in duplicate and data shown are the average of seven individual experiments. *: p<0.05 when compared with unstimulated cells.
DISCUSSION
Protein tyrosine phosphorylation is a key post-translational mechanism that controls intracellular signal transduction to a variety of exogenous and endogenous stimuli. It is catalysed by the activity of tyrosine kinases and is particularly involved in responses to stressful stimuli and cell growth. Phosphotyrosine has been detected in neoplastic lesions, where it has been associated with aberrant kinase activity, but has also been observed in embryonic and adult tissue, where it is thought to reflect the presence of physiologically active kinases 31, 32. Based on the evidence that the asthmatic bronchial epithelium has upregulated expression of EGFR 18 and activation of transcription factors such as nuclear factor (NF)-κB 13, it was postulated that phosphotyrosine levels would be elevated as a consequence of cellular activation. While this was the case in severe asthma, it was surprising to find that in mild asthma a significantly lower level of tyrosine phosphorylation was apparent when compared with either the severe asthmatic or normal subject groups. Thus, although there is a possibility that some phosphorylated proteins may be too short lived to capture in a fixed biopsy that represents a single point in the disease process, this study provides the first evidence that protein tyrosine phosphorylation is significantly altered in the bronchial epithelium of asthmatic subjects when compared with normal controls. Although the phosphorylated substrates could not be directly identified in vivo, studies conducted in vitro revealed several likely substrates, including EGFR, isoforms of the adaptor molecule, Shc, and p42/p44 MAPK.
In previous studies, epithelia from a variety of tissues have exhibited phosphotyrosine immunostaining either at the apical aspect or at the entire contact region between neighbouring cells, suggesting association with cytoskeletal elements. In contrast, in the bronchial biopsies from normal and mild asthmatic subjects, the phosphotyrosine staining was usually localised to the basement membrane; however, this also suggests that cytoskeletal interactions, possibly involving cell adhesion and integrin-mediated signalling 33, are active; in subjects with severe asthma, there was also strong immunostaining around cell membranes suggesting membrane-bound receptor tyrosine phosphorylation, consistent with the high levels of EGFR expression seen in severe asthma.
While phosphotyrosine levels were increased in severe asthma, in mild asthma there was a significantly lower level of tyrosine phosphorylation when compared with either the severe asthmatic or normal subject groups. This was an unusual finding as disease markers tend to increase or decrease according to disease severity, as the current authors have previously reported for the EGFR 18. Using correlation statistics, this difference in phosphotyrosine levels could not be accounted for by any differences in the age or sex of the subjects, but was best explained in terms of disease group. Recognising that the two groups of asthmatic subjects received different treatments, the possibility that these differences were a consequence of the different therapeutic approaches used in these two asthma groups was explored. One of the consequences of corticosteroid treatment is a reduction in exhaled nitric oxide 30. It was postulated that this would lead to reduced peroxynitrite formation and reduced nitration of tyrosine residues leaving more available for phosphorylation. However, no relationship could be found between phosphotyrosine levels and either corticosteroid use or nitrotyrosine levels. Although iNOS did not show a statistically significant decrease in expression after an 8-week trial with inhaled corticosteroids, 10 out of the 15 subjects did show a decrease in their levels of immunostaining after corticosteroids, indicating a trend towards suppression of nitric oxide production. In a previous study 30, levels of iNOS and peroxynitrite decreased significantly after administration of 800 μg budesonide twice daily for 4 weeks, whereas the subjects in the current study had received only 400 μg twice daily, but for 8 weeks. This difference in dosage may provide a possible explanation for the significant decrease in peroxynitrite and iNOS seen in the previous study.
While it is possible that a higher dose or longer-term treatment with inhaled or oral (as used by some subjects in the original study group) corticosteroids may be an explanation for the higher phosphotyrosine levels in the bronchial epithelium of severe asthmatic subjects, this possibility is not supported by the in vitro studies with primary bronchial epithelial cells, which showed that exposure to corticosteroids had no significant effect on protein tyrosine phosphorylation, including phosphorylation of the EGFR. Instead, it seems more likely that, in severe asthma, increased expression of tyrosine kinases, such as the EGFR, is accompanied by increased activation, with consequent effects on phosphotyrosine levels and cell signalling. However, as tyrosine phosphorylation is a transient modification that is reversible by the activity of phosphotyrosine phosphatases 34, differences in phosphotyrosine levels may reflect differences in phosphotyrosine phosphatase levels, which may be lower in severe asthma, or higher in mild asthma, with consequential effects on the extent of epithelial activation. It is known that bronchial epithelial cells express several phosphotyrosine phosphatases, including protein tyrosine phosphatase (PTP)-1B 35; however, there has been no systematic study in asthma. As PTP levels have been recently found to be regulated by tissue injury, it is possible that the extent of epithelial damage in asthma may differentially modulate PTP expression 36. Regardless of whether the observed differences in phosphotyrosine levels arise due to altered kinase or phosphatase levels (or both), the data presented here suggest that there is suppression of signalling pathways in the epithelium of mild asthmatics, whereas there is activation in severe asthma. This will have many possible consequences, including differential effects on the epithelial phenotype in these two subgroups. It would be of interest to determine if this has any predictive value in terms of disease severity or chronicity.
It was also investigated whether the different levels of tyrosine phosphorylation in the two asthmatic groups could be a consequence of β2-agonist treatment. β2-Agonists cause an increase in cyclic adenosine monophosphate (cAMP) with activation of cAMP-dependent protein kinase, which has been shown to catalyse phosphorylation of the EGFR on serine residues and prevent tyrosine phosphorylation 37. The present results agree with this previous work by showing that salbutamol suppresses the immediate tyrosine phosphorylation of the EGFR induced by EGF. However, it did not affect phosphorylation at longer time points and had no effect on EGF-stimulated IL-8 release. These data are consistent with a previous report in which salbutamol failed to affect basal or TNF-α-stimulated IL-8 release from primary bronchial epithelial cells 38. Whether salbutamol affects other, more acute, responses to EGF, such as membrane and cytoskeletal changes, resulting in downstream effects on epithelial repair remains to be determined. This may be particularly relevant, given the localisation of phosphotyrosine staining along the basement membrane region. Since the most effective treatment for moderately severe asthma is combined therapy with both corticosteroids and β2-agonists, it would be of interest to explore further differences in phosphotyrosine levels associated with use of long- or short-acting β2-agonist use and their interactions with corticosteroids.
The corticosteroid, dexamethasone, also failed to affect either EGFR phosphorylation or EGF-stimulated IL-8 release from asthmatic bronchial epithelial cells, contrasting with its ability to inhibit cytokine-stimulated IL-8 release via NF-κB. The lack of effect of dexamethasone on primary epithelial cells is even more marked than that which was previously reported for EGF-stimulated IL-8 release from H292 cells 29. In the previous study, a strong correlation between EGFR and IL-8 expression in severe asthma was also reported. The insensitivity of the proinflammatory responses of the EGFR to corticosteroids may be important in severe asthma, which is characterised by overexpression of the EGFR, increased tyrosine phosphorylation and neutrophilic inflammation.
In conclusion, the data presented here indicate that regulation of protein tyrosine kinase activity is abnormal in severe asthma and provide novel insight into the effects of treatment on epidermal growth factor receptor-mediated responses, which may be relevant to the disease, as epidermal growth factor receptor is overexpressed in asthma 18. Furthermore, the data suggest other avenues that may be fruitful to explore in asthma (e.g. expression of phosphotyrosine phosphatases). This difference in activation of signalling pathways in mild and severe asthmatics may influence the epithelial phenotype in these two subgroups and raise the possibility that anti-asthma drugs may themselves modulate epithelial responses to injury.
Acknowledgments
The authors would like to acknowledge the contribution of M. Thornber and M. Steel in the recruitment and clinical characterisation of volunteers and bronchoscopy.
Footnotes
-
For editorial comments see page 945.
- Received August 24, 2004.
- Accepted February 18, 2005.
- © ERS Journals Ltd
References









