Risk factors for lower respiratory complications of rhinovirus infections in elderly people living in the community: prospective cohort study
BMJ 1996; 313 doi: https://doi.org/10.1136/bmj.313.7065.1119 (Published 02 November 1996) Cite this as: BMJ 1996;313:1119
- Karl G Nicholson, senior lecturer in infectious diseasesa,
- Julie Kent, research assistanta,
- Victoria Hammersley, research assistanta,
- Esperanza Cancio, postdoctoral research fellowa
- a Leicester University School of Medicine, Department of Microbiology and Immunology, Leicester LE1 9HN
- Correspondence to: Dr Nicholson.
- Accepted 6 September 1996
Abstract
Objective: To assess the role of rhinoviruses in elderly people living in the community.
Design: Prospective community based surveillance of elderly people, without intervention. Subjects were telephoned weekly to identify symptomatic upper respiratory tract infections. Symptoms and impact of illnesses were monitored, and specimens were collected for diagnostic serology and human rhinovirus polymerase chain reaction.
Setting: Leicestershire, England.
Subjects: 533 subjects aged 60 to 90.
Main outcome measures: Symptoms, restriction of activity, medical consultations, and antibiotic use during 96 rhinovirus infections. Adjusted odds ratios for lower respiratory syndromes with respect to smoking and health status.
Results: A viral cause was established in 211 (43%) of 497 respiratory illnesses; rhinoviruses were identified in 121 (24%) and as single pathogens in 107. The median duration of the first or only rhinovirus infection in the 96 people with 107 rhinovirus infections was 16 days; 18 of the 96 patients were confined to bed and 25 were unable to cope with routine household activities. Overall, 60 patients with rhinovirus infections had lower respiratory tract syndromes; 41 patients consulted their doctor, 31 of them (76%) receiving antibiotics. One patient died. Logistic regression analysis showed that chronic medical conditions increased the estimated probability of lower respiratory rhinovirus illness by 40% (95% confidence interval 17% to 68%) and smoking by 47% (14% to 90%). There were almost six times as many symptomatic rhinovirus infections as influenza A and B infections.
Conclusions: Rhinoviruses are an important cause of debility and lower respiratory illness among elderly people in the community. Chronic ill health and smoking increase the likelihood of lower respiratory complications from such infections. The overall burden of rhinovirus infections in elderly people may approach that of influenza.
Key messages
Rhinoviruses are responsible for more colds in elderly people living in the community than are other respiratory pathogens combined
Almost two thirds of elderly people with rhino- virus infections can be expected to develop lower respiratory illness
More than 40% of rhinovirus infections in elderly people are seen by medical practitioners, and three quarters of those consulting are prescribed antibiotics
Risk factors for lower respiratory rhinovirus illness include chronic medical conditions and cur- rent smoking; past smoking is not an independent risk factor and stopping smoking is the only factor identified thus far that could reduce the severity of rhinovirus illness in elderly people
Introduction
There are more than 100 serologically distinct types of human rhinovirus. Their importance in the aetiology of the afebrile coryzal syndrome,1 2 3 4 otitis media,5 sinus infection,6 lower respiratory illness including pneumonia,7 8 9 10 11 and exacerbations of chronic bronchitis12 13 14 and asthma15 has been recognised for many years. In the Tecumseh study of respiratory infections in families Monto et al noted an increase in the frequency of lower respiratory illness, restriction in activity, and medical consultations in people over 40 with rhinoviruses compared with younger adults.16 However, only 17 isolates were obtained from people older than 40, and their age distribution was not reported.
Remarkably little is known about the aetiology, prevalence, and impact of acute respiratory infections among elderly people living in the community. One of the most profound changes accompanying the growth in the British population has been the rapid rise in the numbers of elderly people. Official projections suggest that their numbers will continue to grow at an even greater rate during the next two decades.17 We evaluated the role of rhinoviruses in elderly people by means of community based surveillance and a semi-nested reverse transcriptase polymerase chain reaction for rhinoviruses.18
Subjects and methods
The study was conducted during the winters of 1992–3 and 1993–4 in Leicestershire. During April to June 1992 we sent letters to 800 of the 129 000 people aged 60 years and older who lived in Leicestershire inviting them or their spouse, or both, to participate in the study; the sample was randomly selected by the family health services authority computer. Patients living in residential care were excluded. Basic demographic data, medical and drug history, and a baseline blood sample were collected at recruitment. A further blood sample was collected on completion of surveillance. During surveillance periods each subject was contacted weekly by telephone at a prearranged time. Each volunteer was asked questions from a questionnaire about whether an acute upper respiratory tract infection had occurred during the previous week. When illness was reported a record was made of the date of onset and the presence or absence of rhinorrhoea; thick nasal discharge; nasal stuffiness; sneezing, sore throat, hoarseness, gritty or watery eyes, neckache, faceache, headache, or earache; myalgia; dry cough; productive cough; sweating; rigors; feverishness; breathlessness at rest; wheeze; and pain or discomfort on breathing. We also ascertained the extent of incapacitation, use of over the counter drugs, and whether a doctor had been consulted, drugs had been prescribed, and the patient had been admitted to hospital.
Subjects with symptoms were seen at home as soon as possible after the onset of symptoms. Nose and throat swabs and an acute phase blood sample (10 ml) were collected during this visit; another 10 ml blood sample was collected during convalescence about 28 days later. Symptoms were converted into syndromes based on published criteria.16 The illness was considered to be lower respiratory if symptoms of productive cough, wheezy breathing, or pain on respiration were present, irrespective of other respiratory symptoms. It was considered to be an upper respiratory infection if coryza was present without lower respiratory symptoms. If sore throat or hoarseness was present without any of the above symptoms the illness was identified as laryngopharyngeal. Illnesses without any of the above symptoms but with only non-productive cough, earache, nasal stuffiness, or other symptoms were classified as other.
We studied 533 volunteers in total, 441 during the first winter and 439 during the second (table 1). The 257 men and 276 women were aged 63–90 (mean 72.6 (SD 5.7) years) and 60–90 (mean 71.8 (6.1) years) respectively on recruitment. More men than women (207 (81%) v 129 (47%); χ2 test, P<0.001) had a history of smoking, but men and women were comparable with respect to being in the Department of Health's designated high risk category for influenza vaccination19; hospital admission during the preceding five years; attendance at a hospital outpatient department during the preceding 12 months; proportions consulting their medical practitioner during the preceding 12 months; and the numbers vaccinated against influenza. The project was approved by the Leicestershire ethics committee, and signed informed consent was obtained from all volunteers.
Demographic details of volunteers. Values are proportions (percentages) of subjects
VIROLOGY
Nasal swabs were placed high in the anterior nares and throat swabs were passed firmly over the tonsils and pharynx. Swabs were immediately placed together in 2.5 ml of transport medium containing nutrient broth. They were transported to the laboratory on dry ice and stored at −70°C, usually within several hours of collection and always within 12 hours. Paired acute and convalescent serum samples were stored at −20°C and tested later by complement fixation tests for antibodies to adenovirus; influenza A and B; respiratory syncytial virus; parainfluenza viruses types 1, 2, and 3; Mycoplasma pneumoniae; and Chlamydia psittaci. Haemagglutination inhibition tests were also carried out for the identification of infections by influenza type A. A fourfold rise in antibody was taken as indicating infection. An enzyme linked immunosorbent assay (ELISA) that is not commercially available was used to detect rises in antibodies to coronaviruses 229E and OC43. Serum samples were tested at a dilution of 1:200, and a consistent ratio of >/=1.3 between absorbance values of convalescent and acute samples was taken as indicating recent infection.15
Rhinoviruses in nose and throat swabs were identified by using a semi-nested reverse transcriptase polymerase chain reaction incorporating a touchdown reaction cycle.15 18 Cultured rhinoviruses of several serotypes were used as positive controls, and additional controls included baseline samples and water or virus transport medium. The appearance of a 202 base pair amplification was taken to indicate rhinovirus infection.
FACTORS ASSOCIATED WITH LOWER RESPIRATORY COMPLICATIONS
Simple and multiple logistic regression were used to identify factors associated with lower respiratory complications of rhinovirus infection. Multiple logistic regression was used to estimate the probability of lower respiratory complications by calculating adjusted odds ratios for potentially important explanatory variables. Failure to take into account the occurrence of several rhinovirus infections in patients with more than one rhinovirus infection could skew the results by overrepresentation of people with the most frequent infections. Accordingly, we entered data relating to the first rhinovirus infection only into the model for subjects having more than one rhinovirus infection. The modelling strategy used was initially to fit a saturated model including age, sex, regular treatment for heart disease, respiratory illness, and chronic ill health falling within the Department of Health's designated high risk category for influenza vaccination,19 admission during the preceding five years, hospital outpatient visits during the previous year, medical practitioner consultations during the previous year, and previous and current smoking. Variables with the smallest contribution to the model were removed one at a time until only those remaining in the model contributed significantly.
Results
CLINICAL EPISODES
The volunteers completed 24 700 patient weeks of observation. A total of 706 episodes were identified in 384 (72%) subjects. Overall, 691 episodes were classed as respiratory syndromes—these occurred at a median rate of 1.2 episodes per annum (95% confidence interval 1.0 to 1.7); 15 episodes were not classified because symptoms were not recorded.
LABORATORY FINDINGS
Specimens were collected a median of four days after onset of symptoms (range 1–21 days) (fig 1) for 497 (72%) of the 691 classified episodes; 476 (96%) of the 497 were collected within eight days and 493 (99%) within 12 days. Missing specimens occurred when there were delays in reporting illness, notably during Christmas, New Year, and Easter and periods of travel.
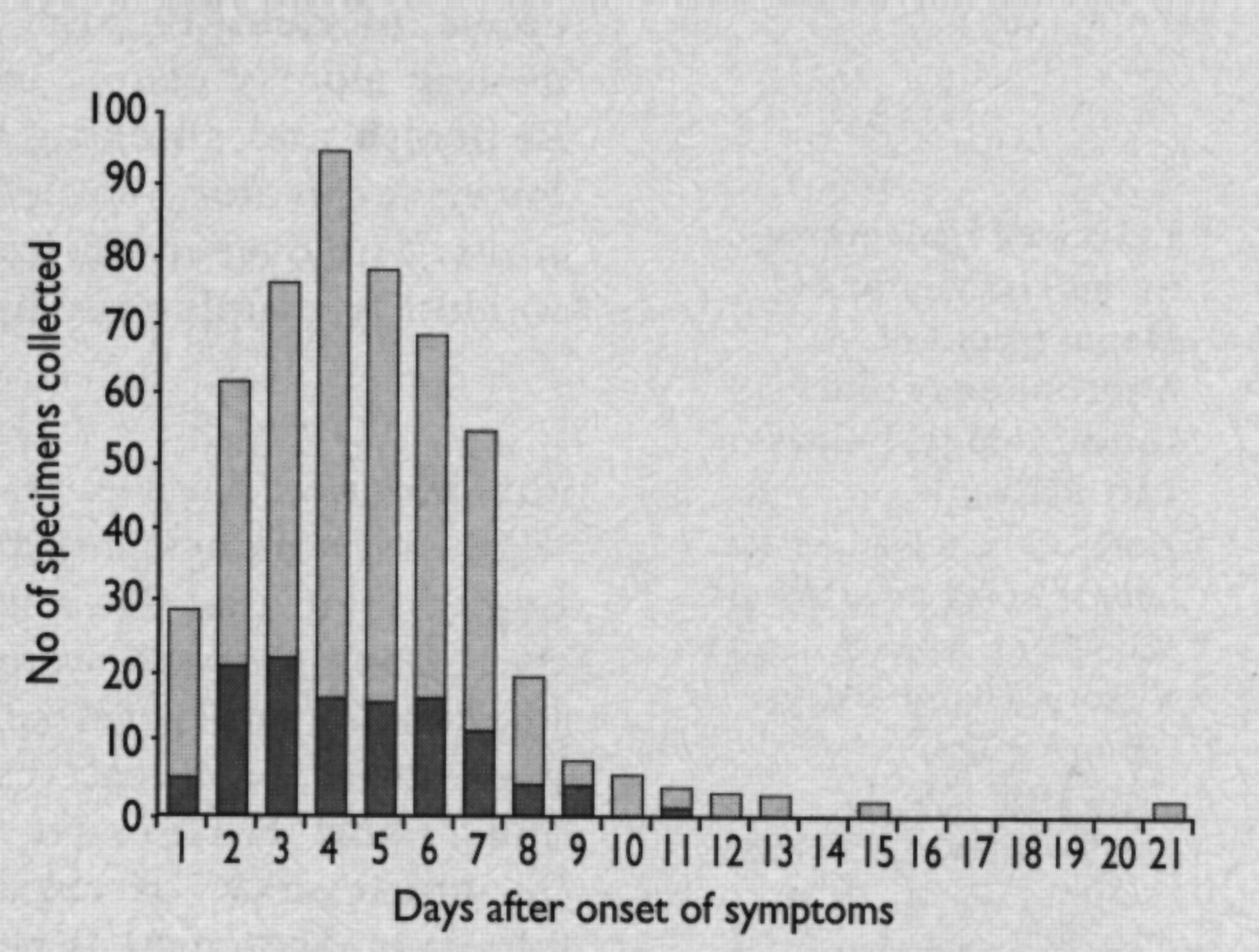
Time between onset of symptoms and collection of 497 nasopharyngeal specimens, the darker shading showing numbers positive for rhinovirus in polymerase chain reaction
{kind=link}
Infection with 231 pathogens was identified for 211 (43%) of the 497 episodes. Overall, 121 of the 231 pathogens were rhinoviruses (52%), 59 (28%) were coronaviruses, 22 were influenza A or B (9.5%), and 17 were respiratory syncytial viruses (7%). Rhinovirus reverse transcriptase polymerase chain reaction was positive for 121 of the 211 (57%) episodes with viral identifications and for 119 (24%) of the 497 illnesses overall. The proportion of the 497 specimens (by day of collection) yielding a rhinovirus is shown in figure 1. Analysis did not show a significant decline in the detection rate for rhinoviruses during the first 14 days after onset of symptoms (χ2 for trend = 0.98), but rhinoviruses were not identified in specimens collected later than day 11. Two out of 77 (3%) baseline nasopharyngeal specimens—from a husband and wife—were positive for rhinovirus.
CHARACTERISTICS OF RHINOVIRUS ILLNESS
Rhinoviruses were identified as single pathogens during 107 episodes in 96 people. Two subjects had three rhinovirus infections and seven people had two. To avoid overrepresentation of rhinovirus infections in those with more than one infection we focused on the first or only infection in the 96 subjects. Sixty of the 96 subjects had lower respiratory tract syndromes, 26 upper respiratory infections, and 10 laryngopharyngeal infections. Most (63 (93%)) had upper respiratory symptoms, and more than half (56) had systemic features (table 2). The median duration of illness was 16 days overall (range 4–69 days); it was 13 days in the upper respiratory and laryngopharyngeal groups combined and 19 days in those with lower respiratory symptoms (Mann-Whitney U test, P = 0.008).
Symptoms of rhinovirus infection in 96 patients with positive results in polymerase chain reaction
Twelve (20%) of the 60 lower respiratory illnesses, two (20%) of the 10 laryngopharyngeal illnesses, and four (15%) of the 26 upper respiratory illnesses resulted in severe restriction of activity, defined as confinement to bed. Twenty five of the 96 people infected with rhinovirus were temporarily unable to cope with routine household activities. Forty one of the 96 infections resulted in medical consultations; there were 47 consultations for 60 lower respiratory illnesses, six for 10 laryngopharyngeal episodes, and five for 26 upper respiratory illnesses (χ2 = 26.6; P<0.001). Antibiotics were prescribed to 31 of the 41 (76%) people who consulted their general practitioner, and antibiotic prescription rates after medical consultations for the three illness categories were similar. However, antibiotics were prescribed less frequently for the upper respiratory syndromes (three out of 26) than for the laryngopharyngeal (four out of 10) and lower respiratory (24 out of 60) syndromes (χ2 test, P<0.05).
None of the rhinovirus infections resulted in hospital admission, but one woman died from chronic obstructive airways disease exacerbated by a rhinovirus infection. She had a history of unstable asthma and produced sputum four days after she developed a sore throat. Her condition deteriorated rapidly: she developed wheeze and was breathless at rest. She increased her use of inhaled bronchodilators. She saw her medical practitioner and took oral steroids and antibiotics, but her condition deteriorated and she died 19 days after the onset of the infection.
FACTORS ASSOCIATED WITH LOWER RESPIRATORY COMPLICATIONS
Simple regression analysis did not show an association between lower respiratory complications of rhinovirus infection and age, chronic heart disease, admission during the previous five years, hospital outpatient visits during the preceding year, general practitioner consultations during the preceding year, or previous smoking. However, associations were found with chronic lung disease, combined chronic medical conditions falling within the Department of Health's designated high risk category for influenza vaccination,19 and current smoking. Multiple logistic regression analysis showed that the estimated probability of lower respiratory complications in those with one or more chronic medical conditions was increased by 40% in comparison with the remainder (adjusted odds ratio 1.40 (95% confidence interval 1.17 to 1.68)). Among current smokers it was increased independently by 47% (adjusted odds ratio 1.47 (1.14 to 1.90)). In the next stage of the analysis the interaction between the Department of Health's high risk category for influenza vaccination and current smoking was assessed by addition of product terms. Adjustment of the model for an interaction between the high risk category and current smoking showed no significant effect.
Discussion
Although there have been several studies of respiratory viral illness in the general community, none has focused on elderly people living in the community, used modern sensitive methods of detecting rhinovirus infections, or examined the clinical outcome in detail. We identified rhinoviruses more often than the other pathogens combined; this finding underscores the major contribution of rhinoviruses to the overall frequency of acute respiratory infections in elderly people.
Peak shedding of rhinovirus, as detected in culture samples, typically occurs several days after inoculation of volunteers with the virus and then diminishes rapidly.20 21 Previously we found that the semi-nested reverse transcriptase polymerase chain reaction is about five times more sensitive than cell culture in detecting rhinoviruses from adults with respiratory tract infections.15 18 Despite the sensitivity of the polymerase chain reaction, the amount of rhinovirus isolated in cell cultures diminishes with increasing age of the subject,22 possibly reflecting residual immunity to previous infection. This coupled with inherent delays in obtaining nasopharyngeal specimens may explain why our overall virus identification rate (43%) was significantly lower than during a previous study of adults with asthma (57%).15 We therefore suspect that the contribution of rhinoviruses to morbidity in elderly people is greater than our results suggest.
The response rate of those invited to take part might also be a source of bias. Participants in our study may have been more health conscious than non-participants, and they may report symptoms and consult their general practitioner for minor respiratory complaints more readily. Indeed, comparatively few were current smokers, and the overall influenza immunisation rate in relation to the prevalence of chronic medical conditions was high.
MORBIDITY
Rhinovirus illness in young adults is generally a self limiting, benign illness characterised by rhinorrhoea, sneezing, sore throat, and nasal obstruction.8 These features were prominent in this study. In addition, severe restriction of activity, defined as being confined to bed, occurred in almost a fifth of those with rhinovirus illnesses, and more than a quarter of them were temporarily unable to cope with routine household activities. The median duration of illness was 16 days, which is more than twice the duration in working adults.8 Overall, about 43% of rhinovirus infections in this study resulted in medical consultations; there was more than one consultation for every two rhinovirus infections, and antibiotics were prescribed empirically to more than three quarters of all people consulting a doctor, irrespective of the clinical features.
An intriguing difference between rhinovirus illness in young and older adults is the evidently greater frequency of lower airway symptoms with aging. In young working adults in Charlottesville, Virginia, sputum production and chest pain were reported by about 10% of 139 people with rhinovirus infections.8 Using the same case definitions as ours, Monto et al reported lower respiratory illness in 5% of 39 rhinovirus infections in people aged 5 to 19 years and in 34% of 59 infections in those aged 20 to 39.16 In contrast, 60 (62%) of the 96 people infected with rhinovirus in our study had lower respiratory syndromes; this is virtually identical with rates of 65% in 17 people over 4016 and 66% in 33 residents of a long term care facility for war veterans.23
RISK FACTORS FOR LOWER RESPIRATORY ILLNESS
Our findings indicate that a substantial proportion of elderly people are at risk of lower respiratory complications from minor upper respiratory disease. Moreover, since there were almost six rhinovirus infections for every influenza infection, our data suggest that the overall burden of rhinoviruses in elderly people may approach that of influenza. Since little is known of the risk factors or immunopathological or pathophysiological mechanisms underlying lower respiratory events we used regression analysis to identify those at increased risk. Preliminary analyses showed associations between lower respiratory complications of rhinovirus infections and chronic lung disease, combined chronic medical conditions falling within the Department of Health's designated high risk category for influenza vaccination,19 and current smoking. We did not identify age as a risk factor, presumably because of underlying chronic ill health (58% prevalence) and the size of the cohort. We also failed to establish hospital admissions in the preceding five years, outpatient attendance, general practitioner consultations, and previous smoking as risk factors. However, multiple logistic regression analysis showed that the estimated probability of lower respiratory complications in those with chronic medical conditions targeted for influenza vaccination increased by 40% in comparison with the remainder and that the estimated probability of lower respiratory complications associated with smoking increased independently by 47%. Thus viruses other than influenza virus pose a risk to people with chronic ill health.
We found that the odds ratio for lower respiratory complications among current smokers was comparable with the odds ratio for chronic ill health. Smokers are at greater risk of developing colds than non-smokers because they are more likely both to develop infections and to develop illness after infection.24 Gwaltney et al observed cough to be more common and persist longer in smokers with rhinovirus infection, but sputum production in their working adult population was uncommon.8 A greater susceptibility of smokers to rhinovirus illness may be due to a decrease in ciliary activity, increased epithelial damage, altered mucous secretion, decreased production of immunoglobulins and interferon, decreased alveolar macrophage activity, or enhanced inflammation and mediator release.25 26 Irrespective of the mechanism, our findings provide a further public health message about the hazards of smoking. They also suggest that smoking should be evaluated as a risk factor for lower respiratory complications of influenza; conceivably smokers should be included as a target group for influenza vaccination, as in France.27
EFFECT ON LOWER AIRWAYS
Rhinovirus replication is substantially reduced at body temperature compared with the temperature of the upper airways, and whether rhinoviruses regularly infect lower airways is uncertain. Halperin et al isolated rhinovirus from lower respiratory secretions obtained at bronchoscopy but were unable to exclude the possibility of nasopharyngeal contamination.28 Colds and rhinoviruses commonly affect the function of small airways as seen by changes in frequency dependence of compliance,29 steady state carbon monoxide diffusing capacity,30 closing volume, and maximal expiratory flow rates,31 particularly in smokers. We and others have also implicated rhinoviruses and colds in substantial proportions of asthma exacerbations in adults and children.15 32 It is questionable whether the effects on pulmonary function are dependent on infection of the lower airways or are due to a generalised inflammatory response to a localised infection. Colds are not associated with a proliferation of bacteria in the nasal cavity and nasopharynx,33 and frequently occurring lower respiratory events in elderly people are unlikely to be due to bacterial superinfection.
MORTALITY
Previously we reported mortality of about 3% (six out of 179) from acute upper respiratory tract illnesses among the elderly people in residential care.34 Wald et al reported one death from rhinovirus infection among 33 (about 3%) veterans in a long term care facility,23 and in our study one (about 1%) rhinovirus infection was fatal. Mortality statistics in England and Wales are significantly associated with general practitioner consultation rates for colds and aggregated acute upper respiratory tract infections.35 36 We anticipate that increasing use of modern highly sensitive methods of detection will lead to a greater recognition of rhinoviruses as a cause of death in elderly people.
CONCLUSION
In summary, we found that rhinovirus infections among elderly people living in the community caused a high incidence of lower respiratory illness and were often associated with restriction of activity, consultating a doctor, and use of antibiotics. Lower respiratory illnesses were more common in people with underlying chronic medical conditions and current smokers. As there are no inexpensive safe antirhinovirus agents or vaccines, the study highlights the need to learn more about the pathogenesis of lower respiratory rhinovirus illness.
We thank the volunteers who participated in this study for their support.
Footnotes
-
Funding The study was supported by a grant from the British Lung Foundation.
-
Conflict of interest None.