Article Text

Abstract
Objective: To evaluate and identify potentially modifiable factors in children with problematic asthma by a nurse-led assessment and home visit.
Design: Observational cohort study.
Setting: A tertiary paediatric respiratory centre.
Patients: 71 children, aged 4.5–17.5 years, with problematic asthma currently under follow-up at a tertiary respiratory centre.
Interventions: A nurse-led hospital visit followed by a home visit.
Main outcome measures: Identification and attempted change of exacerbating factors so that further investigations and consideration of off-label, potentially toxic, asthma therapies were not necessary.
Results: Potentially modifiable factors were identified in 56 (79%) children. Many children had multiple causes for poor control. The most important were ongoing allergen exposure, 22 children (31%); passive or active smoking, 18 children (25%); medication issues including adherence, 34 children (48%); psychosocial factors, 42 families (59%). The home visit contributed valuable information to this assessment. At the home visit house dust mite avoidance measures were found to be inadequate in 84% of those sensitised; medications were not easily available for inspection or were out of date in 23%; 74% of psychology referrals were made after the home visit. In 39 children (55%) the factors identified and the interventions recommended meant that further escalation of treatment was avoided.
Conclusions: Nurse-led assessments including a home visit can help identify potentially modifiable factors for poorly controlled symptoms in children with problematic asthma.
Statistics from Altmetric.com
Most children with asthma have their symptoms controlled with low-dose inhaled corticosteroids (ICS). However, approximately 5–10% of asthmatic children have ongoing symptoms and/or severe exacerbations despite treatment with conventional therapy, including high-dose ICS, long-acting β-2 agonists, and leucotriene receptor antagonists.1 2 These patients with problematic, difficult to manage asthma consume a disproportionate amount of resources.3 4 There can be many reasons for poor symptom control including wrong diagnosis, co-morbidities, poor adherence to treatment, psychosocial issues, allergen exposure and active and passive smoking. We have proposed the subdivision of “problematic” asthma into “difficult asthma”, which becomes easier to treat when basic management, for example adherence to therapy, is optimised, and “severe, therapy-resistant asthma”, in which the children remain symptomatic despite appropriately administered conventional management.5
Secondary and tertiary care assessments of these children and their families usually take place in the hospital setting. Although useful information can be gained during these meetings, we suspected it was often incomplete due to time constraints6 and reluctance to disclose sensitive information to a doctor.7 Visiting families at home has been shown to be of benefit in helping patients with asthma develop self-management plans,8 9 to minimise exposure to home environmental asthma triggers10 11 and to provide psychological support.12 However, little is known of how much a home visit contributes to the assessment of children with problematic asthma. We have evaluated the outcomes of nurse-led assessments as part of the difficult asthma protocol, in particular the home visit to assess the information gained and effect on outcome.
Methods
Eligible subjects were school-aged children with physician-diagnosed asthma who were currently being seen by a respiratory paediatrician at the Royal Brompton Hospital (a tertiary centre). They had persistent symptoms (⩾3 days a week), or frequent exacerbations (once a month or more) despite treatment stage of at least four of the British Thoracic Society/Scottish Intercollegiate Guidelines Network guidelines.13
Our difficult asthma protocol was divided into three parts: stage one, the subject of this manuscript, which comprised a nurse-led hospital-based visit followed by the home visit; stage two, inpatient stay and further investigations including bronchoscopy; stage three, assessment of steroid responsiveness. At stage one, factors that were contributing to poor symptom control were identified and appropriate interventions recommended. Only those children for whom no potentially significant modifiable factors were identified or who still had ongoing symptoms despite the stage one interventions continued to stages two and three.
Nurse-led hospital-based assessment
The child and family attended the outpatient department for the initial assessment. Patient history, including triggers, environmental exposures, exacerbations in the past year and family history was recorded. Skin prick tests to common aeroallergens and foods were performed using standardised extracts and positive and negative controls (ALK-Abelló, Hørsholm, Denmark). A positive result was defined as a wheal size of 3 mm or greater in children aged 6 years or older or 2 mm or greater in children aged less than 6 years. Exposure to environmental tobacco smoke was measured using a high-sensitivity salivary cotinine quantitative enzyme immunoassay kit (Salimetrics, Pennsylvania, USA). Inhaler technique was reviewed and corrected if necessary. Permission was obtained to contact the family practitioner and ask for a list of prescriptions issued. A semistructured questionnaire was used to take a psychosocial history including questions on home life, school, asthma treatment and understanding of treatment. Spirometry was performed to measure first second forced expiratory volume and forced vital capacity. Bronchodilator reversibility was assessed following 1 mg salbutamol administered by a metered dose inhaler and spacer.14
Nurse-led home visit
The home was visited by the asthma nurse, with one or both parents present. The child was not usually present. If the child was also under the care of a local team the relevant paediatric community nurse was also invited to participate in the home visit. The home visit addressed four main areas: allergen exposure, smoking, adherence, psychosocial issues.
Allergen exposure
The home was checked for the presence of likely allergens, in particular house dust mite (HDM) and pets and whether any steps had been made to reduce exposure (including appropriate bedding, hot washing of bed linen, damp dusting and housing of pets outside).
Smoking
Evidence of smoking was noted, and in particular whether this took place inside or outside the home. Smoking was judged to have taken place in the home environment if there was a characteristic odour in the home, the presence of used ashtrays or actual smoking was observed.
Adherence
All medications prescribed to the child were checked and the location of the medicines and ease of access assessed. It was also noted if medicines were within their use-by-date and whether spares were available.
Psychosocial issues
A further opportunity to discuss any issues raised by the psychosocial questionnaire at the hospital visit was given and parents often found this a good opportunity to discuss any such issues at length. A referral to our clinical psychologist was made if appropriate and with the family’s agreement.
Assessment
The findings from stage one were discussed at a multidisciplinary team meeting. Individualised plans of treatment and interventions were recommended. In particular, it was determined whether the child was likely to have true severe, therapy-resistant asthma, with the need to proceed to further investigations including bronchoscopy.
Results
Between February 2005 and June 2008, 71 subjects were visited at home by one of two paediatric respiratory nurses as part of the difficult asthma protocol. The patient demographics and baseline measurements obtained during the nurse-led hospital-based assessment are shown in table 1.
Information obtained at hospital based visit: patient details, medication, spirometry, clinical status and prescription records
Allergen exposure within the home
Seventy-nine per cent of children were atopic (at least one positive skin prick test). The results of skin prick tests, carried out during the hospital-based visit are shown in fig 1. At the time of the home visit it was found that of the 31 children who were sensitised to HDM, five (16%) used reasonable HDM control measures (appropriate bedding, hot washing of bed linen, damp dusting), 15 (48%) were found to have only some measures in place and 11 (36%) none. Thirty pet owners were visited, of whom 17 (57%) were sensitised to their own pet. At the home visit it was found that 15 (88%) of those sensitised had not implemented any pet avoidance measures such as the housing of animals outside. Following the assessment it was felt that the presence of allergens in the home was contributing to ongoing symptoms in 22 cases (31%).
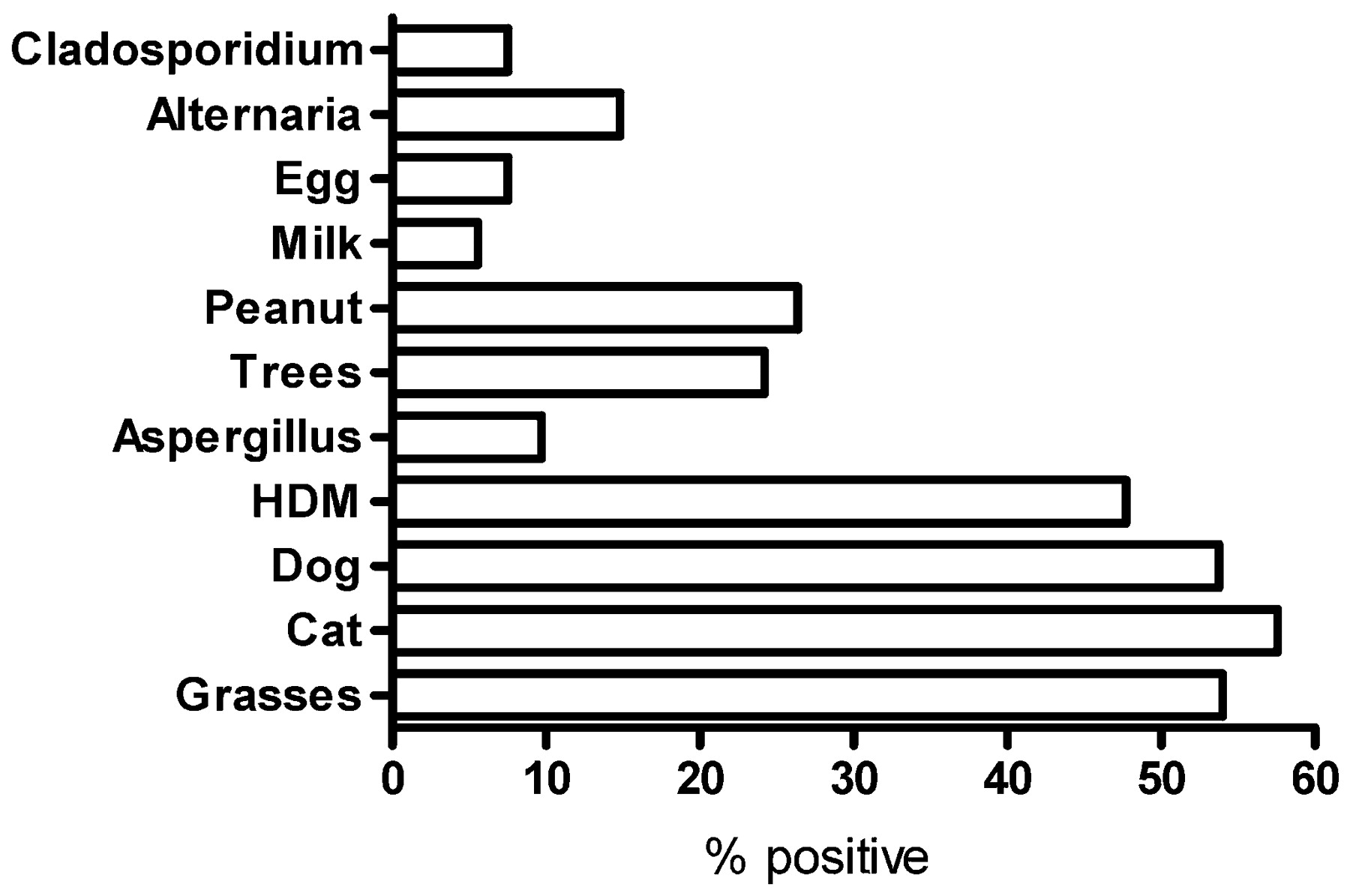
Result of skin prick tests to common aeroallergens and foods. A positive response was defined as a wheal 3 mm or greater in children 6 years of age or older and 2 mm or greater in children under 6 years. Results are expressed as the percentage positive of those tested. HDM, house dust mite.
Smoking
Twenty-three parents reported that they were smokers and two subjects admitted to active smoking. Salivary cotinine was measured in 39 children (26 non-smokers and 13 passive or active smokers). The median (range) cotinine levels were significantly higher in the passive/active smokers compared with non-smokers: 0.1 μg/l (0.01–3.5) versus 1.1 μg/l (0.3–16.1) p<0.001. The two active smokers had salivary cotinine levels of 16.1 μg/l and 4.5 μg/l. At the home visit no unreported parental smoking was found. Among those who smoked, indoor smoking was detected in eight. Smoking cessation advice was given to all parents.
Adherence to treatment
The data from prescription records are shown in table 1. At the time of the home visit complete medications were not easily available for inspection in 13 homes (18%). In eight homes medications were found to be past their use-by-date. Fifty-five families (77%) had a complete set of medications within their use-by-date available at the time of the home visit.
Following the hospital-based assessment 44 children (62%) were assessed as having a good inhaler technique, 13 were average and six had a poor technique. Eleven children were judged to have been prescribed inappropriate inhaler devices, most commonly children still using a mask with a spacer, using a metered dose inhaler without a spacer or unable to use a breath-actuated device.
Medication issues including adherence, unsuitable device and poor technique were felt to contribute to poor symptom control in 34 children (48%).
Psychosocial factors
Psychosocial problems were identified in 42 families (59%). Factors identified are shown in table 2. A total of 39 families (55%) was referred for further psychological evaluation and support. Twenty-nine (74%) of these referrals were made only after further information had been elicited at the time of the home visit. Twenty-eight children (39%) were assessed to have psychosocial factors as a major component of their asthma morbidity, either as a direct cause of their symptoms or as a consequence of their asthma.
Psychosocial factors identified.
Outcome
Fifty-six children (79%) were judged to have potentially modifiable factors contributing to their poor asthma control (fig 2). The interventions recommended as a result of the stage one visit (combined nurse-led hospital and home visits) are shown in fig 3. Following the stage one assessment, of the 71 evaluated only 32 (45%) continued to fulfil the criteria for severe asthma and went on to have further assessment including bronchoscopy. For those who had only stage one assessment further investigations were not necessary either because of improved symptom control as a consequence of the recommended interventions or because the underlying cause, such as very poor adherence, meant that further investigations and escalation of treatment would not be the most appropriate strategies.

Causal factors. More than one factor could be ascribed per child.

{kind=link}
{kind=link}
{kind=link}
Interventions recommended following the stage one assessment. More than one intervention could be recommended for each child.
Discussion
We report that 79% of a group of children, with ongoing poorly controlled asthma despite being prescribed high doses of conventional therapy, had potentially modifiable causes for their symptoms. These were children with prolonged asthma symptoms (mean 9.8 years), most of whom had been under long-term follow-up in secondary and tertiary care and were being considered for treatments beyond the recommendations of most asthma guidelines. In 55% the contributing factors that were identified and the interventions recommended meant that further evaluation, including an inpatient stay and bronchoscopy and escalation of drug therapy, were not needed.
The importance of the home environment and the assessment of adherence based on home visit data has previously been reported;15 however, this is the first study to attempt to quantify the contribution that the home visit makes to the assessment of the child with problematic asthma. We have identified key areas in which vital details were obtained at the home visit that complemented or were in addition to the hospital-based visit and influenced the evaluation and subsequent management of these children.
Allergen exposure
Most children who were sensitised to HDM and pets had previously been given allergen avoidance advice. At the home visit it was found that in most cases steps taken to minimise allergen exposure were suboptimal. The role of allergen avoidance in the management of asthma is controversial. It has been suggested that HDM avoidance is of no value whatever.16 17 However, many of the studies cited did not actually achieve a reduction in HDM levels, yet this is taken as evidence by some that a reduction of allergen load is not beneficial. Furthermore, there are no data in children with really severe asthma. Many children are multiply sensitised and studies that have targeted multiple allergens have been shown to be of benefit10 and this is the approach we have taken. It has been shown that asthma exacerbations are most likely in children who are exposed to high levels of allergen, are sensitised to that allergen and have a viral infection.18 Of these factors, only allergen load is susceptible to modification. Allergen avoidance measures can be expensive and the home visit gives an opportunity to identify the key areas for effective intervention.
The study would have been strengthened if we had actually been able to measure allergen levels in the home, especially after the institution of new allergen reduction measures.
Smoking
Twenty-three children in this study had parents who were smokers. Salivary cotinine levels were significantly higher in those who were passive/active smokers than those who were from non-smoking families. Although no unreported parental smoking was detected at the home visit, indoor smoking was detectable in a third of households. In the clinic setting most parents only reported smoking outdoors. Salivary cotinine levels did not differentiate parents who smoked outdoors and those who smoked in the home.
Adherence
Treatment issues were the most frequent contributory cause of poor symptom control. Non-adherence is a well recognised problem in children with asthma19 and an important cause of treatment failure.20 The difficult asthma protocol enables two dimensions of adherence to be assessed—prescriptions dispensed by the general practitioner, and the availability of in-date medications in the home, although neither is perfect. Merely collecting a prescription does not mean that the medication is actually taken. In some homes medications could not be found and others were located in inaccessible places. During the home visit, it was sometimes discovered that quite young children were inappropriately being left to take their medications with no direct supervision. This is in keeping with a recent study that found that by the age of 11 years, 50% of children with asthma were taking their ICS unsupervised.21 These findings are pointers to poor adherence, which help to build up a picture of the family’s approach and attitude to treatment and serve as a basis for useful discussion with the families.
Psychosocial factors
A wide range of psychosocial morbidity is seen in patients with asthma22 23 and this is reflected in our study. Although tools exist to assess quality of life24 25 we have found a semistructured interview a useful way to establish a dialogue with children and their families around sensitive issues. We have found that parents appear to feel more comfortable at home and are much more likely to disclose personal information during the home visit, particularly as the child was usually not present. This is reflected in the high number of psychology referrals made after the home visit compared with those made after the hospital visit (74% vs 26%).
What is already known on this topic
There are many causes for suboptimal asthma control.
A systematic assessment of children with problematic asthma is necessary in order to distinguish difficult asthma from severe therapy-resistant asthma.
What this study adds
A nurse-led home visit is an important part of the evaluation of problematic asthma and can help to identify potentially modifiable causes.
An effective treatment plan can help to avoid the need for further investigations and escalation of treatment.
Disadvantages
There are some constraints to carrying out home visits. Our catchment area is large and home visits have been carried out up to 60 miles from the hospital. A single visit can take up half a working day of an asthma nurse. We have not performed a health economic analysis of these visits, and this is a weakness of the study. Previously all children referred to us who fulfilled the criteria for problematic asthma were admitted for an inpatient stay and bronchoscopy. The current cost of this is £1053. Since implementing the nurse-led hospital and home-based assessments only 45% of those evaluated as part of the difficult asthma protocol went on to have an inpatient stay.
Home versus hospital assessment
It could be argued that this information could have been obtained as effectively as part of the hospital-based assessment. We acknowledge that some of the important data we have obtained were acquired before the home visit, as part of the hospital-based visit. Exposure to environmental tobacco smoke can be adequately assessed by means of salivary cotinine levels. An assessment of adherence using prescription records can be made without a home visit and psychology screening questionnaires can be administered in the outpatient setting. For some children the discovery that prescription uptake is poor and exposure to environmental tobacco smoke is high may obviate the need for a home visit. However, we feel the home visit affords us a unique insight and an opportunity to forge a closer relationship with our patients and their families; in many children information gained at the time of the home visit was invaluable in their overall assessment.
Further evaluation of outcome measures is needed to assess the long-term benefit of our approach. We have not shown objective evidence of benefit in this paper. However, it is difficult to believe that it is right to continue to escalate treatment and give steroid-sparing immunomodulatory drugs or expensive therapies such as omalizumab to a child who is not taking the prescribed ICS. Our approach led to the adoption of more conventional strategies in 39 of 71 children (55%), obviating the need for further investigations, expensive management strategies and potential toxicity.
In summary, we have evaluated a large cohort of children with problematic asthma, and through a nurse-led hospital and home visit have identified in many modifiable factors that were contributing to a lack of response to asthma treatment. We believe the home visit makes an important contribution to the assessment of the child with problematic asthma.
Acknowledgments
The authors would like to thank all the children and their families who participated in the difficult asthma protocol. We are grateful to Dr Donald Payne who helped devise the protocol, also to Drs Mark Rosenthal and Ian Balfour-Lynn who referred some of the children to the difficult asthma protocol and to Frances Beresford and Michèle Puckey who undertook the psychology assessments.
REFERENCES
Footnotes
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Atoms