Article Text

Abstract
Objective To investigate true adherence with a dry powder inhaler, the Turbuhaler (TBH), in children with asthma. True adherence was calculated by multiplying adherence to treatment with inhaler competence, that is correct use of the inhaler.
Patients and design In an 18-month study, children aged 5–10 years with asthma received twice daily budesonide via a TBH. Parents and children were trained in the correct use of the inhaler before the study started. For each inhalation, peak inspiratory flow through the TBH (PIFTBH) was recorded with an electronic pneumotachograph. The PIFTBH recordings were used to calculate true adherence for the first and last 45-day periods in the study by multiplying adherence in using the device (percentage of days with PIFTBH recordings) with inhaler competence (correct use of inhaler defined as PIFTBH values >40 l/min).
Main outcome measures True adherence, adherence, inhaler competence and PIFTBH.
Results 115 children were treated. The mean (morning and evening) true adherence during the first 45 days was 81.6% (range 78.1–86.4%) and during the last 45 days 57.4% (44.0–66.9%). Mean adherence was 86.0% and 59.3%, whereas mean inhaler competence was 94.7% and 96.2%, respectively. Thus the decline in true adherence was due to the decline in adherence. The largest decline in true adherence occurred in older children.
Conclusions True adherence with budesonide TBH treatment decreased significantly during the 18-month study due to a decrease in adherence. Inhaler competence with the correct use of the budesonide TBH was high and unchanged over the study period.
Statistics from Altmetric.com
Children with asthma are in general prescribed inhalers for the administration of inhaled corticosteroids (ICS) and β2-agonists.1 2 The inhalers depend on the patient's age, and are mainly pressurised metered dose inhalers (pMDI) with or without valved holding chambers, or dry powder inhalers (DPI).1 2 When using DPIs coordination is not required between actuation and inhalation as the drug release is driven by the patient's inspiratory effort. The inspiratory flow dependency of the drug release from DPIs is, however, dependent on internal device resistance. Drug release in DPIs with low internal resistance (powder in separate capsules or blisters) is less flow dependent than in moderate-to-high-resistance reservoir-type DPIs.3 Despite the greater flow dependency of drug release in high-resistance DPIs, the in vivo lung deposition correlating with clinical efficacy, has been shown to be less variable with this type of DPI than with pMDIs.4
What is already known on this topic
▶ Adherence to the prescribed dosing regimen with inhalers has been shown to deteriorate over time in long-term clinical trials of inhaled corticosteroids (ICS).
▶ Inhaler competence has not been recorded in long-term clinical studies of ICS.
▶ The combination of children's adherence to the prescribed dosing regimen and inhaler competence has not been previously reported.
What this study adds
▶ Recording of adherence to the prescribed dosing frequency is not sufficient for determination of the quality of clinical trials.
▶ Inhaler competence is as critical as adherence to the prescribed treatment regimen for inhaled drugs.
▶ Recording of true adherence (adherence×inhaler competence) should be considered in future clinical trials of inhaled drugs.
Lack of adherence to treatment for chronic diseases is a well-known problem.5 Maintenance treatment for asthma is no exception5 6 and as many as 50% of patients have been found to be non-adherent in clinical practice.7,–,9 Several factors may contribute to poor adherence with asthma treatment: the patient's attitude to the disease, the severity of the disease, a too complex treatment regimen, unwillingness to take medicines when symptoms are reduced or disappear, fear of side effects and inhalers too complicated to use.10 Lack of symptoms was, for example, the main reason for reported non-adherence with controller medication in a recently published large questionnaire-based study.11 Improved adherence could be achieved through simplified treatment regimens including number of inhalers and dosing frequency.5 6 The importance of frequently reviewed and reinforced partnership between patients and healthcare professionals has been highlighted as another possible solution to improved adherence.12 Patient feedback through the use of audiovisual reminders has also been suggested in order to improve adherence with inhaled therapy.13
When using inhaled asthma treatments, lack of inhaler competence – that is, incorrect use of the inhaler – could be as detrimental as lack of adherence to the prescribed treatment regimen. In a worst case scenario, the patient might not be able to inhale the intended amount of aerosol to the airways even if they have adhered to the prescribed treatment.14 When using inhalers, it is therefore logical to combine the two components – adherence to treatment and inhaler competence – in one outcome, true adherence.15 The analysis of true adherence is, however, dependent on new tools for daily assessment of inhaler competence in particular. In this study we have combined new technology for the assessment of adherence and inhaler competence with a high-resistance reservoir-type DPI, the budesonide Turbuhaler (TBH; AstraZeneca, Södertälje, Sweden) in an 18-month study of children with asthma. The effects on exacerbation and growth rates have been previously reported.16
Our hypothesis was that monitoring of treatment with a new technology would help to keep adherence at a high level throughout the study and that inhaler competence would not change over time due to the frequent monitoring.
Methods
A total of 176 children (107 boys), aged 5–10 years, with newly detected asthma participated in a randomised, double-blind, 18-month clinical study evaluating the efficacy and safety of budesonide inhaled via the TBH.16 All children randomised to treatment with budesonide received 400 μg twice daily for 1 month followed by 200 μg twice daily for 5 months. Thereafter, the children were randomised to placebo or budesonide 100 μg twice daily for 12 months. Exacerbations were treated with budesonide 400 μg twice daily for 2 weeks.16 Children (and parents) were trained in how to use the budesonide TBH based on the manufacturer's user guide including instructions on a deep and forceful inhalation.
The childrens' morning and evening peak expiratory flow (PEF) was recorded using a portable data storage spirometer (Vitalograph Data Storage Spirometer; Vitalograph, Maids Moreton, Buckingham, UK). The Data Storage Spirometer (DSS) was also used to record the peak inspiratory flow via the TBH (PIFTBH) each time a dose of budesonide was inhaled. The DSS consisted of a pneumotachograph and a computer (figure 1). Before use the DSS was calibrated with a standard volume syringe (variation±1%). After each exhalation (PEF) and inhalation (PIFTBH), values were shown on the DSS display, and both parents and children were informed verbally and in writing (informed consent) that adherence and inhaler competence were monitored through the use of the DSS. The importance of adherence and the correct use of the TBH were stressed at each clinic visit which occurred at approximately 6-week intervals. The date and time of day when the children performed the inhalations were recorded on the DSS, and this information was used to calculate adherence to the twice daily prescribed dosage regimen. The change in dosage of budesonide or switch to placebo was not relevant for the calculation of adherence as this was purely based on twice daily use of the TBH. Adherence was calculated as follows: total number of treatments recorded divided by the prescribed number of treatments×100.
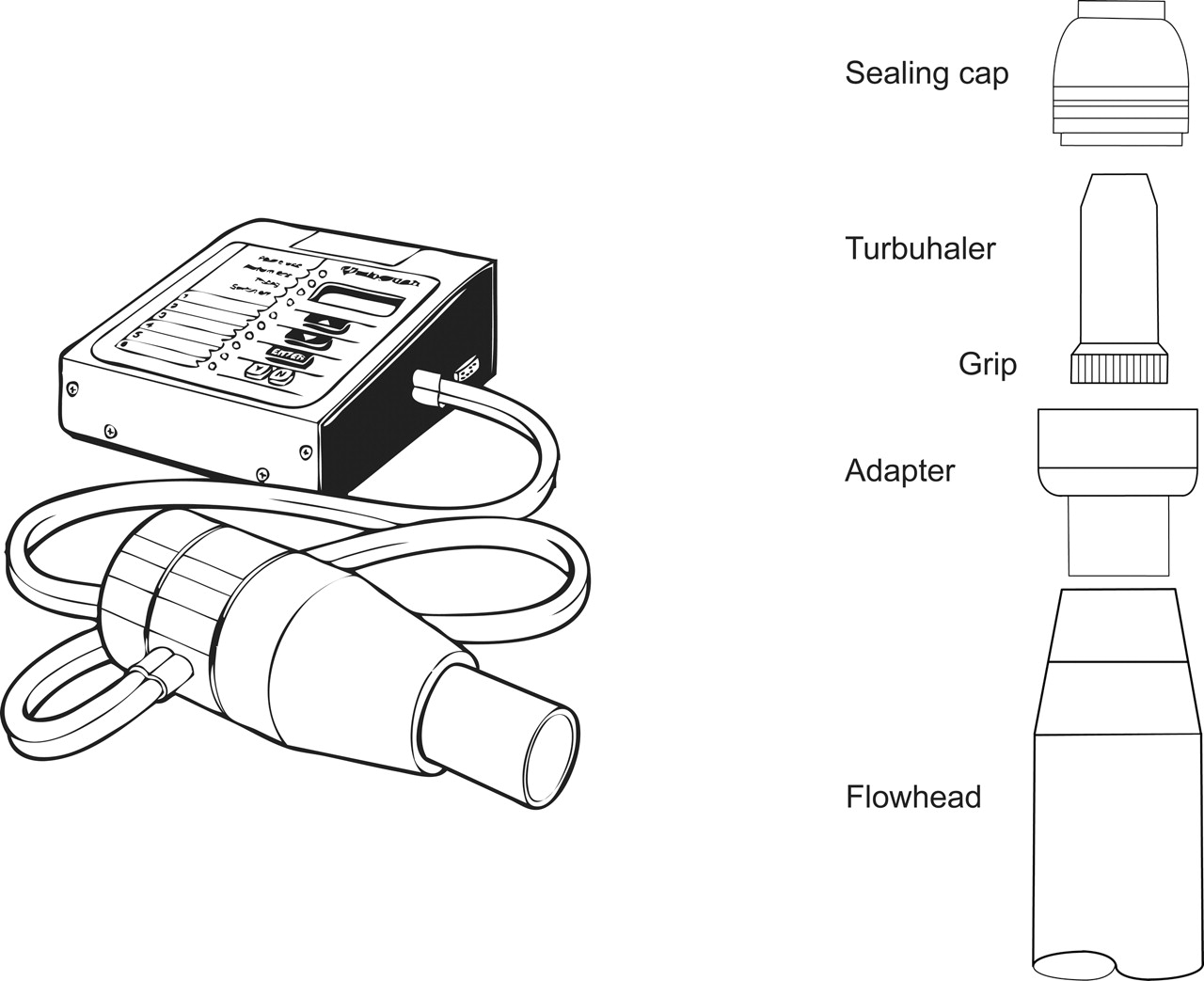
The Turbuhaler inhaler connected in series to the pneumotachograph (Vitalograph Data Storage Spirometer) for twice daily recordings of peak expiratory flow and peak inspiratory flow through the inhaler.
The budesonide TBH was connected in line with the pneumotachograph via a spacer (figure 1) designed to cover the inhaler apart from the mouthpiece. The spacer consisted of two parts, the adapter and the sealing cap. The coloured turning grip for dose selection of the inhaler fitted into the adaptor such that the patient could twist the turning grip by twisting the adaptor as far as it would go, and then twist it back. The patient could hear a ‘click’ when a new dose had been selected. The sealing cap of the spacer sealed tightly around the mouthpiece and against the adaptor. This meant that any flow generated by the patient during inhalation of a dose of drug through the TBH inhaler came through the inhaler without leakage around the inhaler. The PIFTBH value created by the patient was recorded in l/min and this information was used to calculate the patient's inhaler competence. The patient was considered competent with the inhaler if the PIFTBH values were >40 l/min. This cut-off point was chosen as clinical studies with the TBH in adults and children with asthma have shown no difference in bronchodilating effects after inhalation of a β2-agonist at PIFTBH levels of 30 l/min and 60 l/min.17,–,20 Furthermore, a study with radiolabelled budesonide in 6–16-year-old children with PIFTBH values in the range of 45–76 l/min showed satisfactory lung deposition even in the youngest children with the lowest PIFTBH values.21 We therefore decided to use >40 l/min and not >30 l/min as the cut-off point in this study. The inhaler competence was calculated as follows: number of inhalations with PIFTBH values >40 l/min divided by the total number of inhalations×100. PIFTBH values recorded at times of exacerbations were included in the analysis.
The true adherence was calculated by multiplying adherence with inhaler competence and expressed as per cent. Descriptive statistics were used. The results are given separately for boys and girls and for three age groups: children 5–6 years, 7–8 years and 9–10 years of age. Mean values were formed over periods of 45 days during the 18-month treatment period. The last value extended on computed period means was used to fill in missing values due to discontinuations from the study. Children completing the first 6-month phase and starting the second 12-month phase were included in the analyses. Data were subdivided into the first 45 days after randomisation and the last 45 days in the study counted from the last visit assessment. We report data for the first 45 and the last 45 days of the study.
The study was performed in accordance with the Declaration of Helsinki, and was approved by the local ethics committee. Written, informed consent was obtained from each patient's parent(s) or legal guardian and from the patient.
Results
The demographics and baseline characteristics of the children are shown in table 1.
Baseline characteristics of the treatment groups*
In the DSS, about 70% of the study days in the treatment period had morning registrations and 75% evening registrations of PEF. PEF recordings were available for nearly 90% of study days at the beginning of the study but for only approximately 50% at the end. Missing data due to malfunction of the DSS were reported on 2.5% of study days in the treatment period. The PEF values were age dependent with increasing values with increasing age (table 2). The percentage of study days with PEF recordings corresponded to the percentage of days with PIFTBH recordings. A statistically significant correlation was found between individual PIFTBH values and individual PEF values with a slope of 0.368 (95% CI 0.221 to 0.514). However, it was not possible to accurately predict the PIFTBH values from the PEF values in the individual child. The mean morning and evening PIFTBH values during the first and last 45 days of the 18-month study ranged between 31 and 212 l/min (table 2). All individual mean PIFTBH values except those of two children aged 6 and 8 years, were above 40 l/min. The mean values were slightly lower in the 5–6-year-old children than in the two older age groups (table 2).
Morning and evening PIFTBH and PEF values (l/min) in 115 children with asthma by age group
Adherence to treatment
The mean (morning and evening) adherence was 86.0% (range 79.1–91.2%) during the first 45 days and 59.3% (44.9–69.4%) during the last 45 days. The mean morning and evening adherence values during the first and last 45 days of the 18-month study by age group and gender are shown in table 3. The adherence was in general higher in the evening, and girls had slightly higher adherence values during the first 45 days of the study. During each 45-day period 10 350 inhalations (PIFTBH) should have been recorded (115×45×2). The results showed 8786 morning and 9098 evening inhalations were recorded during the first 45 days, and 6004 morning and 6618 evening inhalations were recorded during the last 45 days of the study. These numbers were used to calculate adherence to treatment.
Adherence (% days with PIFTBH recordings), inhaler competence (number of inhalations with PIFTBH >40 l/min) and true adherence (adherence multiplied with inhaler competence×100) as mean percentage (SD) by age group and sex
Adherence to the twice daily inhalations decreased from the initial 45 days of the study to the 45-day period at the end of the 18-month trial. In fact, when considering all the 45-day mean values, a gradual decrease from the first 45-day period to the last was apparent. We therefore believe that detailed reporting of a 45-day period at the beginning and another at the end of the study is representative of the study overall.
Inhaler competence
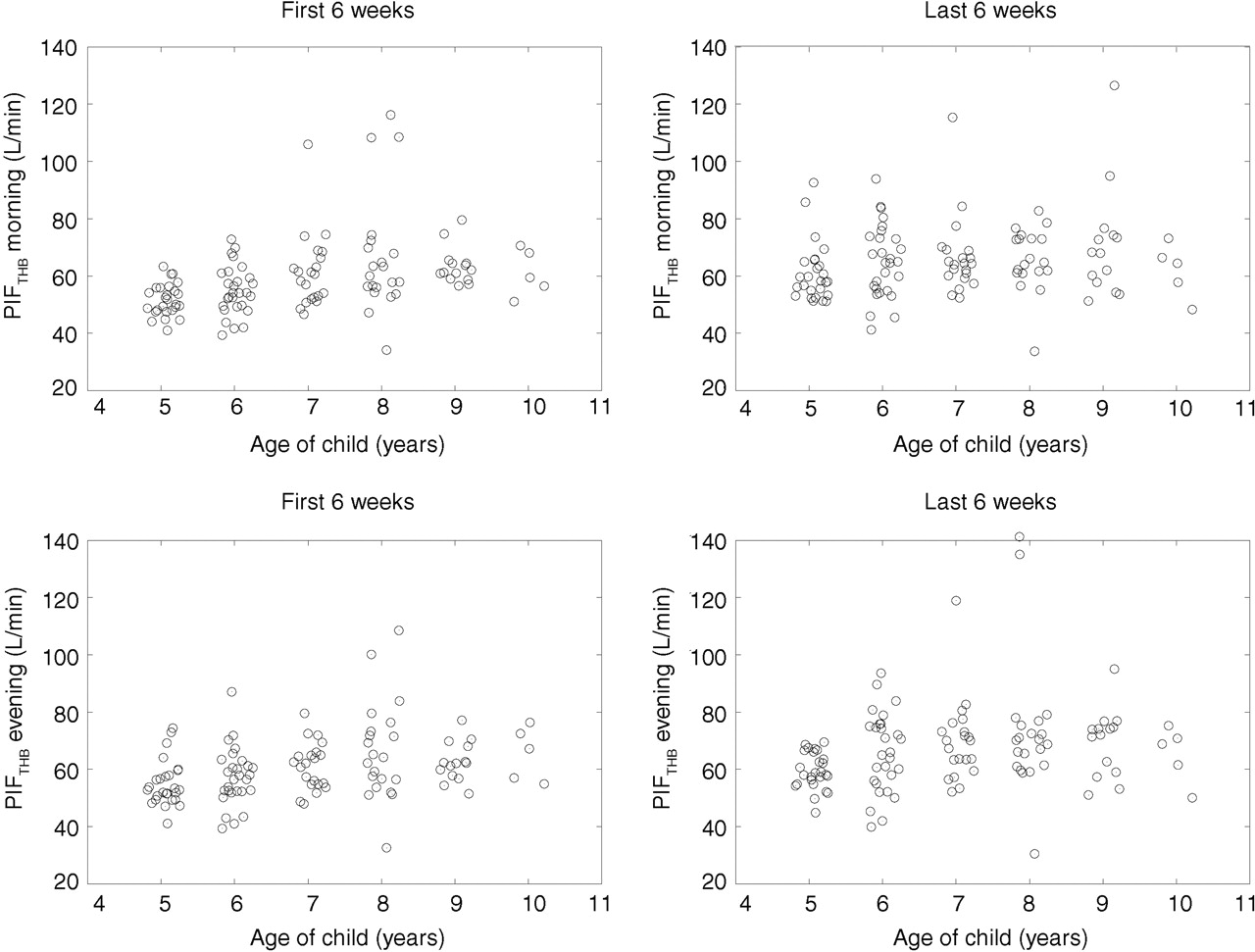
The mean (morning and evening) inhaler competence during the first 45 days was 94.7% (range 91.3–98.7%) and during the last 45 days 96.2% (94.8–98.0%). The mean morning and evening inhaler competence values during the first and last 45 days of the 18-month study by age group and gender are shown in table 3. Inhaler competence was ∼93% in the morning and ∼95% in the evening at the beginning of the study, and increased by approximately 2% towards the end of the study. There was no difference in inhaler competence between boys and girls. The individual mean PIFTBH values during the first and last 45 days of treatment have been plotted in figure 2 separately for morning and evening values and according to children's age at study entry. There were no differences in PIFTBH values between morning and evening recordings. During the first 45 days the morning mean individual PIFTBH values in the 5–6-year-old children ranged from 39 to 73 l/min. The corresponding values in the 7–8-year-old children ranged from 34 to 116 l/min, and in the 9–10-year-old children from 51 to 80 l/min. The mean PIFTBH values increased over time during the 18-month study (figure 3).

Individual mean peak inspiratory flow (PIF) through the Turbuhaler, by age at study entry, during the first and last 45-day periods of treatment.

{kind=link}
{kind=link}
{kind=link}
Development of mean peak inspiratory flow (PIF) through the Turbuhaler, by age, during the 18-month study (circles, 5–6-year-old children; squares, 7–8-year-old children and triangles, 9–10-year-old children).
True adherence
The mean (morning and evening) true adherence during the first 45 days was 81.6% (range 78.1–86.4%) and during the last 45 days 57.4% (44.0–66.9%) (table 3). The mean morning and evening true adherence values during the first and last 45 days of the 18-month study by age group and gender are shown in table 3. As true adherence was a product of both adherence and inhaler competence, any decrease in either component would have affected the true adherence values. The mean inhaler competence was surprisingly robust and ranged from 91.3% to 98.7% during both 45-day periods, whereas the mean adherence decreased over time from levels around 80–90% (first 45-day period) to levels around 50–60% (last 45-day period). Thus, due to poor adherence, the mean true adherence values (morning) dropped from around 80% at the beginning of the study to 64%, 51% and 44% by the end of the study in the 5–6-, 7–8- and 9–10-year-old children, respectively. The true adherence values were consistently higher in the evening throughout the study.
Discussion
The objective of this study was to perform an analysis of adherence to treatment and inhaler competence with the correct use of the TBH inhaler – and therefore true adherence – in an 18-month study in children with asthma using the budesonide TBH.16 The mean (morning and evening) true adherence decreased from a relatively high level (81.6%) during the early part of the study to a mediocre level at the end of the study (57.4%). As inhaler competence was excellent throughout the study, the gradual decrease in adherence over time was the main factor for the poor true adherence at the end of the study.
In clinical practice and in controlled clinical trials, emphasis is usually placed on measuring adherence to the prescribed dosing frequency. It is, however, obvious that inhaler competence is equally important.22,–,25 Regular intake of inhaled medication as prescribed (good adherence) is less effectual if inhaler competence is inadequate. This could result not only in undertreatment and poor disease control, but also in unnecessary costs and waste of medication.22–23 True adherence has been previously analysed in a 24-week study of parent's adherence to treatment and compliance (inhaler competence) with an Adaptive Aerosol Delivery System nebuliser used for nebulisation of budesonide to children with asthma.15 The results were surprisingly high with a mean adherence of 91.3%, a mean compliance of 90.4%, and hence a true adherence of 82.5%.15 True adherence has to the best of our knowledge not been analysed in children aged 5–10 years with asthma. As true adherence is a product of both adherence and inhaler competence, the definition of inhaler competence is of critical importance. We defined inhaler competence in the present study as the ‘correct’ use of the TBH, and correct use was defined as PIFTBH values >40 l/min, a cut-off that was based on clinical data.17,–,20 Based on this definition, inhaler competence was excellent during both 45-day periods. That all children except two had consistent 45-day mean PIFTBH values >40 l/min could mainly be attributed to the training in the use of the TBH inhaler before the study, and the supervision during the study.
It could, however, be argued that ‘inhaler competence’ should be based on inspiratory flow values and the overall handling of the inhaler.9 24 This includes loading each individual dose by turning the grip back and forth in an upright position (tolerance±45°), exhaling before a deep and forceful inhalation, not exhaling into the inhaler, inhaling through the inhaler and placing the protective cap on the inhaler after inhalation.25 The technology we used with the TBH inhaler covered by a spacer eliminated a number of these handling errors such as not inhaling through the inhaler and not replacing the cap. Based on the PIFTBH values the inhalations were sufficiently deep and forceful. We do not, however, know whether the children or their parents turned the grip of the TBH inhaler before every inhalation of study medication. The data on the clinical efficacy and especially the systemic activity of budesonide in the study seem to indicate that the patients inhaled the study medication.16 Nevertheless, a more complete check of inhaler competence with DPIs would in future studies require measurement of inspiratory flow and the transport of aerosol through the mouthpiece.
Adherence to treatment during the first 45 days of the study was relatively high but decreased towards the end of the study. Interestingly, the decrease in adherence was greatest in the two oldest age groups with decreases ranging from 33.5% (7–8 years, morning) to 27.2% (evening), and from 34.2% (9–10 years, morning) to 30.9% (evening). The adherence in the 5–6-year-old children decreased by only 19% (morning and evening), which was probably due to better supervision by their parents compared with the older children. Another possible explanation of the differences in change of adherence over time between the age groups could be differences in asthma control and/or lung function. However, an analysis of lung function data and asthma symptoms did not reveal differences between the age groups and therefore cannot explain the differences in adherence. Neither did the randomisation after 6 months to regular or periodic budesonide treatment explain any differences in adherence. Interestingly, adherence was higher during evenings at the end of the study. This might be of importance when considering a once daily approach to treatments with ICS. If the treatment is planned as once daily, then prescribing evening treatment may be beneficial as the chances that the patient would take the medication might be higher. Nevertheless, adherence to treatment was far from good at the end of the study, which is in agreement with previous observations.24 26 Solutions to problems with adherence in children with asthma vary and most families will benefit from concrete behavioural advice on establishing regular medication routines such as schedules for refills, reminders, or linking medication use to existing daily routines.11 24
This study highlights the importance of recording both adherence to treatment and inhaler competence, and hence true adherence in clinical studies. As true adherence seems to lessen over time, synchronous data analysis could be used to detect the decrease. This would be especially important in modern adaptive clinical trials. This study also shows the value of age stratified analysis of true adherence data. Through this analysis it was shown that the younger children – possibly due to closer supervision by parents – maintained a better true adherence level than older children. Assuming that the present results are relevant to the majority of patients using inhalers, it is obvious that all efforts should be taken to encourage children to keep true adherence with medication at a high level.
Acknowledgments
The authors wish to thank the children and their families for their excellent compliance during this long-term study. We also acknowledge the valuable contribution of Tuula Koljonen, RN, and Leena Ingelin-Kuortti, RN, study nurses, and Eeva Kiiskilä and Eva Holtås, study monitors.
References
Footnotes
-
Funding The study was sponsored by the Helsinki University Central Hospital (grant TYH 2303) and AstraZeneca, Lund, Sweden. This study was performed at the Department of Allergy at Helsinki University Hospital.
-
Competing interests T Bengtsson is an employee of AstraZeneca.
-
Ethics approval This study was conducted with the approval of the Helsinki University Hospital ethics committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.