Article Text

Abstract
Background: The incidence of childhood empyema, a complication of pneumonia, is increasing, and the underlying mechanisms are not understood. Whether a rise in pneumonia incidence could account for the increase in empyema remains to be seen.
Objective: To report trends for empyema admissions in the context of pneumonia and croup admissions in Scottish children over a 25-year period to 2005.
Design: Whole-population study with retrospective analysis using diagnosis codes (International classification of diseases, 9th and 10th revisions).
Setting: All non-obstetric and non-psychiatric hospitals in Scotland.
Participants: Patients <15 years admitted with a diagnosis of empyema, pneumonia or croup (the latter included for reference) between 1 January 1981 and 31 December 2005.
Results: There were 217 admissions for empyema in children (76 1–4-year olds), 24 312 admissions for pneumonia (11 299 1–4-year olds), and 31 120 (20 332 1–4-year olds) for croup. Empyema admissions increased after 1998 from <10 per million children per annum to reach a peak of 37 per million in 2005. In the 1–4-year age group, empyema admissions rose in the late 1990s and 2000s from an average of 6.5 per million per year between 1981 and 1998 to 66 per million in 2005. Overall annual admission rates for pneumonia remained unchanged in most age groups. However, among 1–4-year olds, admissions rose steadily by an average of 50 per million per year between 1981 and 2005. Admission rates for croup in Scottish children (<15 years) remained stable over the preceding 25 years.
Conclusions: This whole-population study shows that the incidence of childhood empyema has risen since 1998 and continues to rise independently of pneumonia. Croup admissions remained stable, suggesting that changes in coding or admission policies are not likely to explain the observed trends. The observations suggest that the rise in empyema is not related to an increase in pneumonia. Changes in bacterial pathogenicity and/or host susceptibility may be important.
Statistics from Altmetric.com
Empyema thoracis or pyothorax is a relatively uncommon but serious complication of pneumonia. The incidence of empyema in childhood is reported to be increasing in the UK and North America.1–6 In an analysis of 1349 admissions for empyema in childhood between April 1995 and March 2003 in England, the highest increase in incidence was observed in the 1–4-year age group, with a rising trend in admission rates seen in all children (0–14 years).4
Reasons for this increase are not fully understood, but may include an increase in pneumonia incidence among the paediatric population. The peak incidence of pneumonia in childhood is in those under 5 years of age,7 and a rise in pneumonia may plausibly account for the reported rise in empyema. A small rise in incidence of non-viral pneumonias in the USA has been reported but not thought to explain the larger increase in empyema incidence.8 In this study, we aimed to report longitudinal trends in incidence of childhood empyema and pneumonia in Scotland over a 25-year period. To ensure that any observed trends were not due to underlying changes in coding or admissions for all paediatric respiratory disease, we also report longitudinal trends for admissions for viral croup, a condition for which the incidence is thought not to have changed in the past 25 years. Our hypothesis was that an increase in empyema will be associated with a commensurate increase in pneumonia.
METHODS
All children admitted to hospitals in Scotland with empyema, pneumonia and croup were identified using International classification of diseases 9th and 10th revisions (ICD-9 and ICD-10) coding. Pneumonia is coded with ICD-9 codes 480–486 and ICD-10 codes J12–18. Empyema is coded ICD-9 510.0 (empyema with fistula) and 510.9 (empyema without fistula) and ICD-10 J86.9. Croup is coded ICD-9 464.4 and 466.0 and ICD-10 codes J05.0 and J20.9. Data were provided by the Scottish Information Services Division Offices in Edinburgh. The period of interest was 1 January 1981 to 31 December 2005. Only patients of 14 years and under (ie, <15 years) were included. Data were divided by age (<1 year, 1–4 years, 5–9 years and 10–14 years). These groupings were used to allow comparison with previous studies.4
Admissions were converted into rates (per million children) using population data from the Scottish General Register Office.9 Linear regression analysis was undertaken using SPSS V14.0 (SPSS Inc, Chicago, Illinois, USA) to establish trends of admission rates and whether observed changes over time were significant.
RESULTS
Study subjects
There were 24 312 children admitted with a diagnosis of pneumonia, and the mean rate of admissions per year was 1019 per million children aged 0–14 (range 714–1363). There were 217 children admitted with empyema, and the mean rate of admissions per year was 9.3 (range 2–37) over the 25-year period. There were 31 120 admissions for croup, with a mean rate per million of 1244.8 (range 793–1667). Table 1 shows that a high proportion of pneumonia (69.2%), empyema (49.8%) and croup (85.3%) admissions were for the <5-year age group.
Trends in pneumonia admissions
There was an increase in the overall rate of pneumonia admissions over the period studied (p<0.001, r2 = 0.47). However, this rise mainly reflected an increase in admissions in the 1–4-year age group by an average of 50 per million per year (p<0.001, r2 = 0.69). The rates in other age groups remained fairly constant over the study period (fig 1).

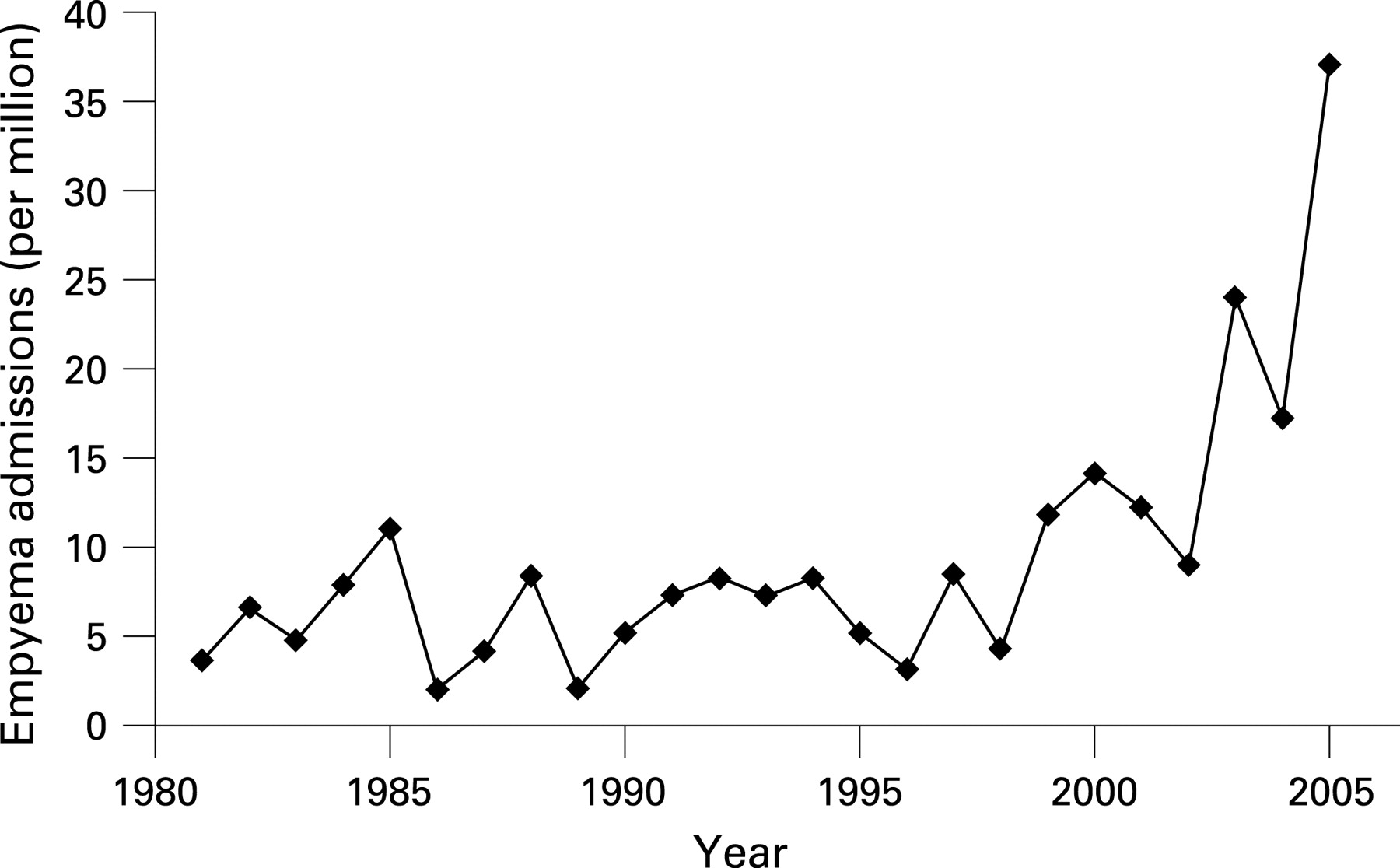
Trends in empyema admissions
The admission rate was stable over the period 1981–1998 (r2 = 0.002, p = 0.86). However, there was a linear increase in admissions for empyema from 1998 to 2005 (p = 0.015. r2 = 0.65) (fig 2). The highest average annual increase was in the 1–4-year age group (8.3 admissions per million per year), but there was also an increasing trend in the 5–9-year and 10–14-year age groups (average annual increases of 5.5 and 2.3 per million, respectively). Breakdown of cases by age grouping resulted in very small groups, therefore we do not show individual age group trends in graphical form (eg, range of 0–3 admissions per million per year for the <1-year age group over the past 25 years).
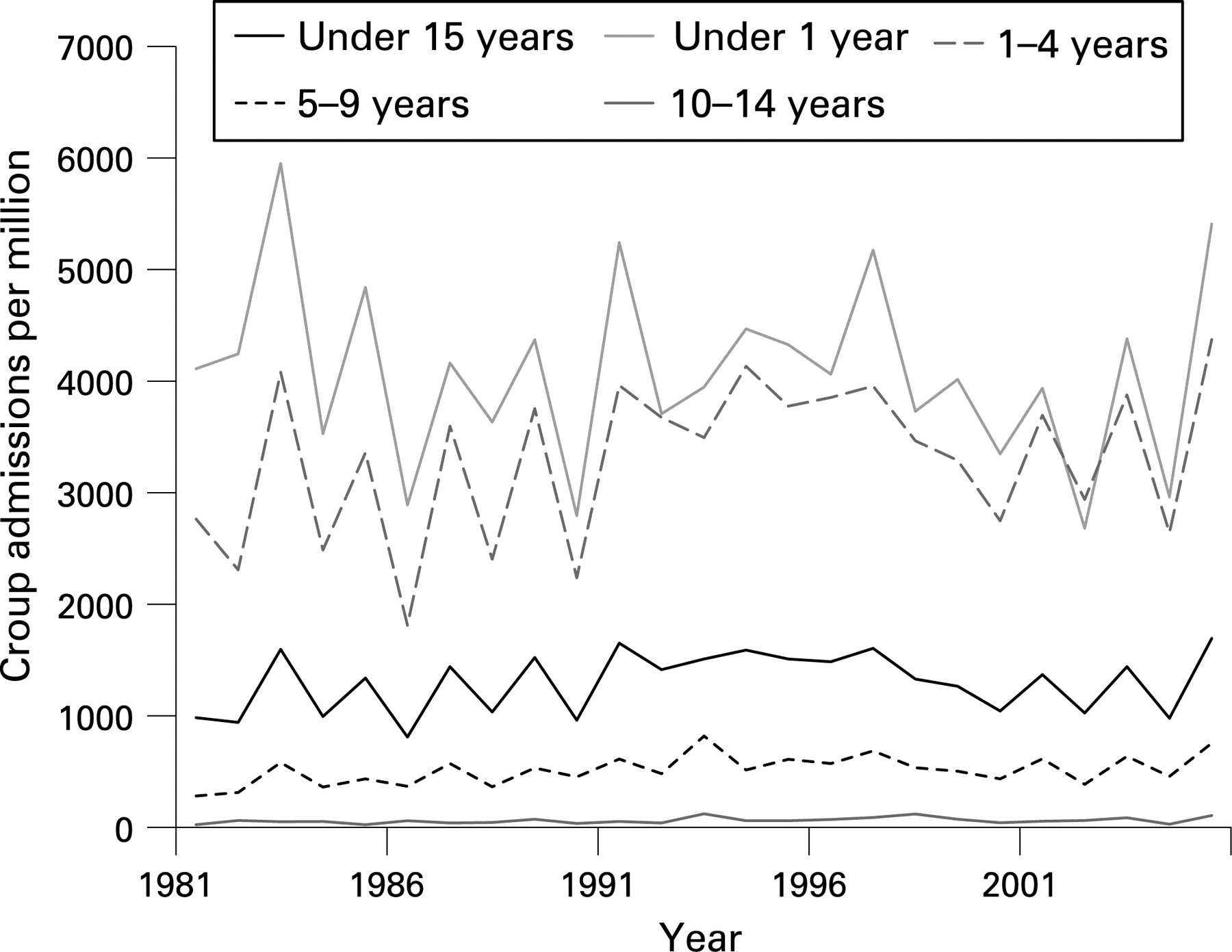
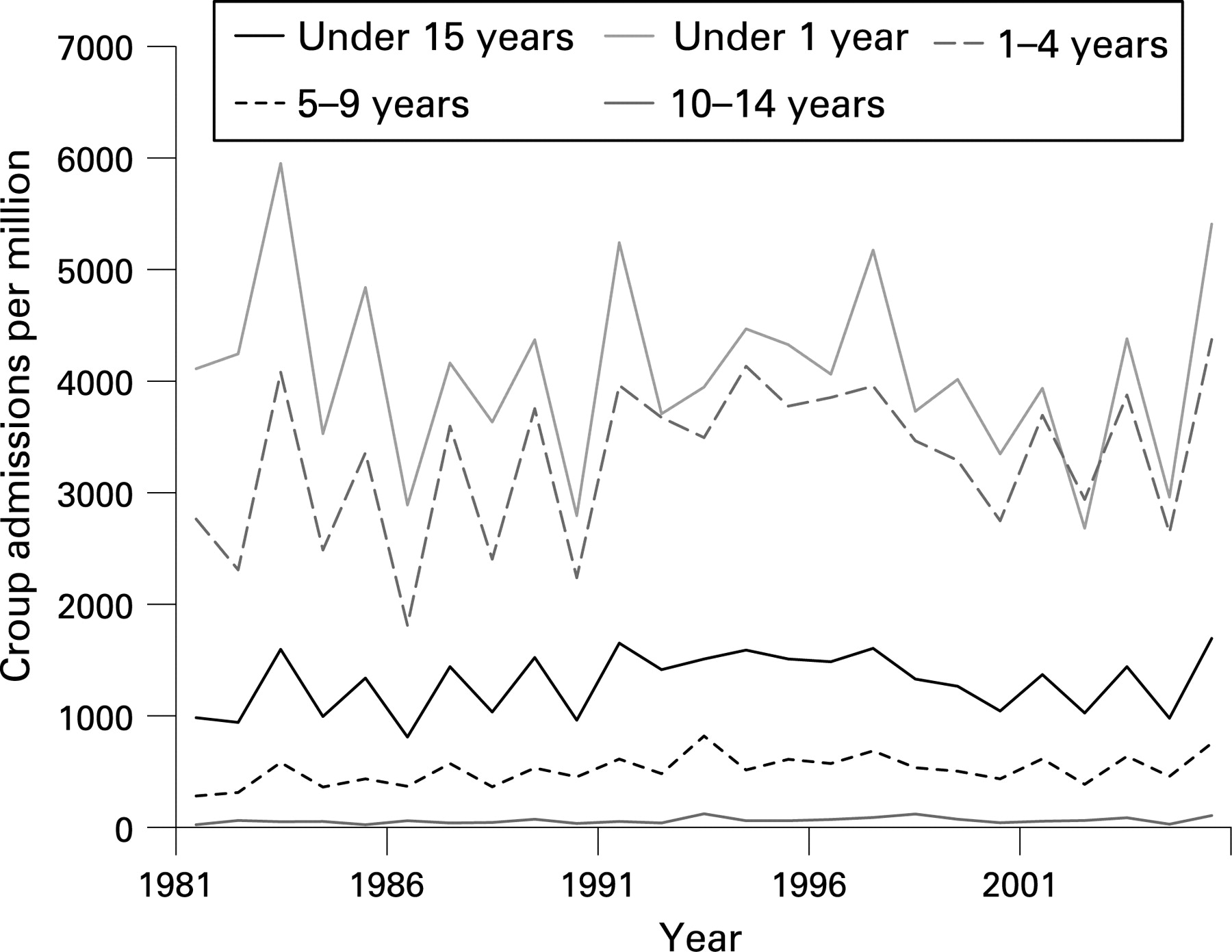
Trends in croup admissions
Over the past 25 years, the admission rates for croup have remained relatively stable in all children (fig 3) (r2 = 0.060, p = 0.237). However, a small but significant linear increase was observed in the 5–9-year (r2 = 0.227, p = 0.016) and 10–14-year age groups (r2 = 0.151, p = 0.04) over the whole 25-year period.
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
This study sought to place trends over a 25-year period for paediatric empyema admissions in the context of pneumonia admissions. The first finding was that the incidence of childhood empyema has risen recently and continues to rise, and this is consistent with previous reports. The second, and novel, finding was that, although pneumonia admissions were relatively constant in most age groups over the period of interest, a gradual increase in pneumonia in the under fives was detected, but this began ∼10 years before the increase in empyema. These findings suggest that the current “epidemic” of empyema in children is not due to an increased incidence of pneumonia.
Croup was included in this study as a reference condition to give assurance that the increase in empyema was not explained by an overall rise in all respiratory infections in children, and the rise in empyema was found to be independent of croup. A small but statistically significant increase in croup admissions was observed in the 5–9-year and 10–14-year age groups, but did not correspond to the increase in empyema admissions since 1998.
This study is the first to look at both empyema and pneumonia admissions in a paediatric population and also has the longest period of data collection. Although previous studies have identified an increase in empyema admissions in the UK, we can show that this phenomenon is a recent occurrence. Although we have observed increasing trends in absolute numbers of admissions for empyema, the general paediatric population is actually declining in Scotland. In 1981 there were 1 100 000 children under 15 years living in Scotland, and, by 2005, this had decreased to 865 000. There has been a slow decline in birth rates over this time.9 This fall in population may have led to an underestimate of the true incidence of empyema, but our analysis adjusted for this.
What is already known on this topic
Empyema incidence in children has increased in recent years.
Reasons for this increase remain unclear at present.
What this study adds
This increase in childhood empyema is not related to a general increase in childhood pneumonia.
In reporting trends for the past 25 years, we can show that the increase in empyema admissions is a recent phenomenon.
Admission coding trends for childhood empyema have previously been described in England. Gupta and Crowley4 reported an increase from 14 cases per million in 1995/6 to 26 per million in 2002/3. These figures are similar to our results, in which we saw a rise from five to 25 cases/million over the same period (fig 2). In a separate study from north-east England, where the population of children is ∼800 000, Eastham and colleagues3 reported an increase in new patient referrals with empyema and parapneumonic effusion from six to over 16 between 1997 and 2001, approximating to 7.5 and 20 cases per million, respectively. The incidence of empyema reported in the present study is consistent with data from England and provides further evidence that empyema is an emerging problem among British children.
As with other publications,4 these results are entirely reliant on accurate ICD coding undertaken over the last 25 years. Individual cases were not analysed and thus coding errors may have occurred. It is, however, unlikely that the shifts in admission rates as detailed in this study are simply due to coding errors. The inclusion of a reference condition such as croup shows that the trends do not simply reflect an overall increase in admissions for children with respiratory disease. Moreover, the results are unlikely to reflect changes in coding practices over the 25-year period. In addition, the unit measured was “number of admissions”; thus one patient with multiple hospital admissions could theoretically skew the data, although repeated admissions for empyema are relatively uncommon.
In summary, our data extend previous published results suggesting that empyema incidence is increasing by showing that empyema rates do not appear to be related to a general increase in all types of pneumonia. Changes in the antibiotic-prescribing policies of general and hospital practitioners and/or changes in virulence of bacteria (most commonly Streptococcus pneumoniae) may have led to the observed increase in empyema. Further research is needed to establish reasons for this increase in empyema, a serious complication of pneumonia. An enhanced surveillance programme for childhood empyema in the UK is underway (funded by the Health Protection Agency), which may answer some important questions.
Footnotes
Competing interests: None.
Linked Articles
- Atoms