Article Text

Abstract
AIM To investigate bone mineral status in patients with cystic fibrosis (CF).
PATIENTS AND METHODS Whole body bone mineral content (BMC), projected bone area, and bone mineral density (BMD) were determined by dual energy x ray absorptiometry in 134 patients with CF and compared with 396 healthy controls.
RESULTS In patients ⩽ 19 years of age, BMD for age was normal in boys and marginally reduced in girls, whereas BMC for age was significantly reduced in both sexes. Height for age and bone area for height were significantly reduced, indicating “short” and “narrow” bones, whereas BMC for bone area was increased, indicating increased size corrected BMC. In patients > 19 years of age, BMD and BMC for age were significantly reduced.
CONCLUSION Short and narrow bones were the main reasons for reduced BMC for age in patients ⩽ 19 years of age, indicating that treatment to prevent osteoporosis in younger patients should be directed at increasing bone size, whereas conventional treatment with calcium and vitamin D supplementation alone might not be as effective. Because of the significant decrease in BMD and BMC in adult patients, we fear that these patients may develop osteoporotic fractures prematurely.
- bone mineral content
- bone mineral density
- cystic fibrosis
Statistics from Altmetric.com
The mean survival age of patients with cystic fibrosis (CF) has increased dramatically to 30 years or more during the past few decades.1 The increased life span brings new disease complications and during the past years there have been several reports about demineralisation and osteoporosis in patients with CF. Studies have shown decreased bone mineral content (BMC) and bone mineral density (BMD) in children, adolescents, and adults with CF.2-6 However, most of these studies had relatively few participants and the control groups consisted of relatively few healthy individuals.
It is well known that patients with CF are growth retarded7-10 and, consequently, skeletal size may be decreased. BMD reflects both bone density and bone size and a reduced BMD can be the result of a reduction in real density and/or bone size.11 Two studies3 4 found decreased bone mineral apparent density (BMAD) in adult patients, a measure that reduces the influence of bone size, and concluded that the low BMD was not only caused by their smaller body size. However, weight, height, and body mass index (BMI) have been related to decreased bone mineralisation in several studies,2 3 5 12 and Salamoniet al found that BMC was normal in well nourished patients with CF compared with healthy controls matched for age, sex, and BMI.13 Therefore, we thought it important to correct for body size when evaluating the bone mineral content in the skeleton of patients with CF.
The aim of our study was to investigate bone mineral status in a large unselected population of patients with CF and to compare the patients with a large reference population of 396 local controls, who were examined using the same scanner. Furthermore, we investigated the bone mineral content corrected for skeletal size in children and adolescents with CF. We investigated this parameter (which has never been reported in patients with CF previously) to determine whether decreased skeletal size might be a possible explanation for decreased bone mineralisation in patients with CF.
Patients
The patients were recruited from the Danish CF centre at Rigshospitalet. Of 213 patients aged 6 years or more, 140 (66%) agreed to participate in a cross sectional study carried out from 1 June 1993 to 1 February 1995. Five patients were excluded because of: congenital adrenal hyperplasia, Noonan syndrome, severe thoracic scoliosis, glomerulonephritis resulting in kidney transplantation, and non-white origin. One patient dropped out. A total of 134 patients with CF remained in the study. The median age was 17.7 years (range, 6.1–45.4); 72 patients were female.
Of 134 patients, 103 (77%) were homozygous for ΔF508, 27 (20%) were compound heterozygous (ΔF508 and another mutation), and four (3%) patients had two non-ΔF508 mutations. This was representative of the Danish CF population.14 All patients were pancreatic insufficient and received daily treatment with pancreatic enzymes.
Seventy five patients did not want to participate in our study. They were slightly older than the study group, with a median age of 18.9 years (range, 6.2–45) v 17.7 years (range, 6.1–45) (p = 0.02), but height standard deviation score (SDS) and BMI SDS were equal (p = 0.51 and p = 0.97, respectively). There was no selection bias with respect to genotype and pancreatic insufficiency.
Methods
ANTHROPOMETRY
Standing height was measured to the nearest 0.1 cm using a stadiometer. Weight was measured on a digital electronic scale with a precision of 0.1 kg. Patients wore only underpants and a cotton T shirt when weighed. BMI was calculated as weight/height2 (kg/m2).
BONE MINERAL ASSESSMENT
Whole body BMC measured in gram hydroxyapatite, bone size expressed as anterior–posterior projected bone area measured in cm2, and BMD (BMC/bone area) were determined by dual energyx ray absorptiometry (DXA) using a Hologic 1000/W (Hologic Inc, Waltham, Massachusetts, USA). For analysis, software version 5.61 was used. Subjects wore only underpants and a cotton T shirt during the scan. For quality control, spine phantoms were scanned daily. The coefficient of variation for these BMC, bone area, and BMD measurements on a spine phantom over a period of two years (n = 482) was 0.43%, 0.29%, and 0.37%, respectively. DXA measurements and heights were compared with local references for children and adolescents (n = 343; age, 6–19 years)15or young adults (n = 53; 21 men; age, 20–29 years; Mølgaardet al, unpublished, 1995). The young adults consisted of healthy staff members or university students (mean (2 SD) height 182.7 (5.2) cm for boys/men and 168.5 (7.2) cm for girls/women; mean (2 SD) weight 78.8 (10.1) kg for boys/men and 64.1 (6.0) kg for girls/women). The height of the reference population was compared with a control population of 1977 children and adolescents from the Copenhagen area measured in the early 1990s (A Juul, unpublished, 1992). No significant differences between these two control populations were found.
The data were analysed as age and sex specific SDSs (SDS = observed − predicted SD). For participants ⩽ 19 years old, whole body measurements were also analysed using a stepwise approach, generating sex specific SDSs for height for age, bone area for height, and BMC for bone area, as described previously by our group.15 These three steps correspond to three different causes of reduced bone mass: short bones, narrow bones, and light bones.15 It was only possible to generate SDSs for bone area for height and BMC for bone area in patients ⩽ 19 years of age because of the large number of controls in this group.15
DISEASE SEVERITY
The patients were characterised by 11 different factors, which might be related to bone mineralisation, namely: (1) forced expiratory volume in one second (FEV1); (2) BMI; (3) the number of precipitating antibodies (precipitation lines (precipitins)) againstPseudomonas aeruginosa; (4) previous or current use of oral glucocorticoids, which divided the patients into two groups, those who had been treated with glucocorticoids orally and those who had not; (5) age; (6) the use of pancreas enzyme substitution measured in Pancreases (6.000 IE lipase)/kg/day; (7) the number of years with pulmonary P aeruginosa infection (pseudomonas years); (8) glucose tolerance, which divided the patients into three groups according to the oral glucose tolerance test: a capillary plasma glucose concentration ⩽ 8.8 mmol/litre was classified as normal glucose tolerance, a value of 8.9 to 12.1 mmol/litre as impaired glucose tolerance, and a value ⩾ 12.2 mmol/litre as diabetes mellitus16; (9) liver function, characterised as abnormal if one of the following parameters was abnormal: alkaline phosphatases, alanine aminotransferase, bilirubin, and coagulation factors II, VII, and X; (10) age at which the cystic fibrosis diagnosis was established; and (11) the possible presence of meconium ileus.
Lung function was measured within one week of the DXA scanning. Liver function parameters and P aeruginosaprecipitins were measured within three months of the scan and the oral glucose tolerance test was performed within six months in most cases and in a few cases within one year of the scan.
FEV1 was transformed to percent predicted values (FEV1 predicted) using the standard formulas of Polgar and Promadhat.17 The precipitins were measured by immunoelectrophoresis as described by Høiby.18 The precipitins were categorised into five groups according to their value: group 1, 0; group 2, 1–10; group 3, 11–20; group 4, 21–30; group 5, > 30.
STATISTICS
The statistical analyses were performed using the statistical package SPSS/PC+. The Wilcoxon signed rank sum test was used for comparing SDSs. The Mann-Whitney test was used to compare two different groups and the Kruskal-Wallis test was used for the comparison of three groups. Simple linear regression was used to correlate two variables.
A general linear model was used to identify variables that were predictable of decreased bone mineralisation and bone area.
ETHICS
Our study was carried out in accordance with the Helsinki II declaration and was approved by the local ethics committee of Copenhagen, Denmark (approval no. KF 01–058/93). Written informed consent was obtained from each participant and, when < 18 years old, also from the parents.
Results
BMC
BMC for age was significantly reduced in both male and female patients with CF ⩽ 19 years of age and > 19 years of age (table 1; fig 1). BMC for age was significantly lower in the patients > 19 years than those ⩽ 19 years of age in both sexes (p < 0.001 and p = 0.002, respectively). BMC for age correlated significantly with age (r = −0.34; p < 0.01). No difference between the two sexes was observed (p = 0.99). A general linear model was used to identify the most important factors associated with decreased BMC for age. The covariates and fixed factors for the model were those used to characterise the severity of the disease listed in the methods. BMI, pseudomonas years, and precipitins all showed a significant association with the BMC for age SDS (table 2). The greatest association between precipitins and BMC for age SDS was in the range 0–30, whereas the association declined when precipitins were > 30 (table 2).
Bone mineralisation standard deviation scores in patients with cystic fibrosis
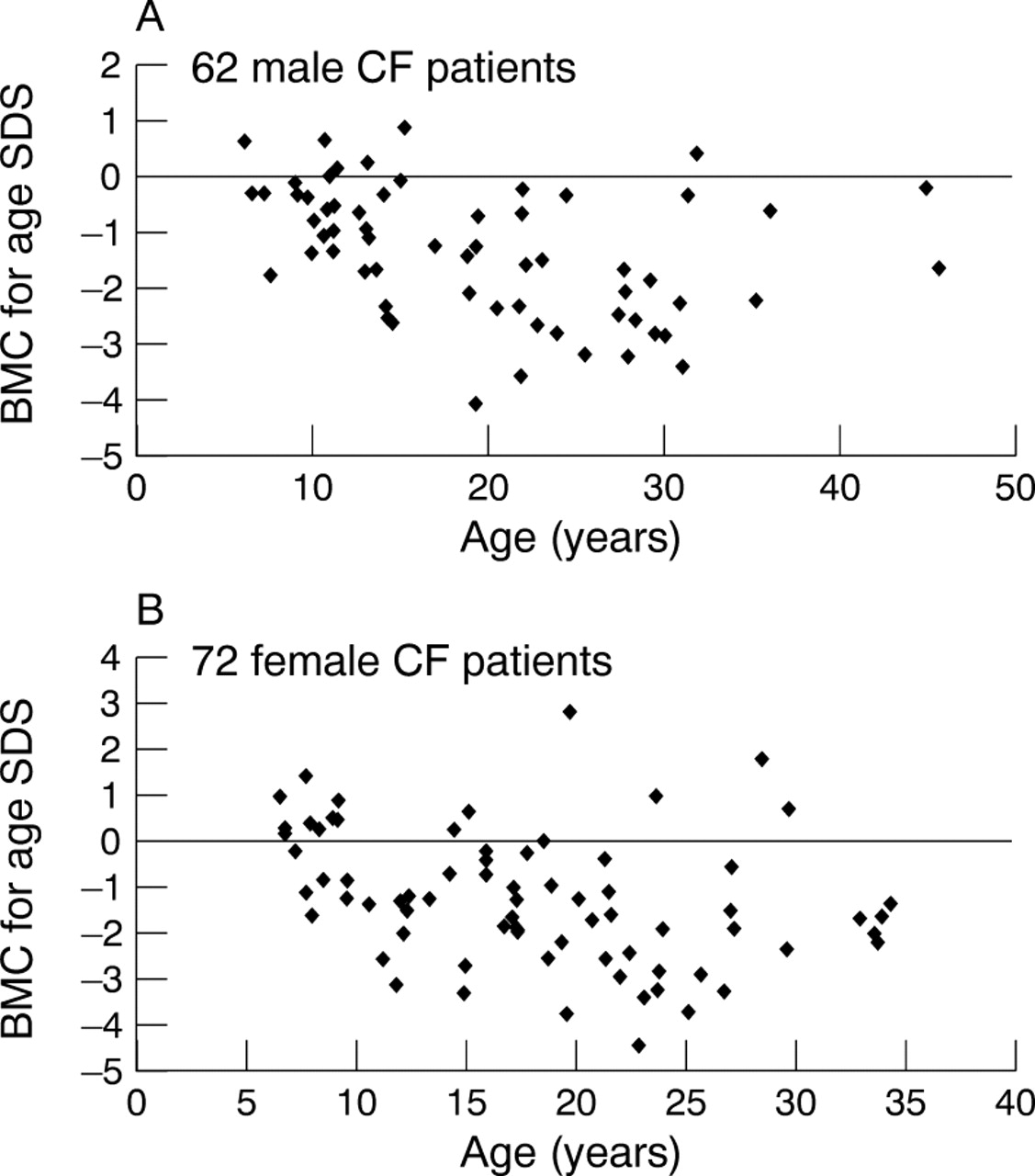
Bone mineral content (BMC) versus age expressed as standard deviation score (SDS) in (A) 62 boys/men and (B) 72 girls/women with cystic fibrosis (CF).
Parameter estimates for the reduced model of the influence of BMI, number of years with Psedomonas aeruginosa (PA) infection, and precipitins on BMC standard deviation score
In patients ⩽ 19 years of age, BMC was validated as suggested by Mølgaard et al.15 Height for age was significantly lower in patients with CF compared with normal controls, indicating “short bones” (table 1; fig 2A). Bone area for age was decreased to a more severe extend than height for age, resulting in significantly reduced bone area for height, indicating “narrow bones” (table 1; fig 2B). BMC for bone area was calculated and it was significantly increased in patients with CF of both sexes, indicating increased size corrected BMC (table 1; fig2C).

(A) Height versus age, (B) bone area for height versus age, and (C) bone mineral content (BMC) for bone area versus age expressed as standard deviation score (SDS) in 73 patients with cystic fibrosis (CF).
In patients ⩽ 19 years of age, a general linear model for height for age SDS revealed that FEV1 predicted and age were the most important factors for reduced height (table 3). FEV1predicted and BMI were the factors most associated with bone area for height SDS (table 3), and none of the factors used in the model had any significant association with BMC for bone area.
Parameter estimates for the reduced model for the influence of FEV1 predicted and age on height SDS, and FEV1 predicted and BMI on bone area for height SDS in patients < 19 years of age
BMD
In patients ⩽ 19 years of age, BMD for age was normal in boys and marginally but significantly reduced in girls (table 1; fig 3). Only two of 73 patients had a BMD SDS below −2.5 and 18 of 73 had a BMD SDS between −1 and −2.5. In adult patients with CF (> 19 years) of both sexes, BMD for age was significantly reduced (table 1; fig 3). Twenty three of 61 patients had a BMD SDS below −2.5 and 28 of 61 patients had a BMD SDS between −1 and −2.5, leaving only 10 with a BMD SDS above −1. BMD was significantly lower in both male and female patients > 19 years compared with patients ⩽ 19 years (p < 0.001 and p = 0.004, respectively). The BMD for age SDS correlated significantly with age (r = −0.35; p < 0.01). There was no significant difference in BMD SDS between male and female patients (p = 0.92).

{kind=link}
{kind=link}
{kind=link}
Bone mineral density (BMD) versus age expressed as standard deviation score (SDS) in (A) 62 boys/men and (B) 72 girls/women with cystic fibrosis (CF).
A general linear model was used to identify the most important factors associated with decreased BMD for age. FEV1 predicted, BMI, and precipitins were the factors significantly associated with a decrease in BMD SDS (table 4). As was seen for the BMC SDS, the greatest association between the precipitins and the BMD SDS was in the range of 0–30 (table 4).
Parameter estimates for the reduced model of the influence of FEV1, BMI, and precipitins on BMD standard deviation score
Discussion
Our study is the largest to date of bone mineralisation in patients with CF and the reference population was unique, partly because of the large number and partly because the controls were investigated using the same scanner as the patients.
In patients ⩽ 19 years of age, we found that the height SDS was reduced, indicating short bones. Furthermore, the bone area for height SDS was reduced, indicating narrow bones. Bone area was more severely decreased than BMC, resulting in an increased BMC for bone area, indicating increased size corrected BMC. In contrast, two studies3 4 have reported that BMAD in the whole body,3 lumbar spine, and femoral neck4 was significantly decreased in adult patients, indicating that the bone mineral deficit could not be attributed to differences in bone size alone. However, these two studies only investigated adult patients, who may be different from younger patients because of the severity of their disease and because less was known about the treatment of CF during their childhood. It was striking that none of the parameters examined were predictors of BMC for bone area, indicating that BMC for bone area was independent of the severity of the disease in the younger patients. Lung function and age were most important for the development of short bones, whereas lung function and BMI were most important for the development of narrow bones.
In patients ⩽ 19 years of age, BMC was significantly decreased in both sexes and BMD was normal in boys and slightly reduced in girls. In contrast, Henderson and Madsen found that the BMD SDS in the lumbar vertebrae and proximal femur in patients with CF < 18 years of age was significantly reduced, and that the BMD SDS declined rapidly with increasing age.2 They also found that the regional BMD SDS correlated well with weight as a percentage of normal median and FEV1 predicted. Baroncelli et alfound that the total body BMD SDS was significantly reduced in prepubertal, pubertal, and young adult patients with CF.19Finally, Salamoni et al found that BMC in 14 well nourished patients with CF, aged 6–20 years, was normal compared with 14 controls matched for sex, age, and nutritional status.13 Therefore, they suggested that osteopenia in patients with CF has a nutritional origin, rather than being related to a primary defect in bone mineral metabolism.13
We found that BMC and BMD were significantly reduced in adult patients with CF, which was in accord with several other studies.3-6
Data were separated on the basis of age (⩽ 19 and > 19 years) for statistical reasons because the number of normal controls ⩽ 19 years of age was very large compared with the number > 19 years of age. Both BMC for age and BMD for age showed a continuous decline with age, and the separation into above and below 19 years had no physiological reason.
We found that BMI was the only common factor that could predict the decrease in bone mineralisation, and the other factors were mainly factors that reflected the severity of the chronic pulmonaryP aeruginosa infection. Accordingly, other studies have found that BMI3 5 6 12 and disease severity5 12 had a significant influence on bone mineralisation. Two studies on patients with CF and end stage disease4 6 found that glucocorticoid treatment had significant influence on bone mineralisation, and these patients had an increased rate of fractures. In our centre, oral glucocorticoids are used only in cases of allergic bronchopulmonary aspergillosis, patients with Burkholderia cepacia, patients with severe asthma, and in extremely ill patients. Accordingly, only 15% of the patients had been treated with oral glucocorticoids, and this may explain why the BMD SDS was independent of oral glucocorticoids. However, it might also be possible that the effect of glucocorticoids was hidden by the association with lung function in this group of patients, making FEV1 predicted a stronger predictor of reduced bone mineralisation than the use of glucocorticoids.
Our group of patients had received a wide spectrum of treatments over the past 30 years, and the older patients were not treated as intensively during childhood as were the younger patients. This may influence bone mineralisation, and the severity of the disease has been identified as an important predictor of bone mineralisation in various studies.2 5 12 In our study, we were only able to calculate BMC for bone area in patients ⩽ 19 years of age, and it is possible that factors other than bone size are more important for bone mineralisation in adult patients.
We suggest that reduced bone size is the most important factor for decreased bone mass in younger patients with CF.
It is likely that some of the discrepancies between our finding of normal BMD SDSs in the younger patients may be explained by differences in bone size. However, differences in the use of oral glucocorticoids, antibiotic treatment, and nutritional regimen may also be important. Furthermore, some of the differences might be explained by differences in the type of bone examined. The lumbar vertebrae and proximal femur comprise mostly trabecular bone, whereas a total body scan (investigated in our study) represents ∼ 80% cortical bones. Trabecular bone has a more rapid turnover than cortical bone and reduced bone mineralisation will be manifested in trabecular bone before cortical bone.
We suggest that treatment to prevent osteoporosis in the younger patients in this population of patients with CF may need to be directed at increasing bone size. Increased bone width may be obtained by increasing BMI, and relevant treatment may therefore be turned against limiting the catabolic condition. Therefore, treatment should be directed at increasing the energy intake, correcting the malabsorption, and limiting pulmonary infection. The common treatment to prevent osteoporosis, using calcium and vitamin D supplementation, without targeting these other factors, may not improve bone mineralisation in patients with CF.
In postmenopausal women, the risk of osteoporotic fractures is doubled for every SDS that the BMD is reduced.20 21Therefore, we fear that patients with CF may develop osteoporotic fractures prematurely, because of the observed reduction in bone mass.