Article Text

Abstract
This study was undertaken to determine whether exposure to various indoor pollutants is associated with a higher prevalence of respiratory symptoms, a diagnosis of asthma, or more variable peak flow rates. Four hundred and twenty six children aged 8–11 years in four junior schools at three locations recorded respiratory symptoms and diagnosis of asthma using the ISAAC questionnaire. Daily peak flow measurements were taken during two six-week periods (winter and summer). Symptoms in children with and without asthma were not related to gas fires, cookers, smokers, or pets in the home. However, the variability of lung function, expressed as the coefficient of variation, in all children was increased with a household smoker. Environmental tobacco smoke increases airways variability in children with and without asthma. Its effects were not apparent from a questionnaire completed by parents, and the coefficient of variation of serially measured peak flows was a more sensitive indicator of lung function.
- tobacco smoke
- peak flows
- asthma
Statistics from Altmetric.com
There is evidence that asthma and respiratory symptoms in children have increased over the past 20 years.1-3Because this rise in prevalence has occurred in such a short time, it is unlikely to be of genetic origin and environmental factors have been implicated.4 5
Local environmental concerns about increased asthma episodes in an area near an open cast mine6 resulted in a study that collected subjective and objective respiratory data on a cohort of 440 school children. This paper describes the effects of the various documented indoor pollutants on the lung function of children attending schools at three different sites.
Methods
The study population was defined as all children in years four, five, and six (aged 8–11) in four schools at three sites expected to have different air quality, namely, in a village near the sea (site 1), in a valley near open cast mining (site 2), and in the city centre (site 3). Information on respiratory symptoms and diagnoses of asthma were obtained by submitting questions from the international study of asthma and allergies in childhood questionnaire (ISAAC).7To reduce selection biases, the request for consent to participate in the study, the explanatory letter, and the questionnaire were available in three languages—English, Welsh, and Bangladeshi—and were offered at least three times.
Our study took place in two six-week periods, from 9 January to 17 February 1995 and 5 June to 14 July 1995. During these weeks, at 09:00 each school day, the pupils recorded three peak flow measurements, using the Mini-Wright peak flow meter, while supervised by the teacher. A nurse trained the pupils and their teachers in the technique of peak flow monitoring before the start of the study. During the study, the schools were visited at least once a week and the diaries checked for completeness and for an accurate recording of peak flows. Each child in the study had a meter provided for use both at home and at school, thus helping to assure completeness of data collection.
We also identified children with asthma by provoking bronchoconstriction with exercise. The “free running asthma screening test” has been used widely to screen for asthma in children,8 9 and has proved to be feasible for use in large community studies because it is safe in children.
Ethical consent was obtained from the West Glamorgan local research ethics committee.
METHOD OF ANALYSIS
Although the diaries were examined at least once each week, the validity of some results were suspect for a variety of reasons and such results were coded as suspect until the child’s technique was seen to be satisfactory.
Using only the largest of the daily peak flows, if coded as good quality, the coefficient of variation was calculated for each child by dividing the standard deviation of his/her peak flows by the mean value for each of the study periods. Therefore, this coefficient took into account the difference in individual height and chest size.
From the ISAAC questionnaire, asthma was defined by affirmative answers to questions on “cough at night”, “ever wheeze”, “wheeze in the last year”, “asthma ever diagnosed”, or “asthma treated in previous four weeks”. The indoor pollutants that were recorded were the presence of gas fires, gas cookers, furry pets, or cigarette smokers in the home.
The association between asthma, defined by either symptoms or diagnoses from the questionnaire, attending a school at one of the three sites, and various indoor pollutants was explored using multiple logistic regression models. The relation between exposure to indoor pollutants and their effects on objectively measured lung function was examined using multiple linear regression, with the coefficient of variation of the peak flows being used as the dependent variable, and the different sites included as dummy variables.
Results
A total of 440 children were eligible for inclusion in the winter period and 435 in the summer. The overall response rate was 94% for the summer and winter periods. Four hundred and twenty seven questionnaires were completed in total, although some children were only in one of the study periods. Of these participating children, 205 were boys and 222 were girls.
SYMPTOMS
Table 1 shows the absolute number and percentage of children reporting different symptoms in the questionnaire, by site. More than one symptom could be reported if appropriate.
Distribution of symptoms by site
There was no significant difference in the distribution of asthma between the sexes and there were no significant differences between the age groups for the various symptom categories, nor was any consistent trend apparent (table 2).
Distribution of symptoms by age
Each of the following—wheeze in last year, ever asthma, wheeze with exercise, cough at night, and currently treated asthma—were tested separately as the dependent variable with age, sex, site, gas fires or cooking, pet ownership, and presence of a smoker in the home as predictor variables in logistic regression. A significant result was found in only one case, when exposure to smoking in the home was significantly related to wheeze in the past year. None of the symptoms was associated with attendance at any site when adjusted for confounders.
PEAK FLOWS
Figure 1 shows the mean coefficients of variation in the winter period for children in groups categorised by various symptoms. Greater variability of lung function was found in those reporting symptoms of asthma. The mean values of the coefficients for those with wheeze in the past year and a diagnosis of asthma (winter, 10.25; summer, 8.61) were significantly different from those children reporting no asthmatic symptoms (winter, 9.14; summer, 6.84; standard error of difference, 0.49; p = 0.03 (winter) and 0.63; p = 0.006 (summer)).

Coefficient of variation by symptom.
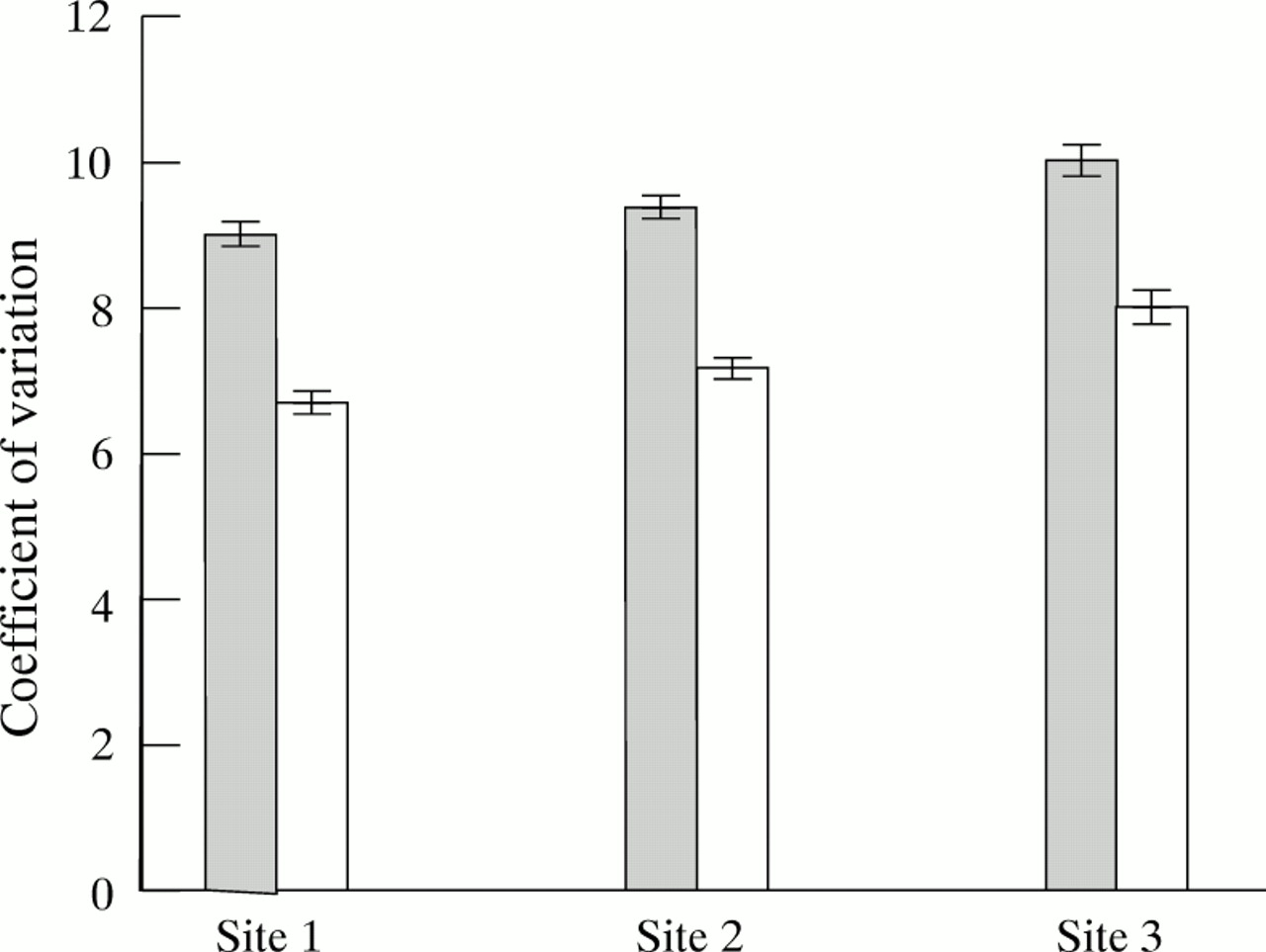
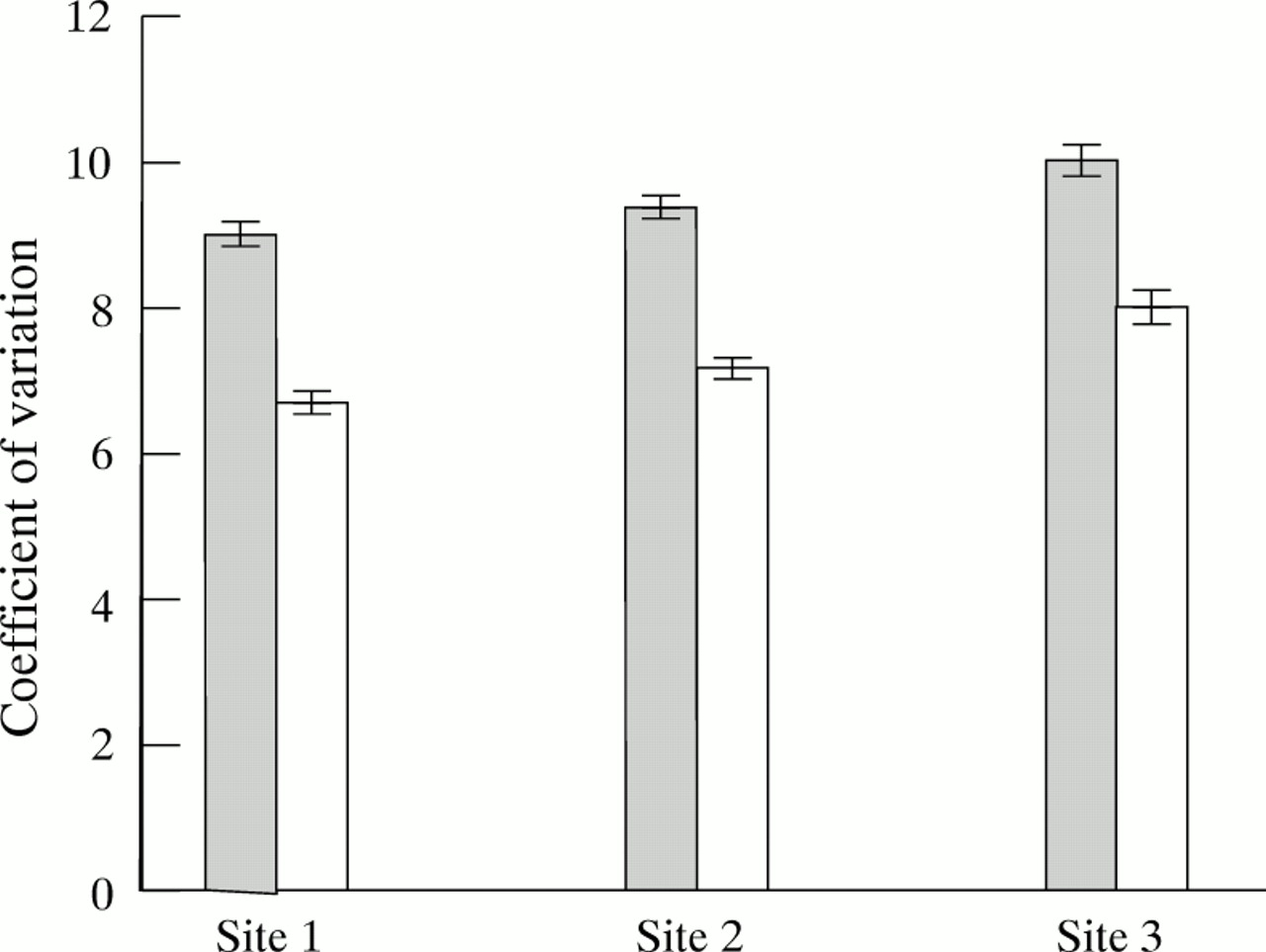
The coefficients also show that, as expected, variability of lung function decreases with age (fig 2). The mean coefficient of variation at 8 years old is significantly larger than that at 11 years old (p < 0.001). Figure 3 shows the values of the coefficients at the three sites, which show a trend in both summer and winter.
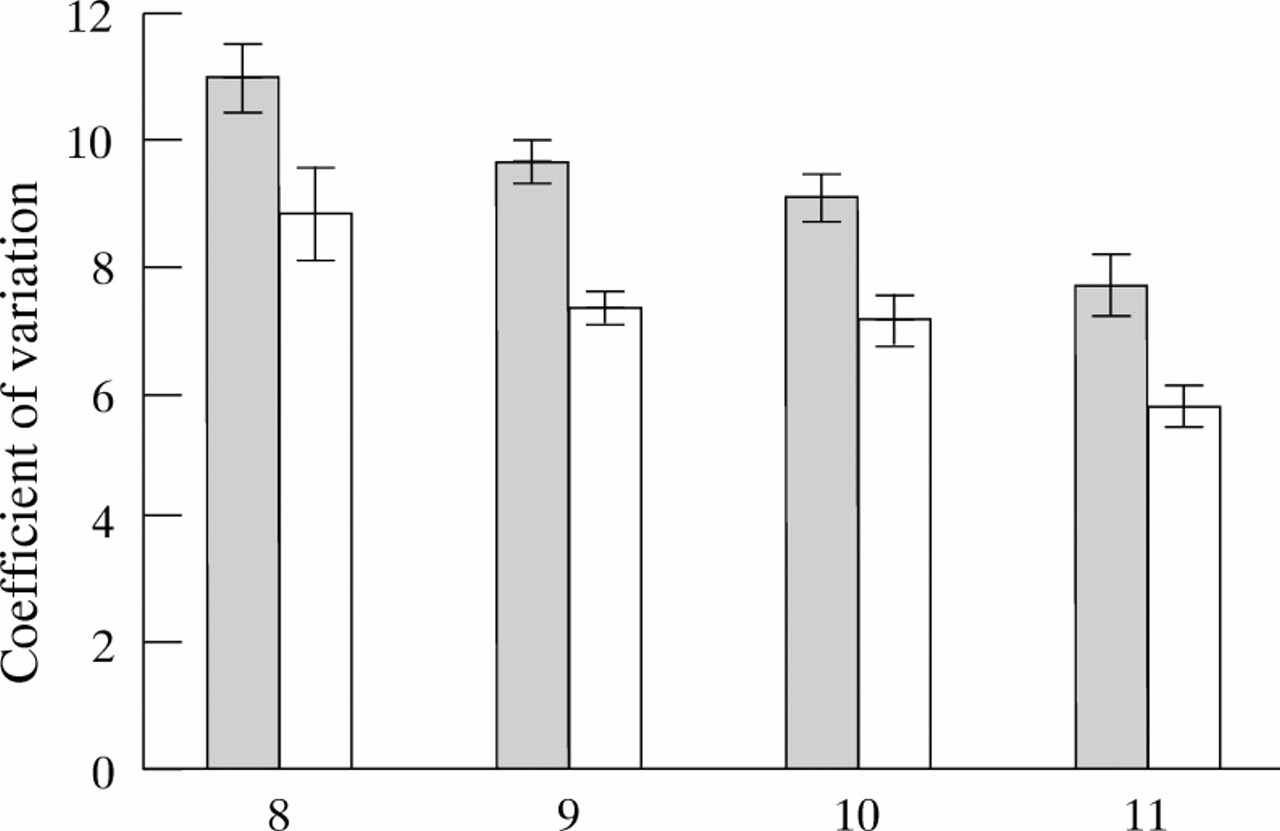
Coefficient of variation by age and season.
{kind=link}
{kind=link}
{kind=link}
Coefficient of variation by site and season.
Table 3 shows the effect of indoor pollutants on lung function in summer and winter. The mean values of the coefficients of variation in children living in a household with a smoker differed significantly from the mean values of children who did not live with a smoker (p = 0.02 (winter); p < 0.001 (summer)). The effect of smoking was greater in children with asthma (diagnosed, or wheeze in past year) than in children with no asthmatic tendency.
Comparison of coefficients of variation with exposure to indoor pollutants in winter and summer
The coefficients were tested in linear regression with the indoor pollutants, age, sex, and site as predictor variables. In the winter period, two variables were significantly related to the coefficient of variation, namely age (p < 0.001; regression coefficient, −0.09), which was negatively associated, and the presence of a smoker in the home (p < 0.004; regression coefficient, 0.01). Although the association was significant, the proportion of variability in the coefficients explained by this regression model was only 5.5% (adjusted R squared = 0.055). In the summer, three variables—age, smoking, and attendance at the city centre school—had a significant effect on airways variability (adjusted R squared = 0.06).
Discussion
Variation in general practitioners’ diagnoses and treatments, and peoples’ perception of illness mean that attendance at doctors’ surgeries, drug treatment of asthma, and even attendance at hospital can all be unreliable estimates of the experience of reversible airway disease in the community. Although there has been reasonable consistency in the diagnostic criteria used by clinicians in the past two centuries,10 it has been more difficult to standardise a precise definition for use in epidemiological surveys. Even different physiological diagnostic tests have been shown to correlate poorly in school children.11 To overcome these difficulties and to minimise bias, standardised methods of comparing symptoms and lung function are required. In our study, symptom prevalence was measured by the ISAAC questionnaire and serial objective measurements of peak flow variability were used.
The response rate of 94% ensured that there was a minimal amount of selection bias and collecting objective data prospectively ensured no recall bias or bias because of doctors’ referral behaviour.
Our study found the prevalence of asthmatic symptoms in the whole cohort to be in the highest ranges of those reported in the literature.3 4 9 12 For example, our study found the prevalence of wheeze in the last year to be 17%. Cliffordet al found the overall prevalence of wheeze in the last year in children aged 7 and 11 to be 9.5%.9Burr et al and Strachanet al found the prevalence to be 15%, although the age groups examined were not exactly the same as our cohort—Burr reported on 12 year old children2 and Strachan reported on ages ranging from 5 to 17 years.12
In our study, we found no association between gas cooking or fires in the home and asthmatic symptoms. High levels of nitrogen oxides can occur in homes where there are poorly vented gas cookers and heaters, and poorer lung function has been documented in children as a result.13 14
No association between smoking and asthmatic symptoms was identified on analysis of our parentally completed questionnaire. The deleterious effect of passive smoking has been identified previously by symptom questionnaire in large studies of school children,15 16although others have failed to show a consistent relation between respiratory symptoms and indoor pollutants.17 The deleterious effect of passive smoking on objectively measured lung function was confirmed in our two study periods of winter and summer and the finding is consistent with other studies.18 19Although peak flow measurements have been criticised for being insensitive to small changes or mild disease,20 in our study of 426 children they showed consistent and expected associations with age, season, and reported symptoms, giving confidence in the results showing that poorer lung function was associated with passive smoking.
Conclusions
The effect of living with a household smoker on the lung function of children was consistently demonstrated in summer and winter periods by prospective measurements of peak flows. The analysis of a standard symptom questionnaire did not detect either these deleterious effects or the increasing stability of lung function with increasing age. The coefficient of variation has the advantage of being easily calculated from objectively measured data and may provide a more sensitive indicator of changes in lung function than questionnaires in studies of environmental pollutants.
Acknowledgments
We acknowledge with thanks the secretarial help given by Mrs S Morgan and Mrs J Dare at West Glamorgan Health Authority (now Iechyd Morgannwg Health), and the enthusiastic participation by pupils and staff at the junior schools in Bishopston, Terrace Road, and Glynneath. This study was funded by the Department of Public Health Medicine, West Glamorgan Health Authority, the Environmental Health Department, Swansea City Council, the Environment and Highways Department, West Glamorgan County Council, the Environmental Health Department, Neath Borough Council, and British Coal Opencast.