Article Text

Summary
A 40-year-old man with Wegener's granulomatosis with renal and ocular involvement was admitted with symptoms of fever, malaise and cough not responding to oral antibiotics. On initial assessment, he had patchy consolidation but was also found to have a new cardiac murmur. He was mildly anaemic. Within 2 days of hospital stay his haemoglobin dropped and he became tachypnoeic. High-resolution CT found extensive pulmonary infiltrates, which suggested pulmonary haemorrhage, and blood cultures were negative. He was on antibiotics because of suspected infective endocarditis and this made any immunosuppressive treatment for active Wegener's granulomatosis very difficult. After extensive discussion with tertiary centres he had pulse methylprednisolone for 3 days. His echo detected aortic regurgitation but no vegetations. His antibiotics were stopped and he had cyclophosphomide to control his active Wegener's granulomatosis.
He improved remarkably with immunosuppression and non-invasive ventilation and was discharged. He had a further echo, which confirmed moderate aortic regurgitation. He is awaiting cardiac catheter studies but the fact is acute aortic regurgitation has happened due to active Wegener's granulomatosis along with pulmonary haemorrhage. This is a very rare presentation.
Statistics from Altmetric.com
Background
Wegener's granulomatosis is a systemic necrotising vasculitis, which could potentially affect any organ system. First described in 1931 by Klinger,1 and further characterised by Wegener2 in 1936, it has evoked keen interest among rheumatologists all over the world, with diagnostic classification, disease assessment and the use of biologics being the main points of discussion.3 Cardiac involvement was found originally at the operating table (valve surgery) but, with improved diagnostic techniques and regular follow-up, cases have been found more frequently (varies between 6% and 44%).
Large vessel disease in anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis may present as stenosing large vessel arteritis, aneurysmal disease, aortic dissection, aortic rupture, aortic regurgitation and death.4 5 Cardiac manifestations can arise from the coronary arteries, pericardium, myocardium, endocardium, valves, conduction system and great vessels, but in most cases cardiac involvement is clinically silent.
Consequently, a regular cardiovascular evaluation, including echocardiography, should be performed in every patient with Wegener's granulomatosis, while patients with disease activity should be closely monitored for cardiac complications even in the absence of specific symptoms.
Case presentation
This 40-year-old man with Wegener's granulomatosis diagnosed 12 months previously with renal (biopsy noted focal segmental necrotising glomerulonephritis) and ocular (resistant bilateral scleritis) involvement had completed a course of intravenous cyclophosphamide and steroid treatment and was due to start on methotrexate. His inflammatory markers, urine protein, cytoplasmic ANCA (cANCA) levels and complement had normalised after initial treatment.
Prior to starting methotrexate he developed symptoms of malaise, fever and cough, which was initially treated as a chest infection with antibiotics. His symptoms deteriorated and a new diastolic cardiac murmur was noted. His inflammatory markers were significantly elevated with a C reactive protein 209 and erythrocyte sedimentation rate 113. His chest x-ray (CXR) showed right upper lobe patchy consolidation (figure 1). He had polymorphonuclear leucocytosis, haemoglobin 9.4 g/dl with normal electrolytes; cANCA PR3 had risen to 60. Within 36 h his haemoglobin dropped to 4.5 g/dl and CXR showed progressive pulmonary infiltrates.

Chest roentgenogram showing patchy consolidation on admission.
Investigations
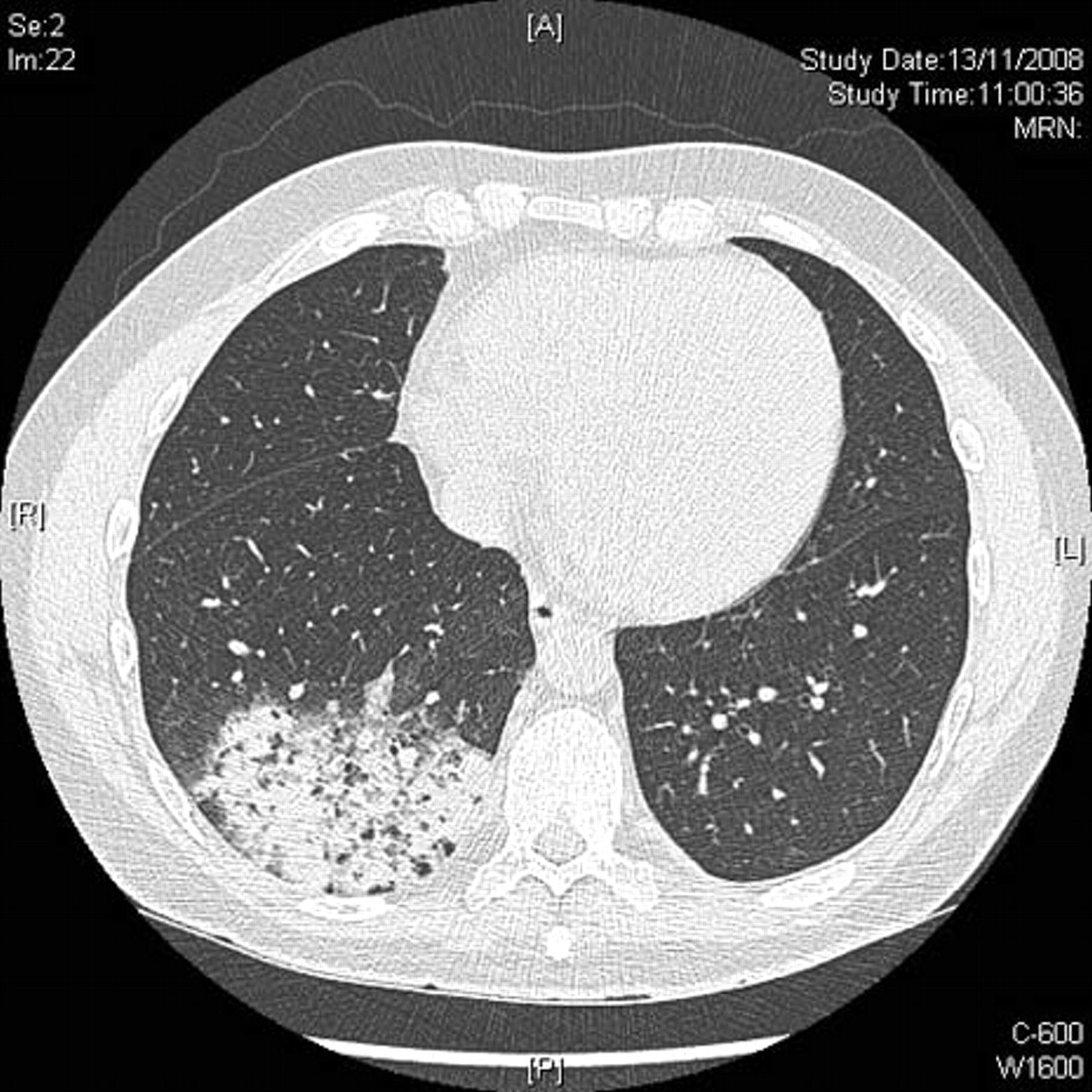
It became obvious that he had developed a pulmonary haemorrhage. His chest high-resolution CT scan confirmed extensive pulmonary changes (figure 2). His transthoracic echo noted moderate aortic regurgitation (video 1), which was confirmed by a tracheoesophageal echo (figure 3). There were no vegetations evident. A bronchoscopic lavage was performed, which excluded any infective or malignant process. Blood cultures remained negative.

CT scan showing pulmonary infiltrates.
A cute aortic regurgitation and turbulence across aortic valve.

Echo showing aortic regurgitation jet.
Differential diagnosis
Gastrointestinal bleed, diffuse pulmonary haemorrhage, infective endocarditis and active Wegener's vasculitis.
Treatment
He received blood and intravenous methylprednisolone 1 g for 3 consecutive days. Initially his inflammatory markers remained high and his serial CXRs showed no significant improvement. His oxygen requirement increased and he was transferred to a high dependency unit for continuous positive airway pressure. He was pulsed with intravenous cyclophosphamide and daily 60 mg of oral prednisolone. At this point, the use of intravenous immunoglobulin and plasmapheresis was discussed with a tertiary centre.
Outcome and follow-up
It was several days before any significant clinical, biochemical or radiological improvement occurred (figure 4). At 3 months his serological and inflammatory markers had normalised and radiological changes resolved. However, the latest echo showed persistent moderate to severe aortic regurgitation and he awaits cardiac catheter studies for further assessment.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Chest roentgenogram showing improved signs after treatment.
Discussion
This case is presented in view of the rarity of aortic valve involvement with Wegener's granulomatosis and also the complexity of managing pulmonary haemorrhage in the acute setting. It also demonstrates the need to be vigilant for infection at all times especially in disease relapse. Only very few cases have been published with aortic involvement.
Learning points
▶ Pulmonary haemorrhage is to be considered when acute anaemia occurs in patients with vasculitis.
▶ Infection needs to be ruled out before subjecting the patient on immunosuppression.
▶ It is essential to perform a periodical echocardiogram in patients with Wegener's granulomatosis, even in the absence of a specific symptom, in order to identify early cardiac and great vessels involvement.
▶ Infective endocarditis is the diagnosis until proven otherwise if new regurgitant cardiac murmur appears in immunocompromised patients.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.