Article Text

Abstract
Background: Diagnosis of active pulmonary and paranasal involvement in patients with Wegener’s granulomatosis (WG) can be difficult. The diagnostic value of gallium-67 scintigraphy in WG is unclear.
Objective: To evaluate the added diagnostic value of gallium-67 scintigraphy in patients with WG with suspected granulomatous inflammation in the paranasal and chest regions.
Methods: Retrospectively, the diagnostic contribution of chest and head planar gallium scans in 40 episodes of suspected vasculitis disease activity in 28 patients with WG was evaluated. Scans were grouped into normal or increased uptake for each region. Histological proof or response to treatment was the “gold standard” for the presence of WG activity.
Results: WG activity was confirmed in 8 (20%) episodes, with pulmonary locations in three, paranasal in four, and both in one (n=7 patients); all these gallium scans showed increased gallium uptake (sensitivity 100%). Gallium scans were negative for the pulmonary area in 23/36 scans (specificity 64%), and negative for paranasal activity in 13/16 scans (specificity 81%) in episodes without WG activity. Positive predictive value of WG activity for lungs and paranasal region was 24% and 63%, respectively, negative predictive value was 100% for both regions. False positive findings were caused by bacterial or viral infections.
Conclusion: Gallium scans are clinically helpful as a negative scan virtually excludes active WG. Gallium scintigraphy of chest and nasal region has a high sensitivity for the detection of disease activity in WG. However, because of positive scans in cases of bacterial or viral infections, specificity was lower.
- Wegener’s granulomatosis
- gallium-67 scintigraphy
- ANCA, antineutrophil cytoplasmic antibodies
- FDG, [18F]fluorodeoxyglucose
- PNR, paranasal region
- WG, Wegener’s granulomatosis
Statistics from Altmetric.com
- ANCA, antineutrophil cytoplasmic antibodies
- FDG, [18F]fluorodeoxyglucose
- PNR, paranasal region
- WG, Wegener’s granulomatosis
Wegener’s granulomatosis (WG) is a rare disease of unknown aetiology, characterised by necrotising vasculitis and granulomatous lesions, primarily affecting the upper and lower respiratory tract.1,2 Antineutrophil cytoplasmic antibodies (ANCA) directed against proteinase-3 or myeloperoxidase in plasma are considered to be a useful tool for diagnosis of WG. However, the presence of these antibodies is not strictly related to disease activity. ANCA levels can be persistently high even during remissions without any sign of disease activity, and in addition, titres may remain low despite disease progression or relapse.3,4 Other tools for diagnosis of active disease are biochemical parameters of inflammation and tissue biopsies. However, the outcome of these diagnostic tools is frequently inconclusive. Inflammatory blood parameters are non-specific and tissue biopsies can lack the typical histological findings owing to sampling error.5,6 Finally, imaging studies such as high resolution computed tomography imaging are often unable to distinguish correctly active WG from inactive scarred or fibrotic tissue.7 For treatment decisions, a better method is desirable to detect or exclude WG activity. In particular, correct exclusion of WG activity will prevent further invasive diagnostic procedures and unnecessary intensive treatments.
Gallium-67 (67Ga) scintigraphy is commonly used in the detection of malignant lymphoma or inflammatory lesions such as sarcoidosis.8–10 Gallium leaks through the vascular epithelium at the site of inflammation, where it is bound to the lactoferrin of the macrophages.11 The value of 67Ga scintigraphy in detecting Wegener’s disease activity is unknown. This study aimed at evaluating 67Ga scintigraphy in the detection or exclusion of disease activity in patients with known WG suspected to have had a disease relapse, especially in cases of difficult diagnosis.
PATIENTS AND METHODS
Patients
Twenty eight patients with WG (10 men, 18 women; age 34–90 years) diagnosed as having WG by the current classification criteria, were included in this retrospective analysis.12,13 Between 1985 and 2000, in 28 patients, a gallium scan of the chest (n=40) and paranasal region (n=21) was performed in the diagnostic investigation of suspected local WG activity relapse. The mean interval since the initial diagnosis of Wegener’s disease was 7.7 years (range 1–16). Most patients received treatment with co-trimoxazole as part of the standard maintenance treatment for WG. In cases of suspected relapse, diagnosis was difficult to obtain. Previous diagnostic analysis, including clinical features, laboratory assessment for ANCA, biochemical parameters of inflammation, lung and/or nose tissue biopsy, chest and nasal sinus radiographs, and computed tomography, had been inconclusive to confirm disease activity or an alternative diagnosis.
67Ga citrate scintigraphy
Imaging of the head and chest was performed 72 hours after intravenous injection of 185 MBq of 67Ga citrate. Planar scans (10 minutes) were acquired on gamma cameras, equipped with medium energy, all purpose, parallel hole collimators. About 300 000 and 500 000 counts were obtained for a head scan and chest scan, respectively. Photopeaks of 93, 184, and 296 keV in a 128×128 matrix were used.
Analysis
Gallium scans of the head and chest were reanalysed by a nuclear medicine physician, who was unaware of the clinical outcome. In case of differences between the original and the reanalysis, a consensus was reached by consulting colleagues also unaware of the original analysis. Gallium uptake was classified as either normal or increased, for both the paranasal region (PNR) and the lung. Quantification of lung uptake was obtained by drawing regions of interest over both lungs and the liver on posterior and anterior views. The geometric mean count density in both lungs was divided by the count density in the liver yielding a lung/liver ratio. In addition, regions of interest were drawn around the PNR of interest and over the brain, yielding a PNR/brain ratio. Only gallium scans performed in the past six years were digitally available, so calculation of the count rate ratios was only possible for these recent scans (n=30). A few older gallium scans had been quantified in the past (n=11).
True active pulmonary or paranasal WG involvement was concluded if further diagnostic procedures led to histologically proved active WG disease at the site of increased gallium uptake, or in the case of a clinical diagnosis only after appropriate response to treatment. In some cases, WG activity was only localised in the kidneys, proved by renal biopsy. Unremarkable gallium scans of the lungs and paranasal region were considered true negative scans if progression or renewed signs of WG remained absent for at least three months without treatment. Active bacterial or viral infection of the lung and nose was excluded as much as possible by culture and serology. However, clinical response to empirical antimicrobial treatment(s) and the absence of WG manifestations in the next three months was considered to indicate the presence of infection. PNR/brain, lung/liver ratios and ANCA titres of patient groups with and without WG activity were compared using the Mann-Whitney test. Two sided p<0.05 was considered significant.
RESULTS
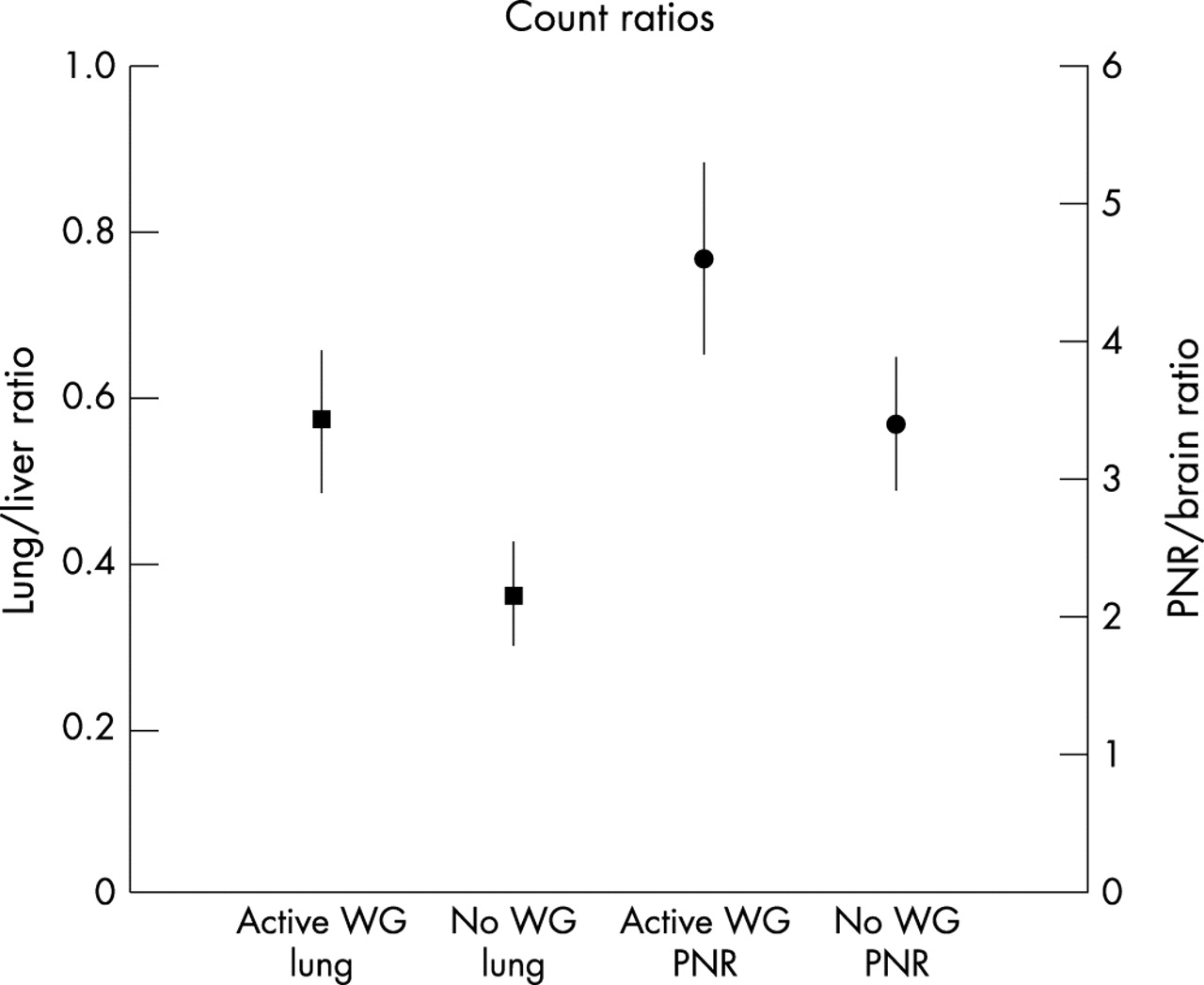
WG activity was confirmed in eight episodes (20%) (six histologically and two clinically), with pulmonary locations in three, paranasal in four, and both in one (seven patients) (tables 1 and 2). In all these patients, chest or paranasal scans showed increased gallium uptake, yielding a sensitivity of 100% (figs 1 and 2). The mean lung/liver ratio of patients with, compared with those without, active WG was 0.57 v 0.36, respectively (p=0.002, fig 3). The mean PNR/brain area ratio of patients with, versus without, active WG was 4.6 v 3.4, respectively (p=0.027, fig 3). After treatment, a follow up gallium scan (mean interval two months) of three patients, who all had a true positive chest or paranasal scan at diagnosis, showed normalisation of pulmonary or paranasal gallium uptake. In four additional episodes WG disease activity was diagnosed outside the pulmonary and paranasal regions. In three of four chest and one of two PNR gallium scans of these four episodes, increased uptake was seen. As there was no histological proof of disease activity at these sites, and clinical and radiological signs did not change during treatment or were found to be caused by concomitant infection, these findings of increased gallium uptake are considered to be false positive (tables 1 and 2).
Gallium scans results for detection of pulmonary Wegener disease activity
Gallium scans results for detection of paranasal Wegener disease activity

Gallium scan; anterior view of the head with normal uptake in a patient without WG (A) and increased (B) uptake in the paranasal region in a patient with active WG. Active WG in the nose was histologically proved in the patient shown in (B). Physiological uptake in the lachrymal and salivary gland on the right side of the head.

Gallium scan; anterior chest view of normal uptake in a patient without WG activity (A) and increased (B) uptake in a patient with active WG. Active WG in the lung was histologically proved in the patient shown in (B).
{kind=link}
{kind=link}
{kind=link}
Normalised count rate ratios of lung/liver and PNR/brain area in patients with and without WG activity.
In patients without active WG, gallium scans were negative for pulmonary activity in 23 out of 36 episodes, and negative for paranasal activity in 13 out of 16 episodes.
The negative predictive values are 100% for lungs and PNR and a specificity of 64% and 81%, respectively. Positive predictive value for lungs and PNR was 24% and 63%, respectively. False positive findings were all related to bacterial or viral infection, which were either subsequently diagnosed by additional culture or serological results or by the response to empirical antimicrobial treatment. Patients without WG activity and an abnormal gallium scan caused by infection showed a mean lung/liver and PNR/brain area ratio of 0.62 and 4.2. These ratios were not significantly different from those of patients with active WG (p>0.6). ANCA titres were not significantly different in patients with active WG compared with those with inactive WG (p=0.12); ANCA titres were not related to the scan findings.
DISCUSSION
Active WG requires intensive and prolonged treatments, which can be complicated by serious side effects. Therefore clinicians need useful diagnostic tools before starting these treatments. Especially in cases of difficult diagnosis, imaging tools can make diagnosis more likely. Radiological tools like x ray examination and computed tomography visualise anatomical abnormalities in tissue but cannot always distinguish between active WG and fibrotic or scarred tissue.
Up to now, no reports of the value of gallium scintigraphy in patients with WG have been published, except for two case reports14,15: in both increased pulmonary gallium uptake in histologically proved pulmonary WG activity was found. Our retrospective study of 40 episodes in 28 patients clearly shows that in patients with suspected WG activity, a normal gallium scan virtually excludes disease activity. A normal gallium scan can prevent unnecessary treatments and, also, treatment of patients without WG activity can be safely withdrawn. In addition WG activity in the lungs and paranasal region can also be detected with gallium scintigraphy because of significantly increased uptake in the lung and PNR. The measurement of count rate ratios may be helpful to follow active WG during and after treatment, as the count rate ratio accurately detects normalisation of gallium uptake in the lungs and PNR. However, because of the occurrence of positive gallium scans in cases of bacterial and viral infections, the specificity for WG is lower. This prevents differentiation between WG activity and infection. The outcome of the gallium scans resulted in additional diagnostic procedures directed at sites of increased gallium uptake, leading to confirmation of WG activity or other diagnoses.
In the case of a negative chest and PNR gallium scan, no patient of this group showed WG activity within three months after the negative gallium scan. The added value of gallium scans is also confirmed by the observed lack of adequate association between ANCA titres and WG activity, which has also been found by other investigators.3,4 In other studies, radiolabelled granulocytes showed an added value in detecting active WG.7,16,17 In an another vasculitic disease, Kawasaki disease, radiolabelled granulocytes provided a more sensitive method than gallium scintigraphy for the detection of myocarditis in the acute phase, whereas gallium scintigraphy was more sensitive in detecting chronic myocardial inflammation.18,19 In our patients, disease activity is prolonged for weeks or months and therefore gallium scintigraphy is likely to be more suitable for detecting chronic disease activity. Additionally, a main disadvantage of using radiolabelled granulocytes is the comprehensive labelling processes, which may generate false positive lung uptake.17
Newer radionuclide techniques may also be used in the assessment of vasculitic disease activity in diseases like WG. Granuloma tissue of patients with active WG is likely to express somatostatin receptors in sufficient numbers to allow in vivo visualisation using an indium-111 (111In) labelled somatostatin analogue. Besides WG, high somatostatin-receptor expression is found in the tissue of patients with sarcoidosis, tuberculosis, and aspergillosis.20 [18F]Fluorodeoxyglucose (FDG) positron emission tomography may also be of value in the diagnosis of WG activity. FDG makes in vivo measurement of metabolism processes possible, and increased FDG uptake can be seen in various conditions such as ischaemically myocardial tissue,21 cancer,22 or inflammatory processes.23 Experience with these newer techniques is limited but it may be expected that these techniques also will not be sufficiently specific to diagnose active WG.
Our study has limitations, because the set up of this study was retrospective and gallium scans were performed in case of difficult diagnosis, which resulted in a small selected patient group. In this selected group we demonstrated high sensitivity and a high negative predictive value in the detection of active WG disease. It is not known whether consecutive inclusion of all patients with a suspicion of WG would have resulted in better results with more true positive and fewer false positive gallium scans. Another limitation is the lack of histological proof of disease activity tissue biopsy in some patients in whom clinical outcome had to be taken as a second best “gold standard”. In addition, the use of co-trimoxazole maintenance treatment in our patients might have influenced the occurrence infections.
In conclusion, detection of Wegener’s disease activity is often difficult, therefore gallium scans are clinically helpful, as a negative scan virtually excludes active WG. Normal gallium scans preclude unnecessary treatment. Gallium scintigraphy of the chest and nasal region has a high sensitivity for the detection of disease activity in WG. However, owing to positive scans in cases of bacterial or viral infections, the specificity is lower.