Article Text

Abstract
Chronic arthritis is characterised by chronic joint inflammation and concurrent joint erosion and destruction. The inflammatory cytokine interleukin 1 (IL1) has been shown to be a key mediator in the autoimmune disease rheumatoid arthritis (RA). Interleukin 1 mediates bone resorption and cartilage destruction, but may not play as dominant a part in joint swelling and inflammation. Interleukin 1 receptor antagonist (IL1Ra) selectively inhibits the effects of IL1 by competing for the IL1 receptor on all surfaces of the synovium. In a randomised controlled trial in 472 patients with active disease, IL1Ra 30 mg/day, 75 mg/day or 150 mg/day given by subcutaneous injection significantly reduced the signs and symptoms of RA at 24 weeks. An American College of Rheumatology (ACR) 20% response was seen in 43% of the patients treated with 150 mg/day at 24 weeks. IL1Ra was well tolerated; injection site reactions were the most common adverse event. In another trial, in 419 patients with active RA treated concomitantly with methotrexate, there were ACR 20% responses after 24 weeks in 42% of the patients treated with 1 mg/kg/day by subcutaneous injection and in 35% of those treated with 2 mg/kg/day. I1Ra offers a unique selective, targeted mechanism of action to block the IL1 mediated effects of RA.
- interleukin 1
- rheumatoid arthritis
- cytokine
- tumour necrosis factor α
Statistics from Altmetric.com
Rheumatoid arthritis (RA) has puzzled medical science for centuries. It is a chronic systemic inflammatory disease that occurs almost three times as often in women as in men, mainly affecting those between the ages of 29 and 50 years. The crippling disorder may have a sudden onset, and often has a poor prognosis. When the signs of the disease are not clear, RA can remain undiagnosed for years and can continue to progress. Recent research has better defined the biology of RA and has identified several cytokine messengers as responsible for the destruction in the affected joints throughout the body.1
In RA, an unknown environmental agent such as a virus or toxin triggers an autoimmune response in genetically susceptible persons. This innate response first evolved in microorganisms as a defence against microbial invasion, and differs from the acquired (memory type) immune response.2 The innate (natural or non-specific) immune response works to neutralise and destroy invading microorganisms, reduce tissue injury and cell death, promote recovery and decrease the risk of opportunistic infections.3 It produces internal mediators, particularly the cytokines, to ward off the invading agent. Cytokines increase the production of migrating defence cells, including macrophages, neutrophils and chondrocytes. The overproduction of specific cytokines, such as interleukin 1 (IL1) and tumour necrosis factor α (TNFα), drives pathophysiological processes that lead to the clinical symptoms of RA.1 ,2 ,4 ,5 Studies have shown that IL1 and TNFα have overlapping proinflammatory effects in patients with RA (table 1).6
Overlapping proinflammatory effects of IL1 and TNFα
New treatment strategies for RA target these mediators of the inflammatory response. An avenue of therapeutic entry is the cytokine network that regulates the innate immune system. Studies in animals and humans have identified IL1 as a pivotal mediator in the disease process. Patients with active RA have been shown to have increased plasma concentrations of IL1β.7 Three cytokines, IL1, IL6 and TNFα, seem to play important parts in initiating and regulating the innate immune response.6 Evidence indicates that IL1 acts as a comitogen for T lymphocytes, while TNFα transmits the T helper cell type 1 T cell response and IL6 promotes B lymphocyte growth.2
Role of IL1
IL1 serves as the prototypic “alarm” cytokine in healthy persons, affecting nearly every tissue and organ in the body. The induction of IL1 by a virus, bacterium or toxin leads to the production of several other proteins, including TNFα, IL6 and IL1 receptor antagonist (IL1Ra), through cytokine production or signalling pathways.1 ,2 ,8 Some of the cytokine pathways induce immunological mechanisms, and others produce haematological changes. IL1 is produced by a variety of cells that are part of the innate immune system. There is increasing evidence that constant activation of the innate immune system occurs in several chronic inflammatory processes, including RA.2 This persistent activation promotes constitutional changes, metabolic abnormalities and destruction and remodelling of tissues in persons with chronic, uncontrolled disease.9 Experiments have found that the administration of IL1 stresses host defences and mediates the response to disease. In animal and human studies, overproduction or continued production of IL1 compromises host defences in autoimmune disorders such as RA.10 Thus, reducing the synthesis of IL1 or blocking the effects of an overabundance of IL1 may offer a therapeutic option for such conditions.
IL1 causes inflammatory cells to move into the structures of joints and the synovium in patients who have RA. A currently unknown antigenic trigger activates the production of IL1 in the joint by macrophages (lymphocytes, monocytes and transformed fibroblasts).11 ,12 These cells further produce or secrete additional cellular messengers such as the proteoglycans and proteases that can lead to the formation of the pannus, which accumulates in the joints. Destructive enzymes can then go on to destroy cartilage and ultimately degrade and erode bone. Selectively and specifically blocking IL1 is a targeted, rational treatment against the destructive effects of this cytokine in RA.13
At the cellular level, IL1 induces other cytokines, including IL6 and TNFα.1 ,2 TNFα is a very potent inducer of IL1 in animal studies. Together, IL1 and TNFα act synergistically to cause further damage to the joints in patients with RA.14 This relation between cytokine pathways may explain why, although TNFα may not be a direct cause of RA, anti-TNF based treatment may have a therapeutic effect in some patients (J I Frishmanet al, European League Against Rheumatism (EULAR) Nice, France, 2000 and Van den Berg15).
In animal models of RA, both IL1 and TNFα seem to play a crucial part in causing the degradation of proteoglycans that can damage the joints.2 ,16 ,17 Local production of IL1 in the early immune complex arthritis model in the mouse shows this cytokine to be directly responsible for the inhibition of proteoglycan synthesis.16 IL1 and TNFα may act synergistically to mediate parts of the inflammatory process. However, some data suggest that IL1α in fibroblasts may serve as the endogenous mediator of joint damage in RA.18
IL1 also seems to promote joint breakdown by attracting inflammatory leucocytes and activating synovial cells. TNFα seems to have no effect on any of these promoters of RA: the deleterious cell influx, proteoglycan synthesis or proteoglycan degradation.19 Some animal research suggests a “decoupling” of the IL1 and TNFα pathways, with IL1 performing the pivotal role in this disease.15 ,20 There seems to be a dysregulation of IL1Ra production and a failure to modulate the effects of IL1β in people with RA.21
The action of IL1Ra and its recombinant form
IL1ra, the first described naturally occurring specific receptor antagonist of any cytokine or hormone, was discovered in the 1980s.22 The binding of IL1Ra to the IL1 receptor on the cell surface is almost irreversible, and shows no agonist activity in the body.2 Animal research with recombinant human IL1Ra has shown that it selectively and directly blocks IL1 (fig 1). In the rabbit lipopolysaccharide induced arthritis model, the levels of endogenous IL1Ra were too low to suppress the IL1 that mediates the disease.23 Endogenous expression of IL1Ra was also a determinant in transgenic mice being susceptible to collagen induced arthritis.24

IL1Ra binds to IL1 receptor type I but does not activate the cell.2
Animal and human studies alike have shown that IL1 and IL1Ra are present in the inflamed synovium and rheumatoid joints, indicating that the IL1 pathway is expressed and regulated within diseased joints.25 ,26 Injecting IL1 into the knees of rabbits produced a synovitis with a loss of proteoglycan from the matrix of articular cartilage.27 Intravenous injection of IL1Ra into these animals inhibited the entry of leucocytes into the synovial lining and joint cavity and blocked the IL1 caused loss of proteoglycan from the articular cartilage.
Patients with active RA have increased plasma concentrations of IL1β (fig 2).7 It has also been found that patients with the highest levels of IL1Ra and lowest levels of IL1β in the synovial fluid had the least troublesome course of Lyme arthritis.28 In addition, studies have shown that animals that overexpress IL1Ra are protected against endotoxin caused death.1

Plasma concentrations of IL1β in controls and patients with active RA.7
Clinical findings also suggest that inhibiting IL1 can retard osteoclast activity (fig 3) and downregulate the production of metalloproteinases. This may have the direct effect of preventing the bone erosion that is seen in RA.29 The results of a trial to examine this possibility are expected shortly.
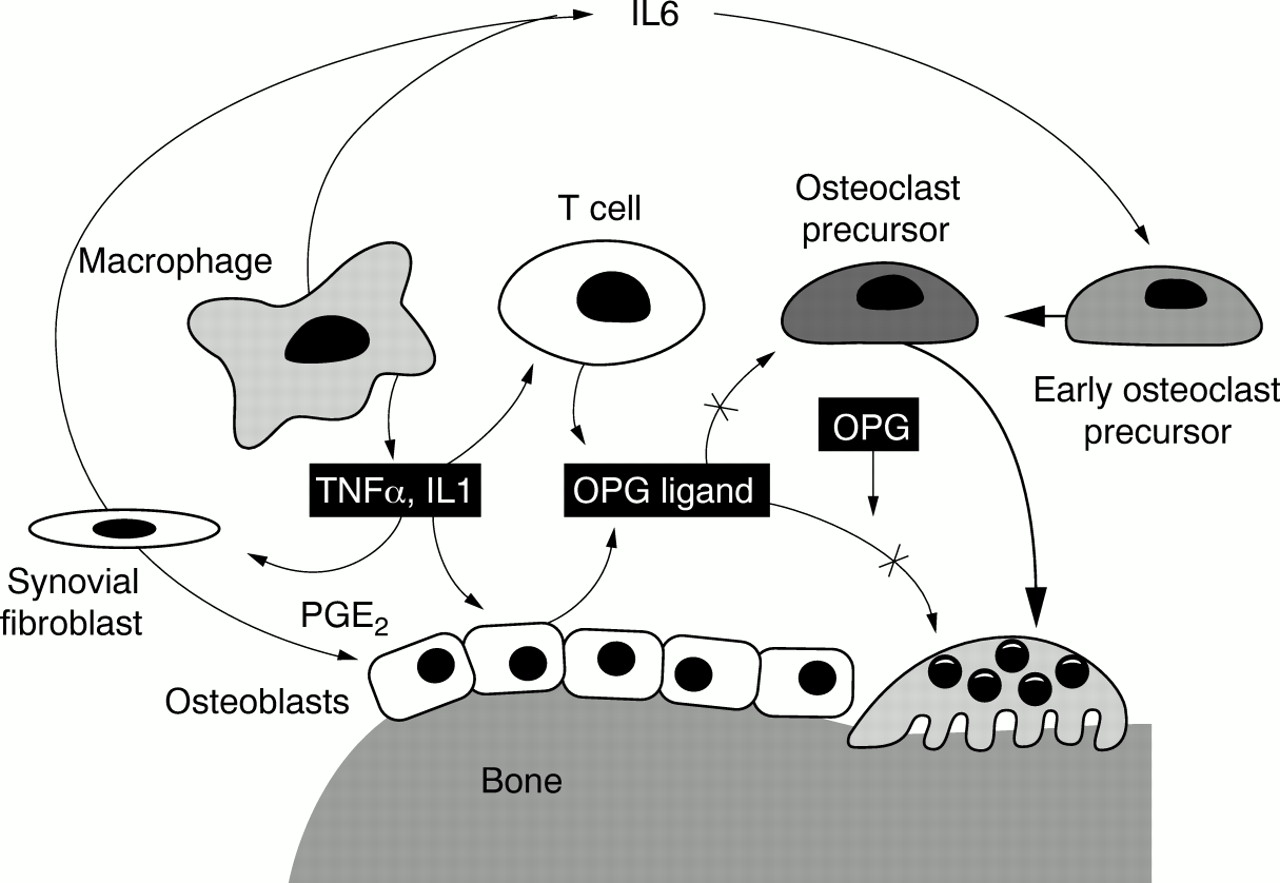
Cytokine regulation of osteoclast differentiation and activation. OPG, osteoprotogerin; PGE2, prostaglandin E2. (Courtesy of M H Schiff).
Intravenous injection of IL1Ra in healthy volunteers presents overwhelming evidence of the cytokine's role as a pure receptor antagonist in the body.2 IL1Ra showed no agonist activity in humans when given at doses a millionfold greater than the concentration of IL1α or IL1β.30 ,31 By occupying the IL1 receptor, IL1Ra effectively stops the IL1 signal transduction that effects the deleterious changes in the synovium and joints in patients with RA (see fig 1).
Clinical experience
Studies over the past 10 years in patients with sepsis and RA have shown the excellent safety profile of IL1Ra. It has been used without serious adverse effects in more than 4500 people, including more than 2000 patients with RA,29 some for as long as five years.
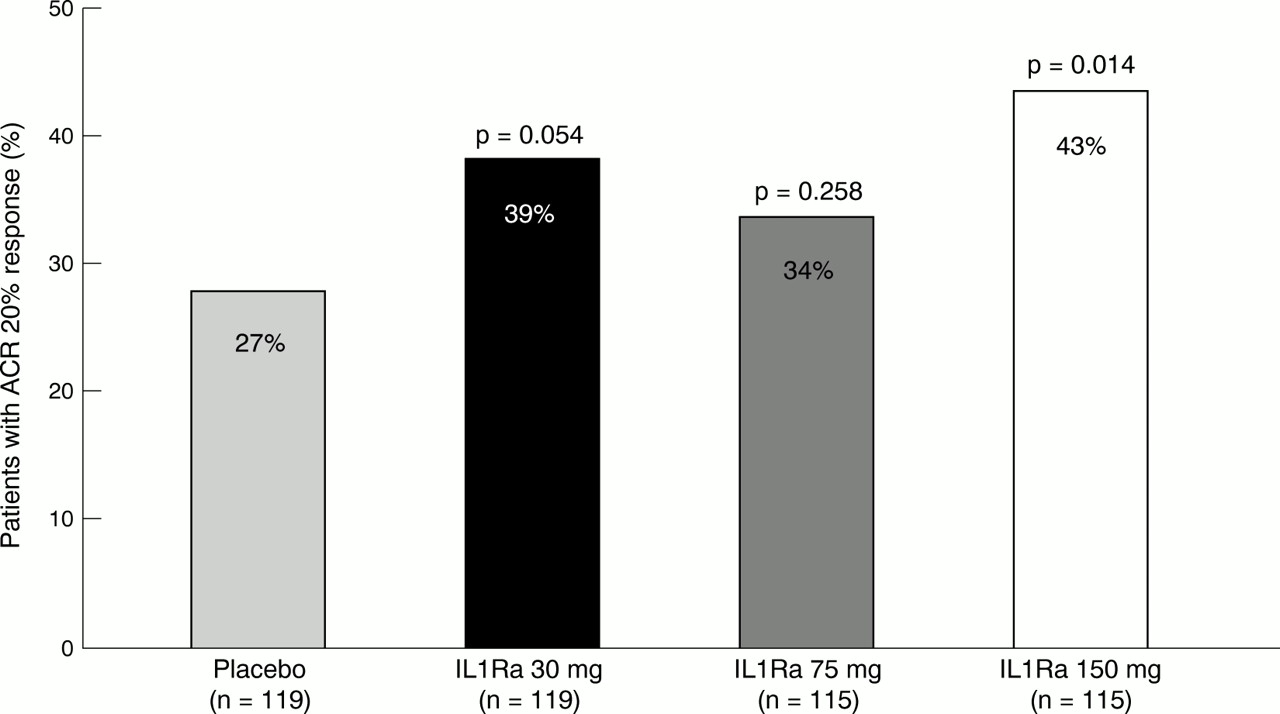
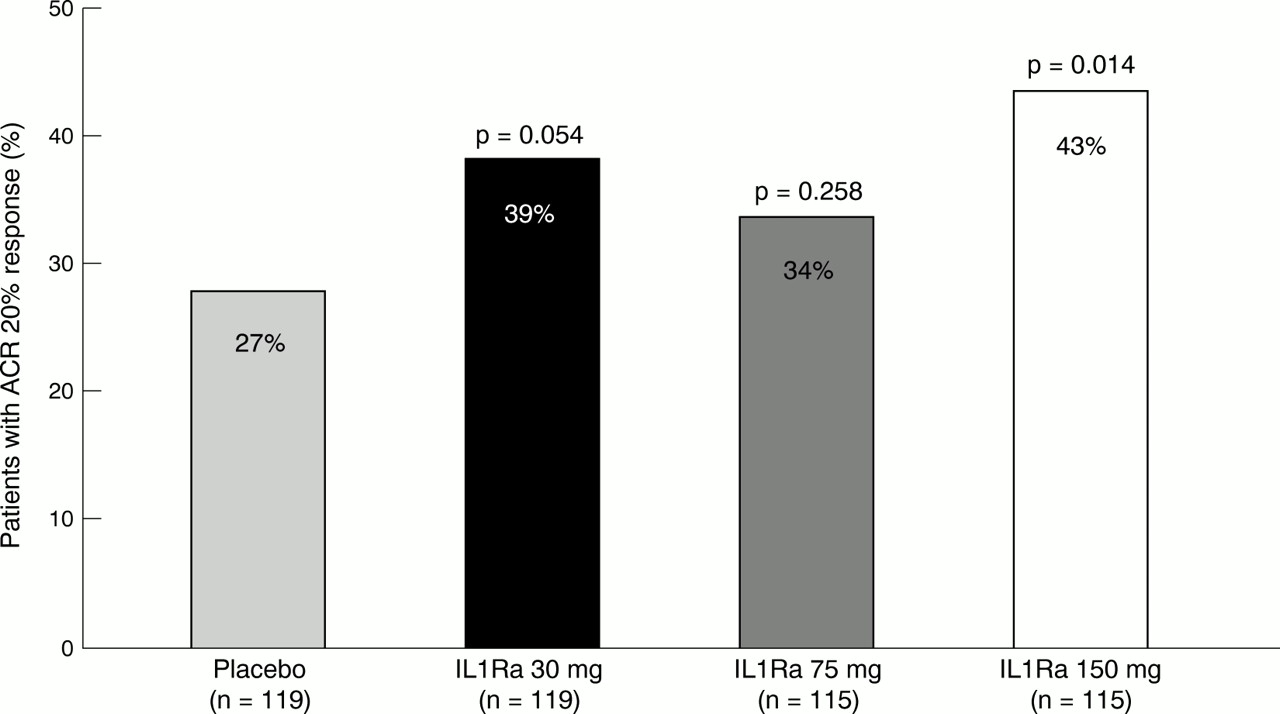
A randomised double blind placebo controlled trial in 472 patients with RA (tables 2 and 3) found that IL1Ra given daily by subcutaneous injection produced a sustained clinical response at week 24, with an American College of Rheumatology (ACR) 20% response seen in 43% of the patients treated with the highest dose, 150 mg (fig 4). The administration of IL1Ra significantly reduced other clinical measures of the disease in these patients as well (p<0.0001 for erythrocyte sedimentation rates and p=0.0009 for the number of tender joints) (fig5, A and B, respectively).32 The 150 mg dose of IL1Ra also significantly decreased the number of swollen joints in patients with moderate to severe RA (p=0.03) compared with placebo (fig 5, C).32 An extension of this trial also showed a continued beneficial effect on the disease (fig 6). In this study, patients with RA who were treated with IL1Ra showed a slowing of radiographic progression in as little as 24 weeks and had a continued benefit with extended treatment for 48 weeks (fig7).
Design of European Monotherapy Study
Patient details in European Monotherapy Study
Clinical response at week 24 in European Monotherapy Study.33

Erythrocyte sedimentation rates (ESRs) (A), inhibition of structural damage by IL1Ra (B) and swollen joint counts (C) in European Monotherapy Study.32

Erythrocyte sedimentation rates (ESRs) in Extension Study of European Monotherapy Study.33

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Assessment of joint damage in Extension Study of European Monotherapy Study.33
IL1Ra has also been studied when given concomitantly with methotrexate.34 In a randomised double blind placebo controlled trial (n=419) of IL1Ra doses of between 0.04 mg/kg/day and 2 mg/kg/day, the 1 mg/kg and 2 mg/kg doses resulted in significant reductions in the signs and symptoms of RA. An ACR 20% response at week 12 was seen in 46% of those treated with 1 mg/kg and in 38% of those treated with 2 mg/kg, which was generally sustained at week 24 (S B Cohen, 63rd Annual Scientific Meeting of the American College of Rheumatology, Boston, 1999). An ACR 20% response was seen in 42% of the patients who completed 24 weeks of treatment with IL1Ra 1 mg/kg/day and in 35% of those who received 2 mg/kg/day, but in only 19% of those given placebo (S B Cohen, 63rd Annual Scientific Meeting of the American College of Rheumatology). IL1Ra was well tolerated, with injection site reactions being the most frequently reported adverse event. The injection site reactions generally occurred within the first 28 days of IL1Ra treatment, with 97% of these transient reactions being mild to moderate. In 87% of those in whom the adverse events occurred there were only one or two such reactions.
Safety of IL1Ra
In the clinical trials to date, IL1Ra has been well tolerated. Injection site reactions have been the most frequently observed adverse event, particularly in those given 1 mg/kg and 2 mg/kg doses. The European Monotherapy Study found injection site reactions to be the most frequent (table 4), and there were no changes in creatinine clearance rates or liver enzyme levels.32
Most common adverse events in European Monotherapy Study
The adverse effect profile of the cytokine modifiers, such as IL1Ra and TNFα antagonists, is superior to that of the other drug classes that are used to treat RA. Furthermore, the safety record of IL1Ra in terms of risk of infection compares favourably with that of the current biological treatments that target TNFα. IL1Ra has shown no evidence of immunosuppression or increased risk of infection or malignancy in controlled clinical trials.29
Conclusion
Stopping the disease process remains the goal of treatment for RA. Recent research has shown this process to include IL1 as pivotal cytokine in initiating disease and the body's natural anti-IL1 response, IL1Ra, to block its effects. Laboratory and animal studies have shown that inhibiting IL1 with either antibodies to IL1 or IL1Ra produces beneficial outcomes. Now, two large well controlled studies in patients with RA have shown that IL1Ra is clinically effective and that it slows progression of bone damage as measured radiographically. Because it is a specific, selective inhibitor of the IL1 pathway, IL1Ra offers an important new treatment for RA that significantly reduces the signs and symptoms of the disease, reduces joint destruction and is safe and well tolerated.
Acknowledgments
This article was developed, in part, from a presentation by Dr Schiff at the Second International Symposium on Advances in Targeted Therapeutics, Miami Beach, Florida, 29 March to 2 April 2000. Dr Schiff has professional relationships with Adventis, Amgen, Bayer, Bristol-Myers Squibb, Centocor, Cypros, Fujisawa, Genelabs, Hoffmann-La Roche, Immunex, Lilly, Merck, Novartis, Parke-Davis, Pfizer, Procter & Gamble, Searle, SmithKline Beecham and Wyeth-Ayerst. This article was made possible, in part, by an unrestricted grant from Amgen Inc.