 Marta G. Cavalcanti
Marta G. Cavalcanti Aline Fernandes Araujo Cunha
Aline Fernandes Araujo Cunha José Mauro Peralta2*
José Mauro Peralta2*- 1Serviço de Doenças Infecciosas e Parasitárias, Hospital Universitário Clementino Fraga Filho, Universidade Federal do Rio de Janeiro, Rio de Janeiro, Brazil
- 2Departmento de Imunologia, Instituto de Microbiologia Paulo de Góes, Universidade Federal do Rio de Janeiro, Rio de Janeiro, Brazil
Like soil-transmitted helminth infections, schistosomiasis is an important neglected tropical disease (NTD) related to poverty with a major impact on public health in developing countries. Diagnosis of active infection is crucial for surveillance of controlled or post-elimination schistosomiasis areas. In addition, the use of conventional diagnostic tools in non-exposed populations (such as travelers) results in misdiagnoses in the prepatent period of infection. Also, the accuracy of standard tests applied in low-endemicity areas (LEAs) decreases after several rounds of treatment. We aimed to determine whether it would be necessary to replace schistosomiasis conventional diagnostic tests such as parasitological methods in LEAs. Also, we evaluate the use of new tools in non-endemic areas. Reliable, cheap and easy-to-use diagnostic tools are needed to respond to the demands of a new era of elimination and eradication of schistosomiasis. To this end, molecular diagnosis—including nucleic acid-based assays (loop-mediated isothermal amplification, polymerase chain reaction) and circulating cathodic and anodic antigen detection tests have become promising strategies. In this review, we attempt to address the use of alternative diagnostic tests for active infection detection and drug-monitoring after specific schistosomiasis treatment.
Introduction
The World Health Organization (WHO) set a high standard: eliminating schistosomiasis until the end of the decade. In 2012's, delegates in the World Health Assembly adopted WHA65.21 resolution which urged the Member States to get involved in plans with achievable targets toward elimination. Endemic countries would also ensure the provision of therapies, being WHO task to elaborate a procedure to evaluate the interruption of schistosomiasis transmission. Also, to achieve this goal, the WHO established partnerships with non-profit organizations participating in initiatives that hopefully will allow morbidity control of schistosomiasis in areas of Sub-Saharan Africa (1–4). The ultimate objective is to decrease the risk of infection in exposed populations, e.g., school-aged children, women, farmers and fishermen in areas of high prevalence. In addition, low endemic areas (LEA) try to achieve this goal: sustainable schistosomiasis control and interruption of transmission in the nearby future (3). Despite the low transmission rates and low parasitic loads, individuals living in LEA are still at risk of infection. Moreover, since even light infections bear a reasonable chance of morbidity, it is essential to increase efforts toward eliminating schistosomiasis from LEAs.
Overall, the main strategies to control or eliminate schistosomiasis transmission include preventive chemotherapy, water sanitation and hygiene (WASH), snail control, and the dissemination of information, education, and communication (IEC) (5). Although most of these approaches are feasible, elimination of schistosomiasis in every transmission area is not simple. In addition, global changes are re-shaping the world map by introducing, establishing and spreading vector-borne diseases like schistosomiasis in previously non-endemic areas (6, 7). Although schistosomiasis is a poverty-related NTD, Schistosoma infection was recently detected in Southern Europe. In the summer of 2013, an autochthonous schistosomiasis outbreak affected travelers from France, Germany and Italy. A hybrid of human and livestock-specific Schistosoma was identified as a causative agent of urogenital schistosomiasis in Corsica, a tourist destination (8).
The emergence of new endemic areas and the persistence of transmission hotspots require the strategies of control and/or elimination to be perfected. As a result, surveillance systems must be able to detect early changes in transmission patterns in endemic areas and the introduction of parasites in formerly non-endemic areas, and strategies must be designed to suppress infection spread. However, the success of schistosomiasis control or elimination in the world depends on how infection is detected.
Schistosoma infection is primarily determined by laboratory testing. After laboratory detection of Schistosoma infection, it is possible to measure the effectiveness of interventions, monitor transmission in endemic areas, detection of recent introduction of the parasite into non-endemic areas and assess the drug response at community and individual levels (9). Thus, it is necessary to have reliable, accurate, and low-cost diagnostic approaches. In LEAs, traditional tests show decreased performance and underestimate infection prevalence both pre-and post-treatment. By contrast, diagnosis of schistosomiasis in non-endemic areas is also difficult for groups of recently infected travelers and immigrants from non-transmission areas. Could changes to the conventional diagnostic approaches remedy the present scenario? The advances and the relevant perspectives in schistosomiasis diagnosis are discussed here.
Conventional Approaches Underestimate Schistosoma Infection Frequency: Implications for the Reliability of Pre-Treatment Diagnoses and Efficiency of Post-Therapy Interventions
Schistosomiasis diagnosis traditionally relies on ova detection in biological specimens. Positive egg-excretion is a marker of active infection. However, the peculiar life cycle of Schistosoma, as well as the complexities involving tissue distribution and excretion of ova makes the diagnosis of active infection far from certain in many scenarios. Dictated by parasite loads and egg production, the host's level of infection ultimately determines the tests' success. Low parasite burden in individuals living in LEAs is associated with decreased accuracy of microscopy before and after treatment (7, 10–12). Adult worms can live for decades, but elderly parasites may have reduced egg production, interfering with egg detection. Also, acquired single gender infections or after use of chemotherapy could explain the absence of egg excretion despite the persistence of infection. A variation in egg excretion and subsequent erroneous diagnosis by an inexperienced technician can mistakenly lead to underestimation of schistosomiasis prevalence or an incorrect evaluation of post-treatment response (13, 14).
Molecular assays—including DNA and antigen detection for immature forms like schistosomula and young adult worms—could help the diagnosis of infection in the prepatent period when eggs have not yet been produced. Schistosoma's biological sub-products, such as schistosome antigens, can be present in the blood and excreted in the urine by a single pair of adult live parasites during very early infection (pre-patent infection) (15–19). Also, schistosome antigens may remain detectable from worm pairs that no longer produce eggs after treatment with praziquantel (PZQ). The presence of urinary antigen in the absence of eggs may indicate a single sex infection or unhealthy, unfertile female or senile worms (10, 19, 20). Fragments of Schistosoma nucleic acids are released during the entire parasitic life cycle in intermediate and definitive hosts (humans), but are also found in the parasites' post-mortem tissue. DNA detection assays have the potential to detect schistosomiasis at day one post-infection (21).
The Decreased Sensitivity of Conventional Tests Changes the Efficiency of Global Schistosomiasis Surveillance for the Detection of Elimination and Leads to Underdiagnoses of Light Infections at the Individual and Community Levels
In resource-limited settings, the need to keep costs low makes the use of parasitological methods such as the Kato-Katz (K-K) technique a favored diagnostic approach in transmission areas. Requirements for K-K sample preparation are usually affordable, although a well-trained technician is necessary for correctly reading the slides and identifying and counting eggs of soil-transmitted helminths (STH) and schistosomes (22). K-K is a quantitative, highly specific method traditionally used for monitoring STH in co-endemic areas, as it also detects hookworm, whipworm, and roundworm eggs as well as schistosome eggs. However, its low sensitivity compromises evaluation after drug administration, which generates large numbers of false negative results in patients with decreased parasitic loads. Also, it is a time-consuming method and requires electricity to be available. Another limitation is the inaccuracy of K-K for diagnosing early infections prior to oviposition (11, 23, 24).
Population-based studies demonstrate that the variability of parasitological test performance can be an important issue (Table 1). In moderate–to-high endemic areas, K-K may have low sensitivities varying from 41.4–83.5%. In LEAs and/or populations with low parasite burden, the K-K technique has sensitivities that may range from 12.5 to 75% (Table 1). As a result, prevalence may be underestimated in those settings. In moderate-to-high endemicity areas, prevalence is as poor as 20.4–94.8% by using the duplicate K-K technique (Table 1). However, in LEAs, prevalence varies from 4.9 to 7.4% and mostly reflects the reference test's decreased accuracy (25–27). Hence, the results indicate that the test sensitivity varies with infection prevalence and, the last one depends highly on “reference test” accuracy (31). For example, in one study in LEA, S. mansoni infection prevalence determined by K-K with a single slide/sample showed a prevalence of 1.9% and a test sensitivity of 62.5%, respectively (30). By increasing the number of slides per sample and/or the number of stool samples examined, prevalence estimation also increases in both moderate-to-high and low endemic areas (25, 30).
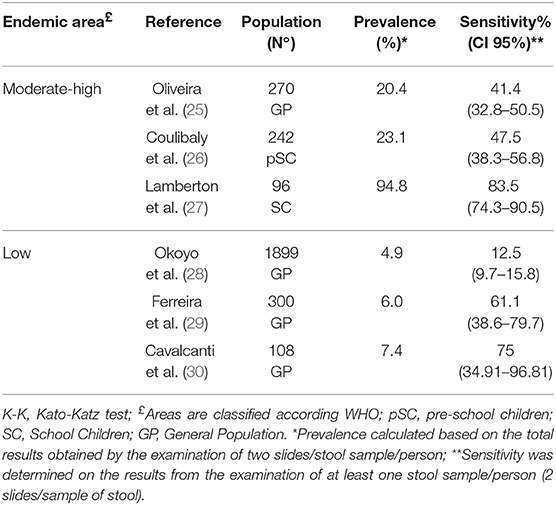
Table 1. Baseline comparative prevalence and sensitivity in high-moderate and low endemicity areas based on Kato-katz test in study populations not submitted to praziquantel treatment.
Since the intensity of infection and prevalence may influence schistosomiasis conventional test sensitivity, it is critical to get better solutions toward diagnosis improvement in areas of low endemicity (2, 7). In Cavalcanti et al. (30), a study performed in LEA assessed schistosomiasis prevalence by using both conventional tests and new diagnostic tools. By using duplicate K-K with a sensitivity of 75% (CI95%: 34.91–96.81), the egg counts varied from 0 to 72 eggs per gram (epg) and the estimated prevalence was 7.41% (Table 1). The results showed that the number of individuals with no egg detection could not be assessed by traditional methods, diagnosis of “real” active schistosomiasis became an issue. The use of a molecular approach in this same area changed the prevalence estimation by demonstrating that 12.96% of the study population had an active infection. Individuals with active infection were composed of 7.41% egg excretors and 21.3% non-egg excretors as determined by K-K and molecular methods, respectively (30). The introduction of molecular methods increases detection of active infection in areas of low, moderate and high endemicity (Tables 2, 3).
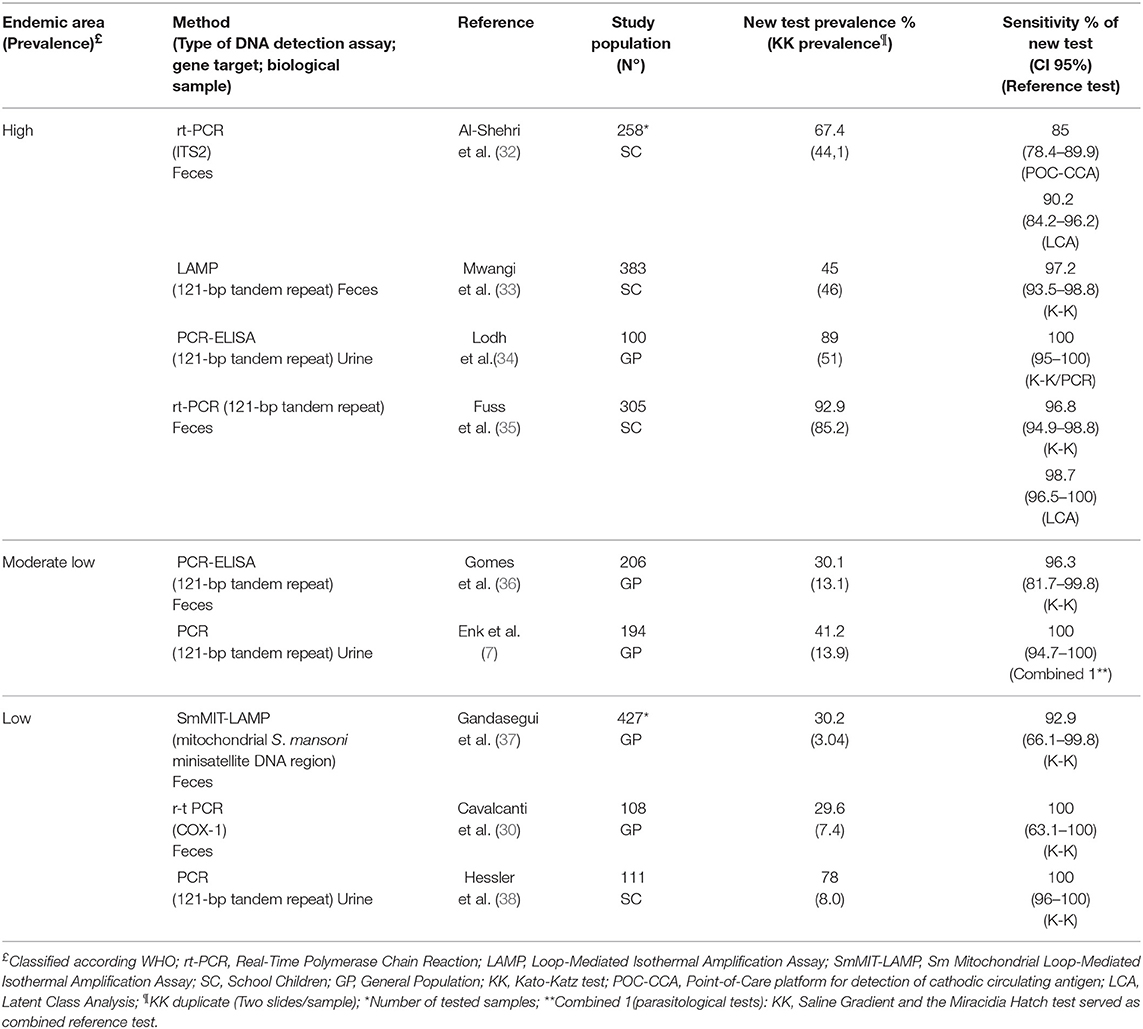
Table 2. Prevalence and sensitivity values determined by Schistosoma mansoni DNA detection assays before treatment in high, moderate, and low endemicity areas.
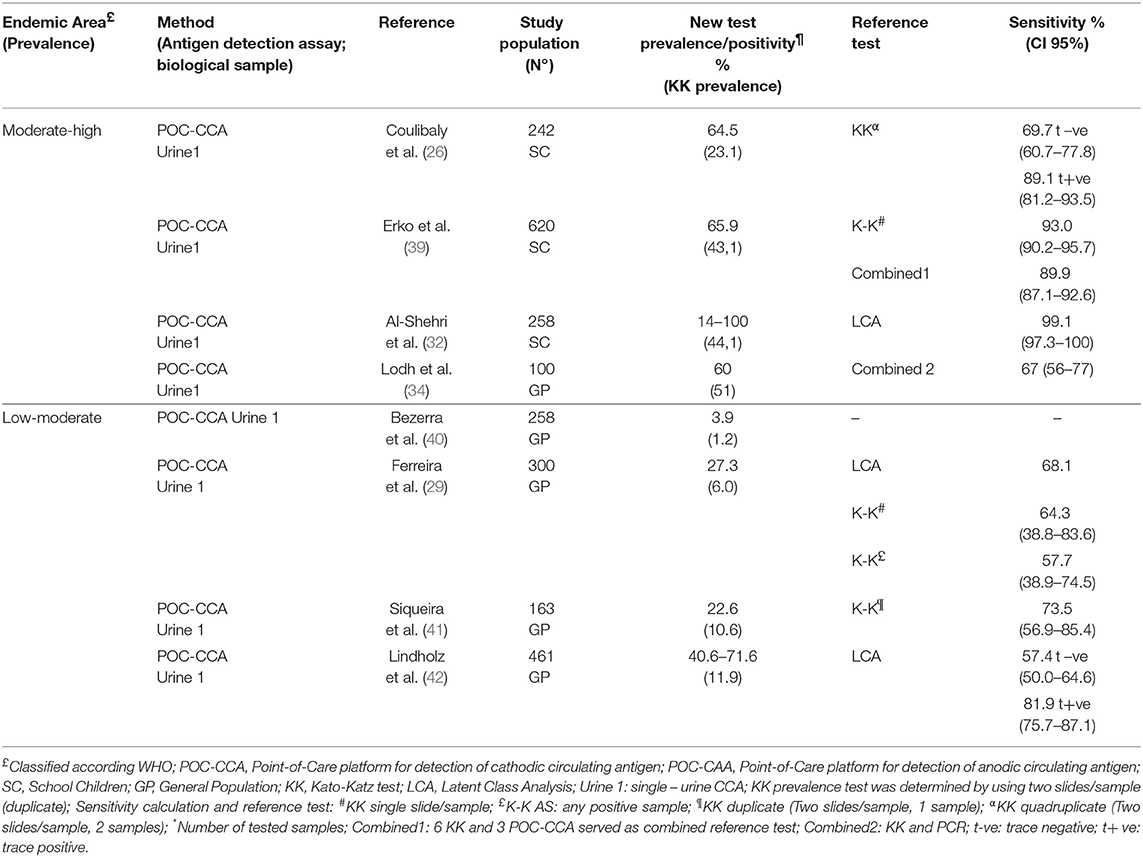
Table 3. Prevalence and sensitivity values determined by antigen detection assays in high, moderate and low endemicity areas.
Evaluation of drug response by parasitological methods at the community level in LEAs is unreliable for a long time (9, 13, 28–30, 43). More than a decade has passed since studies pointed out the progressive loss of sensitivity in parasitological methods with decreasing prevalence and an associated difficult in measuring treatment efficacy (44). Teles et al. (45) demonstrated a progressive reduction of schistosomiasis prevalence from 3.4 to 1.8% in the 3-year observation period in an LEA. The prevalence rate decreased sharply after treatment. However, some egg-positive cases remained detectable after treatment, with no change in parasite load. Since only an egg-based assay was used, non-egg excretors were not diagnosed and treated. Diagnosis based on egg detection does not reveal residual infections with low- or no-egg excretion, only those infections with a persistent parasite burden (2). Other studies presented similar data, demonstrating the failure to distinguish the status of control vs. elimination of schistosomiasis in transmission areas based exclusively on egg detection, as shown in Table 1.
Decreased test sensitivity jeopardizes surveillance of endemic areas by compromising the mapping and monitoring hotspots of transmission and accurately assessing the impact of interventions like preventive chemotherapy use, sanitation and health education (9). However, the limitations of conventional methods are not restricted to transmission areas. At institutional settings in non-endemic areas, both diagnosis and clinical management of individuals with a history of exposure to contaminated water could be a problem (43). For example, the diagnosis of acute schistosomiasis during the prepatent period, with low parasite burden or an absence of egg excretion during chronic infection in travelers, immigrants and refugees often leads to misdiagnoses (23). Low-cost alternatives, like egg enrichment methods, such as HelmintexTM, have potential to improve egg detection. By using magnetic beads to trap eggs in a magnetic field, HelmintexTM enhances microscopic efficacy. It is a very sensitive (100%) technique to detect Schistosoma infection in individuals with as few as 1.3 epg of feces (46). The data suggest that the method could be a reliable alternative to enhance the diagnostic performance of egg-detection assays in LEAs and for the diagnosis of infections with low worm load (25). However, it is a laborious test, and in areas of co-endemicity it may not distinguish Schistosoma species. Also, species-specific differences in eggs' ability to bind to the magnetic beads must be determined for its use in urinary schistosomiasis and “new” infections induced by hybrid species (9). More extensive studies should be conducted.
Also, during chronic infections, low parasite burden can remain unnoticed in asymptomatic individuals. However, in individuals with advanced disease and/or atypical presentations, parasitological tests and even tissue sample analysis can miss active infections (43). As a result, schistosomiasis diagnosis by egg detection in particular groups—like travelers, immigrants and refugees—is underdiagnosed and clinical management becomes restricted.
The use of conventional tests for the diagnosis of schistosomiasis in endemic and non-endemic areas seems to have reached a crossroad; reliable new diagnostic approaches are urgently needed.
Non-Traditional Diagnostic Approaches Currently Available May Change Schistosomiasis Management Before and After Treatment in LEAs and Non-Endemic Areas
Although egg detection remains as a reference for the diagnosis of schistosomiasis at community and individual levels, diagnostic assays for DNA and antigen detection can overcome the limitations of parasitological tests. DNA detection assays are mostly in-house tests, although some are becoming commercially available (10). PCR-based assays detect DNA of Schistosoma in stool, serum, plasma, urine, and tissue, demonstrating high sensitivity and specificity (Table 2) (7, 36, 47).
Studies carried out in high, moderate and low endemicity areas suggest that DNA-based assays are reliable tools for schistosomiasis diagnosis and for monitoring treatment response (32–38, 47). In the field, PCR-based assays are more sensitive than parasitological tests regardless of the area endemicity (Table 2). PCR-based methods demonstrated higher sensitivities (80–100%), and—in LEAs— resulted in prevalence values that were higher than those of the K-K technique (Table 2). Amplification of the S. mansoni 121-bp tandem-repeat sequence by a conventional PCR test in one fecal sample showed a higher prevalence than K-K analysis of three stool samples from individuals living in LEAs (Table 2). By using real-time PCR targeting the COX-1 target region, Cavalcanti et al. (30) demonstrated that Schistosomiasis mansoni prevalence was 12.96% compared to K-K estimated prevalence of 7.4% in a low endemicity setting (Table 2). DNA amplification was demonstrated in up to 100% of the egg excretors and 85.7–94.7% of serologically-reactive individuals. Loop-mediated isothermal amplification (LAMP) is a cheaper and simpler version of a molecular detection assay. LAMP is user-friendly and does not require a thermocycler (10). In LEAs, LAMP showed superior performance compared to K-K (Table 2). There is growing evidence that LAMP might be an affordable diagnostic approach in low-income settings. A small study in Brazil indicated that LAMP detected almost 10 times more active infections of schistosomiasis in humans than a duplicate K-K smear. The test detected 92.31% of the egg excretors and 24.83% of K-K negative individuals living in a LEA (37).
Robust data demonstrated that PCR-based methods are also reliable approaches to monitoring response to treatment (Table 2). In areas of high prevalence and infection intensity, at 2 months after PZQ treatment, single real-time PCR detected 69, 3% of S. haematobium infected children vs. 22.8% demonstrated by microscopy (14). After 18 month follow up, real-time PCR diagnosed 78.9% of positive samples in contrast to 63.2 to 68.1% detected by microscopy. In LEAs, persistent DNA amplification can be demonstrated in up to 50% of previously treated individuals with schistosomiasis mansoni 6 months after a single round of PZQ therapy, while no K-K positivity was found [Supplementary Material, (30)]. In LEAs, “false” rapid clearance of egg excretion until 6 months post-therapy may occur while amplification of DNA persists (30). However, during a 2-year long follow up, results showed that both egg and DNA detection had similar performance in a study population of pretreated individuals [Supplementary Material, (30)].
By using PCR-based assays to assess PZQ cure rates, rt-PCR demonstrated that 24% and 18.2% of the treated individuals with one and two rounds of therapy, respectively, remained positive after treatment (30). The results suggest that persistent DNA amplification after PZQ use may be a more suitable indicator of cure.
PCR-based assays detect Schistosoma DNA in stool, serum, plasma, urine and tissue, demonstrating high sensitivity and specificity (Table 2) (38, 48). DNA detection assays are also useful in cases of co-infection with different Schistosoma species and soil-transmitted helminths (STHs); they have potential use in both STH and schistosomiasis control programs (38, 49–51). Multiplex diagnostic platforms allow the diagnosis of multiple STHs and Schistosoma, and may be a cheaper alternative for low-income areas (49).
Egg-negative infections missed by conventional methods can also be revealed by DNA detection assays in travelers, immigrants and refugees leaving non-endemic areas (48). Based on a small case series, real-time PCR for DNA detection in serum was shown to surpass K-K and serology and improve the diagnosis of acute infections in egg-negative and/or serologically inconclusive individuals (52). One crucial pitfall is the amplification of certain Schistosoma target genes. In the same case series, the authors discuss how a repetitive 121-bp DNA fragment represents a little more than 10% of the S.mansoni genome. Its use as a target sequence in real-time PCR might reduce test sensitivity in infections other than S. mansoni, such as S. haematobium and S. japonicum. In situations of co-endemicity or hybrid introduction, the test could have lower performance.
Antigen Detection Might Play a New Role in Schistosomiasis Diagnosis
Lately, different assays for the detection of Schistosoma biological sub-products became investigated as reliable alternative to ova detection. Antigen detection was made possible through the development of immunodiagnostic assays in the 1980s (53, 54). Enzymatic (ELISA) assays to detect Schistosoma gut-associated polysaccharides—CCA and CAA—turned out to be a promising diagnostic approach (10, 55). In the 1990s, study in area of high endemicity showed that immunodiagnostic assays (e.g., ELISA) for detection of CAA and CCA in serum and urine demonstrated active S. mansoni infection in 94, 83, and 95% of the populations studied, of which 91% were positive by stool exam. Data showed that CCA and CAA levels correlated with egg counts, although these antigens could also be detected in egg-negative individuals. ELISA for CCA and CAA also demonstrated higher sensitivities than a single stool exam (56). But when testing the applicability of CAA and CCA detection in a low endemicity area, results showed that sensitivities for CAA and CCA using ELISA were 23% and 17%, in serum and 3 and 28% in urine samples, respectively. In contrast, egg detection was positive in 29% of the examined cases in the same area. Based on this, the study suggested that the detection of CCA in urine and CAA in serum might be a suitable diagnostic approach for schistosomiasis, and may be used in conjunction with the parasitological tests to determine the prevalence and intensity of Schistosoma infection in LEAs (57). At this time, CCA and CAA detection assays use were limited. But, a huge step was taken after lateral flow (LF) based assays became available by changing the scenario of schistosomiasis diagnosis (58, 59).
In the era of rapid tests for the diagnosis of many infectious diseases, LF-based assays for CAA and CCA detection have the potential to revolutionize the field of schistosomiasis diagnosis. Schistosoma antigens are detectable in serum and urine samples. CAA-detection based assay uses luminescent quantitative up-converting phosphor (UCP) reporter particles (UCP-LF). But, the assay is not available in the market currently. The point-of-care (POC) test for CCA detection has a commercial version (10, 60). Detection of Schistosoma species is highly variable. POC-CCA, e.g., is more reliable for S. mansoni than for S.haematobium detection, although it can also detect S. japonicum active infections (59). By contrast, UCP-LF CAA may be a promising diagnostic tool in urinary schistosomiasis. A study carried out in Zanzibar of 2,067 randomly selected school children from 16 schools evaluated UCP-LF CAA test accuracy in areas with prevalences ranging from <2 to 10%. By using latent Bayesian analyses (LBA), sensitivity of UCP-LF CAA was estimated to be 97% (95% CI: 91–100%), and suggested a 14% prevalence. Results showed that high sensitivity and reasonable specificity values assured that the UCP-LF CAA test could be a reliable approach for diagnosis of urogenital schistosomiasis in LEAs attempting complete elimination (61). In non-endemic areas, results from a study of 81 serology-positive individuals demonstrated that UCP-LF CAA confirmed active infections in 56/81 individuals exposed to contaminated waters (62). Also, acute infection was diagnosed before oviposition, since CAA levels were detectable 4 weeks after exposure. CAA levels become measurable before detection of Schistosoma-specific antibodies. Moreover, the study also detected different CAA concentrations in the sera of travelers and migrants, with higher CAA levels demonstrated in migrant serum samples. Post-treatment, a sharp decrease of CAA levels was demonstrated. The results suggest that a UCP-LF CAA serum assay would be a reliable test for diagnosing light infections in non-endemic settings (62).
Field studies presented promising results, and the diagnosis of active schistosomiasis was made easy by the commercial version of CCA manufactured by Rapid Test Diagnosis (Pretoria, South Africa). In high and moderate endemic areas, POC-CCA showed higher accuracy than the K-K technique (26, 39). The results also indicated that the intensity of the POC-CCA reaction correlated with the number of eggs (26). By contrast, results also showed that antigen daily variability was frequently observed in school children as well as antigen persistence in the absence of egg excretion after PZQ treatment (26). In Table 3, POC-CCA sensitivity ranged from 67 to 99.1% when applied in areas of high and moderate endemicity. However, studies performed in populations with light infections and/or LEAs did not experience the unquestionable success of the high and moderate endemicity areas (63). The accuracy of POC-CCA is reduced as a result of an increased number of false positive reactions (Table 3) (20). Mostly, the presence of very weak reactions—called trace positives—overestimates the estimation of active infections. In LEAs, the trace reactivity in POC-CCA is poorly associated with positivity in other confirmatory tests (64). However, it remains undetermined whether the data showing trace results may represent accurate positive reactions and instead should confirm active schistosomiasis (65).
In non-endemic areas, antigen-detection assays' accuracy must be further investigated. In a retrospective study of immigrants and refugees, CCA showed low sensitivity when compared to microscopy, ELISA, Western blot and immune-chromatographic tests (66). Although some authors agree with the usefulness of POC-CCA as a tool for detecting active infection in special populations like refugees, use of the test after treatment follow up is still disappointing in this group (67).
Discussion: About the Controversies, Current Research Gaps and Potential Future Developments in the Field
The main question in an era of control and elimination of Schistosoma infection in a transmission areas is: can the diagnosis of schistosomiasis in endemic settings rely on one test? Although the K-K technique has been applied over the years, several adaptations of the method did not improve its skill in diagnosing schistosomiasis. At the moment, ideal tests are inexistent, and gold standard or reference tests in schistosomiasis diagnosis are missing in LEAs. Limitations of the K-K technique include loss of test sensitivity, low reproducibility, and it is a time-consuming technique even though it has a lower cost compared to molecular tests. Applicability of the K-K in LEAs has become practically useless since a low parasite burden is often hidden within individuals with no egg excretion. Also, K-K performance for diagnosis of multiple parasitic infections in co-endemic areas becomes poor when parasitological tests are used. In institutional settings, primary healthcare of travelers, immigrants, and refugees is compromised by stool exam low performance in light infections. As a marker of drug response or complete cure, the parasitological tests may underestimate the number of treatment failures to PZQ (non-responders) among individuals living in areas of persistent transmission (11).
Since diagnosis limited to conventional tests compromises the detection of active schistosomiasis, it is time to consider new approaches. In the case of S.mansoni, the substitution of DNA or antigen detection assays for stool exam has been considered before (68). Both of the molecular detection assays uncover active infections in both egg excretors and non-excretors. DNA- and antigen-based assays are gradually showing increased potential as markers of active infection in endemic and non-endemic areas. DNA detection assays seem to be an eligible tool for assessing response to therapy in transmission and non-endemic areas. However, superior performance can be seen when molecular approaches are used as a single confirmatory test in both endemic and non-endemic areas. Inferior performances by DNA amplification techniques may be the result of a poor choice of target gene amplification regions for the species under investigation. Also, its universality is debatable under this argument: the costs of DNA-based assays in low-income settings can be 10 times more expensive than the alternatives (10). One possible solution to drop the costs could be the use of multiplex platforms by the Global Polio Laboratory Network (GPLN) in areas of STH and SCH co-endemicity (49). The GPLN already performs molecular diagnosis for poliovirus and other enterovirus infections in 16 labs across Africa. By using multiplex platforms for the diagnosis of STH and SCH, detection of multiple parasitic active infections might be improved while assessment of drug response in transmission areas is kept to a minimal cost. Antigen detection assays are quickly becoming the new reference test of preference in areas of schistosomiasis transmission. However, standardization of the assays, as well as increased sensitivity and specificity and increased availability of multiple commercially affordable tests, are essential issues to be addressed by national schistosomiasis control programs.
Overall, diagnostic tests unveil different aspects of the Schistosoma biology. Detection of Schistosoma and its subproducts may not overlap during the parasite cell cycle. Distinct from egg detection, the kinetics of Schistosoma antigens and DNA are still poorly established during Schistosoma maturity. In budget-limited national programs, it is fundamental to have an accurate, reliable, easy-to-use, and cheap diagnostic tool available to diagnosis schistosomiasis. However, the use of a single tool might restrict the management of Schistosoma infections at community and institutional levels. Hence, adoption of multiple diagnostic approaches should be considered in areas of low endemicity.
Conclusion
Evidence of the necessity of settling the new options for the detection of active schistosomiasis is overwhelming. However, it appears more research must be conducted before a final decision is made regarding the total substitution of the conventional tests such as parasitological assays.
Author Contributions
MC and JP: the conception and design of the work. MC and AC: performed the literature review. MC and JP: contributed to draft manuscript editing/reviewing. All authors contributed to the revisions and approved the final version of the manuscript.
Funding
JP was supported by the Brazillian Agency CNPq (Conselho Nacional de Pesquisa e Desenvolvimento).
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. WHO. Neglected Tropical Diseases. Available online at https://www.who.int/neglected_diseases/Schistosomiasis_wha65/en/ (accessed May 28, 2012).
2. Colley DG, Andros TS, Campbell CH Jr. Schistosomiasis is more prevalent than previously thought: what does it mean for public health goals, policies, strategies, guidelines and intervention programs? Infect Dis Poverty. (2017) 6:63. doi: 10.1186/s40249-017-0275-5
3. WHO. Schistosomiasis. (2018). Available online at https://www.who.int/neglected_diseases/schistosomiasis_zanzibar_2012/en/ (accessed March 7, 2012).
4. Bill Melinda Gates Foundation. Fight Against Neglected Diseases Sets Sights on Parasites Transmitted by Livestock. Available online at https://www.gatesfoundation.org/search#q/k=Schistosomiasis (accessed July 17, 2012).
5. Tian-Bi YT, Ouattara M, Knopp S, Coulibaly JT, Hürlimann E, Webster B, et al. Interrupting seasonal transmission of Schistosoma haematobium and control of soil-transmitted helminthiasis in northern and central Côte d'Ivoire: a SCORE study protocol. BMC Public Health. (2018) 18:186. doi: 10.1186/s12889-018-5044-2
6. Calvo-Cano A, Cnops L, Huyse T, van Lieshout L, Pardos J, Valls ME, et al. A case of urogenital human schistosomiasis from a non-endemic area. PLoS Negl Trop Dis. (2015) 9:e0004053. doi: 10.1371/journal.pntd.0004053
7. Enk MJ, Oliveira e Silva G, Rodrigues NB. Diagnostic accuracy and applicability of a PCR system for the detection of Schistosoma mansoni DNA in human urine samples from an endemic area. PLoS ONE. (2012) 7:e38947. doi: 10.1371/journal.pone.0038947
8. Boissier J, Grech-Angelini S, Webster BL, Allienne JF, Huyse T, Mas-Coma S, et al. Outbreak of urogenital schistosomiasis in Corsica (France): an epidemiological case study. Lancet Infect Dis. (2016) 16:971–9. doi: 10.1016/S1473-3099(16)00175-4
9. Cavalcanti MG, Peralta JM. Investment on new technologies for diagnosis of schistosomiasis is justified in the era of Schistosoma elimination? Contagion Live. (2018) 3:18–19. Available online at: https:/www.contagionlive.com/publications/contagion/2018/june/is-investment-in-new-tchnologies-for-diagnosing-schistosomiasis-justified-in-an-era-of-schistosomiasis-elimination (accessed June 2018).
10. Ajibola O, Gulumbe BH, Eze AA, Obishakin E. Tools for detection of schistosomiasis in resource limited settings. Med Sci. (2018) 6:E39. doi: 10.3390/medsci6020039
11. Cavalcanti MG, Silva LF, Peralta RH, Barreto MG, Peralta JM. Schistosomiasis in areas of low endemicity: a new era in diagnosis. Trends Parasitol. (2013) 29:75–82. doi: 10.1016/j.pt.2012.11.003
12. Ibironke OA, Phillips AE, Garba A, Lamine SM, Shiff C. Diagnosis of Schistosoma haematobium by detection of specific DNA fragments from filtered urine samples. Am J Trop Med Hyg. (2011) 84:998–1001. doi: 10.4269/ajtmh.2011.10-0691
13. Kongs A, Marks G, Verlé P, Van der Stuyft P. The unreliability of the Kato-Katz technique limits its usefulness for evaluating S. mansoni infections. Trop Med Int Health. (2001) 6:163–9. doi: 10.1046/j.1365-3156.2001.00687.x
14. Vinkeles Melchers NV, van Dam GJ, Shaproski D, Kahama AI, Brienen AE, Vennervald BJ, et al. Diagnostic performance of Schistosoma real-time PCR in urine samples from Kenyan children infected with Schistosoma haematobium: day-to-day variation and follow-up after praziquantel treatment. PLoS Negl Trop Dis. (2014) 8:e2807. doi: 10.1371/journal.pntd.0002807
15. Deelder AM, van Zeyl RJ, Fillié YE, Rotmans JP, Duchenne W. Recognition of gut-associated antigens by immunoglobulin M in the indirect fluorescent antibody test for Schistosomiasis mansoni. Trans R Soc Trop Med Hyg. (1989) 83:364–7. doi: 10.1016/0035-9203(89)90506-3
16. Gundersen SG, Ravn J, Haagensen I. Early detection of circulating anodic antigen (CAA) in a case of acute Schistosomiasis mansoni with Katayama fever. Scand J Infect Dis. (1992) 24:549–52. doi: 10.3109/00365549209052643
17. van Dam GJ, Bogitsh BJ, van Zeyl RJ, Rotmans JP, Deelder AM. Schistosoma mansoni: in vitro and in vivo excretion of CAA and CCA by developing schistosomula and adult worms. J Parasitol. (1996) 82:557–64. doi: 10.2307/3283780
18. Sanya RE, Muhangi L, Nampijja M, Nannozi V, Nakawungu PK, Abayo E, et al. Schistosoma mansoni and HIV infection in a Ugandan population with high HIV and helminth prevalence. Trop Med Int Health. (2015) 20:1201–8. doi: 10.1111/tmi.12545
19. Corstjens PLAM, Hoekstra PT, de Dood CJ, van Dam GJ. Utilizing the ultrasensitive Schistosoma up-converting phosphor lateral flow circulating anodic antigen (UCP-LF CAA) assay for sample pooling-strategies. Infect Dis Poverty. (2017) 6:155. doi: 10.1186/s40249-017-0368-1
20. Haggag AA, Rabiee A, Abd Elaziz KM, Campbell CH, Colley DG, Ramzy RMR. Thirty-day daily comparisons of kato-katz and CCA assays of 45 Egyptian children in areas with very low prevalence of Schistosoma mansoni. Am J Trop Med Hyg. (2019) 100:578–83. doi: 10.4269/ajtmh.18-0829
21. Kato-Hayashi N, Leonardo LR, Arevalo NL, Tagum MN, Apin J, Agsolid LM, et al. Detection of active schistosome infection by cell-free circulating DNA of Schistosoma japonicum in highly endemic areas in Sorsogon Province, the Philippines. Acta Trop. (2015) 141(Pt B):178–83. doi: 10.1016/j.actatropica.2014.05.003
22. WHO. Action against Worms. Are you Deworming? Available online at www.who.int/intestinal_worms/resources/AAW_4_en.pdf (accessed January 2004).
23. Grenfell RF, Martins W, Drummond SC, Antunes CM, Voieta I, Otoni A, et al. Acute schistosomiasis diagnosis: a new tool for the diagnosis of schistosomiasis in a group of travelers recently infected in a new focus of Schistosoma mansoni. Rev Soc Bras Med Trop. (2013) 46:208–13. doi: 10.1590/0037-8682-0064-2012
24. Mationg MLS, Gordon CA, Tallo VL, Olveda RM, Alday PP, Reñosa MDC, et al. Status of soil-transmitted helminth infections in schoolchildren in Laguna Province, the Philippines: determined by parasitological and molecular diagnostic techniques. PLoS Negl Trop Dis. (2017) 11:e0006022. doi: 10.1371/journal.pntd.0006022
25. Oliveira WJ, Magalhães FDC, Elias AMS, de Castro VN, Favero V, Lindholz CG, et al. Evaluation of diagnostic methods for the detection of intestinal schistosomiasis in endemic areas with low parasite loads: saline gradient, Helmintex, Kato-Katz and rapid urine test. PLoS Negl Trop Dis. (2018) 12:e0006232. doi: 10.1371/journal.pntd.0006232
26. Coulibaly JT, N'Gbesso YK, Knopp S, N'Guessan NA, Silué KD, van Dam GJ, et al. Accuracy of urine circulating cathodic antigen test for the diagnosis of Schistosoma mansoni in preschool-aged children before and after treatment. PLoS Negl Trop Dis. (2013) 7:e2109. doi: 10.1371/journal.pntd.0002109
27. Lamberton PH, Kabatereine NB, Oguttu DW, Fenwick A, Webster JP. Sensitivity and specificity of multiple Kato-Katz thick smears and a circulating cathodic antigen test for Schistosoma mansoni diagnosis pre- and post-repeated-praziquantel treatment. PLoS Negl Trop Dis. (2014) 8:e3139. doi: 10.1371/journal.pntd.0003139
28. Okoyo C, Simiyu E, Njenga SM, Mwandawiro C. Comparing the performance of circulating cathodic antigen and Kato-Katz techniques in evaluating Schistosoma mansoni infection in areas with low prevalence in selected counties of Kenya: a cross-sectional study. BMC Public Health. (2018) 18:478. doi: 10.1186/s12889-018-5414-9
29. Ferreira FT, Fidelis TA, Pereira TA, Otoni A, Queiroz LC, Amâncio FF, et al. Sensitivity and specificity of the circulating cathodic antigen rapid urine test in the diagnosis of Schistosomiasis mansoni infection and evaluation of morbidity in a low- endemic area in Brazil. Rev Soc Bras Med Trop. (2017) 50:358–64. doi: 10.1590/0037-8682-0423-2016
30. Cavalcanti MG, Silva LF, Macedo HW, Peralta RHS, Igreja RP, Barreto MGM, et al. Real-time PCR improves detection of active infection in human feces and treatment failure following multiple chemotherapeutic rounds in Schistosoma mansoni low endemic área. Ann Clin Pathol. (2016) 2:1092–100. Available online at: https://www.researchgate.net/publication/327285969_Real-Time_PCR_Improves_Detection_of_Active_Infection_in_Human_Feces_and_Treatment_Failure_Following_Multiple_Chemotherapeutic_Rounds_in_Schistosoma_mansoni_Low-Endemic_Area.
31. Leeflang MM, Rutjes AW, Reitsma JB, Hooft L, Bossuyt PM. Variation of a test's sensitivity and specificity with disease prevalence. CMAJ. (2013) 185:E537–44. doi: 10.1503/cmaj.121286
32. Al-Shehri H, Koukounari A, Stanton MC, Adriko M, Arinaitwe M, Atuhaire A et al. Surveillance of intestinal schistosomiasis during control: a comparison of four diagnostic tests across five Ugandan primary schools in the Lake Albert region. Parasitology. (2018) 21:1–8. doi: 10.1017/S003118201800029X
33. Mwangi IN, Agola EL, Mugambi RM, Shiraho EA, Mkoji GM. Development and evaluation of a loop-mediated isothermal amplification assay for diagnosis of Schistosoma mansoni infection in faecal samples. J Parasitol Res. (2018) (2018) 2018:1267826. doi: 10.1155/2018/1267826
34. Lodh N, Mwansa JC, Mutengo MM, Shiff CJ. Diagnosis of Schistosoma mansoni without the stool: comparison of three diagnostic tests to detect Schistosoma [corrected] mansoni infection from filtered urine in Zambia. Am J Trop Med Hyg. (2013) 89:46–50. doi: 10.4269/ajtmh.13-0104
35. Fuss A, Mazigo HD, Tappe D, Kasang C, Mueller A. Comparison of sensitivity and specificity of three diagnostic tests to detect Schistosoma mansoni infections in school children in Mwanza region, Tanzania. PLoS ONE. (2018) 13:e0202499. doi: 10.1371/journal.pone.0202499
36. Gomes LI, Dos Santos Marques LH, Enk MJ, de Oliveira MC, Coelho PM, Rabello A. Development and evaluation of a sensitive PCR-ELISA system for detection of schistosoma infection in feces. PLoS Negl Trop Dis. (2010) 4:e664. doi: 10.1371/journal.pntd.0000664
37. Gandasegui J, Fernández-Soto P, Muro A, Simões Barbosa C, Lopes de Melo F, Loyo R, et al. A field survey using LAMP assay for detection of Schistosoma mansoni in a low-transmission area of schistosomiasis in Umbuzeiro, Brazil: assessment in human and snail samples. PLoS Negl Trop Dis. (2018) 12:e0006314. doi: 10.1371/journal.pntd.0006314
38. Hessler MJ, Cyrs A, Krenzke SC, Mahmoud ES, Sikasunge C, Mwansa J, et al. Detection of duo-schistosome infection from filtered urine samples from school children in Zambia after MDA. PLoS ONE. (2017) 12:e0189400. doi: 10.1371/journal.pone.0189400
39. Erko B, Medhin G, Teklehaymanot T, Degarege A, Legesse M. Evaluation of urine-circulating cathodic antigen (Urine-CCA) cassette test for the detection of Schistosoma mansoni infection in areas of moderate prevalence in Ethiopia. Trop Med Int Health. (2013) 18:1029–35. doi: 10.1111/tmi.12117
40. Bezerra FSM, Leal JKF, Sousa MS, Pinheiro MCC, Ramos AN Jr., Silva-Moraes V, et al. Evaluating a point-of-care circulating cathodic antigen test (POC-CCA) to detect Schistosoma mansoni infections in low endemic area in north-eastern Brazil. Acta Trop. (2018)182:264–70. doi: 10.1016/j.actatropica.2018.03.002
41. Siqueira LM, Couto FF, Taboada D, Oliveira ÁA, Carneiro NF, Oliveira E, et al. Performance of POC-CCA® in diagnosis of schistosomiasis mansoni in individuals with low parasite burden. Rev Soc Bras Med Trop. (2016) 49:341–7. doi: 10.1590/0037-8682-0070-2016
42. Lindholz CG, Favero V, Verissimo CM, Candido RRF, de Souza RP, Dos Santos RR, et al. Study of diagnostic accuracy of Helmintex, Kato-Katz, and POC-CCA methods for diagnosing intestinal schistosomiasis in Candeal, a low intensity transmission area in northeastern Brazil. PLoS Negl Trop Dis. (2018) 12:e0006274. doi: 10.1371/journal.pntd.0006274
43. Cavalcanti MG, Araújo-Neto JM, Peralta JM. Schistosomiasis: clinical management of liver disease. Clin Liver Dis. (2015) 6:59–62. doi: 10.1002/cld.495
44. Enk MJ, Lima AC, Drummond SC, Schall VT, Coelho PM. The effect of the number of stool samples on the observed prevalence and the infection intensity with Schistosoma mansoni among a population in an area of low transmission. Acta Trop. (2008) 108:222–8. doi: 10.1016/j.actatropica.2008.09.016
45. Teles HM, de Carvalho ME, Santos Ferreira C, Zacharias F, de Lima VR, Fadel ML. Schistosomiasis mansoni in Bananal (State of São Paulo, Brazil): I. Efficiency of diagnostic and treatment procedures. Mem Inst Oswaldo Cruz. (2002) 97(Suppl 1):181–6. doi: 10.1590/S0074-02762002000900035
46. Candido RR, Favero V, Duke M, Karl S, Gutiérrez L, Woodward RC, et al. The affinity of magnetic microspheres for Schistosoma eggs. Int J Parasitol. (2015) 45:43–50. doi: 10.1016/j.ijpara.2014.08.011
47. Espírito-Santo MC, Alvarado-Mora MV, Dias-Neto E, Botelho-Lima LS, Moreira JP, Amorim M, et al. Evaluation of real-time PCR assay to detect Schistosoma mansoni infections in a low endemic setting. BMC Infect Dis. (2014) 14:558. doi: 10.1186/s12879-014-0558-4
48. Cnops L, Soentjens P, Clerinx J, Van Esbroeck M. A Schistosoma haematobium-specific real-time PCR for diagnosis of urogenital schistosomiasis in serum samples of international travelers and migrants. PLoS Negl Trop Dis. (2013) 7:e2413. doi: 10.1371/journal.pntd.0002413
49. Cunningham LJ, Stothard JR, Osei-Atweneboana M, Armoo S, Verweij JJ, Adams ER. Developing a real-time PCR assay based on multiplex high-resolution melt-curve analysis: a pilot study in detection and discrimination of soil-transmitted helminth and schistosome species. Parasitology. (2018) 2018:1–6. doi: 10.1017/S0031182018001361
50. Madinga J, Polman K, Kanobana K, van Lieshout L, Brienen E, Praet N, et al. Epidemiology of polyparasitism with Taenia solium, schistosomes and soil-transmitted helminths in the co-endemic village of Malanga, Democratic Republic of Congo. Acta Trop. (2017) 171:186–93. doi: 10.1016/j.actatropica.2017.03.019
51. Sady H, Al-Mekhlafi HM, Ngui R, Atroosh WM, Al-Delaimy AK, et al. Detection of Schistosoma mansoni and Schistosoma haematobium by real-time PCR with high resolution melting analysis. Int J Mol Sci. (2015) 16:16085–103. doi: 10.3390/ijms160716085
52. Wichmann D, Poppert S, Von Thien H, Clerinx J, Dieckmann S, Jensenius M, et al. Prospective European-wide multicentre study on a blood based real-time PCR for the diagnosis of acute schistosomiasis. BMC Infect Dis. (2013)13:55. doi: 10.1186/1471-2334-13-55
53. Mott KE, Dixon M. Collaborative study on antigens for immunodiagnosis of schistosomiasis. Bull World Health Organ. (1982) 60:729–53.
54. Tsang VCW, Peralta JM, Simons AR. Enzyme-linked immunoelectrotransfer blot techniques (EITB) for studying the specificities of antigens and antibodies separated by gel electrophoresis. Methods Enzymol. (1983) 92: 377–91. doi: 10.1016/0076-6879(83)92032-3
55. Deelder AM, Qian ZL, Kremsner PG, Acosta L, Rabello AL, Enyong P, et al. Quantitative diagnosis of Schistosoma infections by measurement of circulating antigens in serum and urine. Trop Geogr Med. (1994) 46(4 Spec No):233–8.
56. Polman K, Stelma FF, Gryseels B, Van Dam GJ, Talla I, Niang M, et al. Epidemiologic application of circulating antigen detection in a recent Schistosoma mansoni focus in Northern Senegal. Am J Trop Med Hyg. (1995) 53:152–7. doi: 10.4269/ajtmh.1995.53.152
57. Van Lieshout L, Panday UG, De Jonge N, Krijger FW, Oostburg BF, Polderman AM, et al. Immunodiagnosis of Schistosomiasis mansoni in a low endemic area in Surinam by determination of the circulating antigens CAA and CCA. Acta Trop. (1995) 59:19–29. doi: 10.1016/0001-706X(94)00084-E
58. Corstjens PL, van Lieshout L, Zuiderwijk M, Kornelis D, Tanke HJ, Deelder AM, et al. Up-converting phosphor technology-based lateral flow assay for detection of Schistosoma circulating anodic antigen in serum. J Clin Microbiol. (2008) 46:171–6. doi: 10.1128/JCM.00877-07
59. Corstjens PL, De Dood CJ, Kornelis D, Fat EM, Wilson RA, Kariuki TM, et al. Tools for diagnosis, monitoring and screening of Schistosoma infections utilizing lateral-flow based assays and upconverting phosphor labels. Parasitology. (2014) 141:1841–55. doi: 10.1017/S0031182014000626
60. van Dam GJ1, de Dood CJ, Lewis M, Deelder AM, van Lieshout L, Tanke HJ, et al. A robust dry reagent lateral flow assay for diagnosis of active schistosomiasis by detection of Schistosoma circulating anodic antigen. Exp Parasitol. (2013) 135:274–82. doi: 10.1016/j.exppara.2013.06.017
61. Knopp S, Corstjens PL, Koukounari A, Cercamondi CI, Ame SM, Ali SM, et al. Sensitivity and specificity of a urine circulating anodic antigen test for the diagnosis of Schistosoma haematobium in low endemic settings. PLoS Negl Trop Dis. (2015) 9:e0003752. doi: 10.1371/journal.pntd.0003752
62. van Grootveld R, van Dam GJ, de Dood C, de Vries JJC, Visser LG, Corstjens PLAM, et al. Improved diagnosis of active Schistosoma infection in travellers and migrants using the ultra-sensitive in-house lateral flow test for detection of circulating anodic antigen (CAA) in serum. Eur J Clin Microbiol Infect Dis. (2018) 37:1709–16. doi: 10.1007/s10096-018-3303-x
63. Danso-Appiah A, Minton J, Boamah D, Otchere J, Asmah RH, Rodgers M, et al. Accuracy of point-of-care testing for circulatory cathodic antigen in the detection of schistosome infection: systematic review and meta-analysis. Bull World Health Organ. (2016) 94:522–33. doi: 10.2471/BLT.15.158741
64. Coelho PM, Siqueira LM, Grenfell RF, Almeida NB, Katz N, Almeida A et al. Improvement of POC-CCA interpretation by using lyophilization of urine from patients with Schistosoma mansoni Low worm burden: towards an elimination of doubts about the concept of trace. PLoS Negl Trop Dis. (2016) 10:e0004778. doi: 10.1371/journal.pntd.0004778
65. Clements MN, Donnelly CA, Fenwick A, Kabatereine NB, Knowles SCL, Meité A, et al. Interpreting ambiguous ‘trace' results in Schistosoma mansoni CCA tests: estimating sensitivity and specificity of ambiguous results with no gold standard. PLoS Negl Trop Dis. (2017)11:e0006102. doi: 10.1371/journal.pntd.0006102
66. Beltrame A, Guerriero M, Angheben A, Gobbi F, Requena-Mendez A, Zammarchi L, et al. Accuracy of parasitological and immunological tests for the screening of human schistosomiasis in immigrants and refugees from African countries: an approach with latent class analysis. PLoS Negl Trop Dis. (2017) 11:e0005593.
67. Neumayr A, Chernet A, Sydow V, Kling K, Kuenzli E, Marti H, et al. Performance of the point-of-care circulating cathodic antigen (POC-CCA) urine cassette test for follow-up after treatmentof S. mansoni infection in Eritrean refugees. Travel Med Infect Dis. (2018) S1477-8939(18)30236-9. doi: 10.1016/j.tmaid.2018.09.004
Keywords: schistosomiasis, molecular diagnosis, POC-CCA, POC-CAA, praziquantel
Citation: Cavalcanti MG, Cunha AFA and Peralta JM (2019) The Advances in Molecular and New Point-of-Care (POC) Diagnosis of Schistosomiasis Pre- and Post-praziquantel Use: In the Pursuit of More Reliable Approaches for Low Endemic and Non-endemic Areas. Front. Immunol. 10:858. doi: 10.3389/fimmu.2019.00858
Received: 04 October 2018; Accepted: 03 April 2019;
Published: 28 May 2019.
Edited by:
Michael Harrison Hsieh, Children's National Health System, United StatesReviewed by:
William Evan Secor, Centers for Disease Control and Prevention (CDC), United StatesRicardo Fujiwara, Federal University of Minas Gerais, Brazil
Copyright © 2019 Cavalcanti, Cunha and Peralta. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: José Mauro Peralta, peralta@micro.ufrj.br