
Summary
Levofloxacin is a fluoroquinolone antibiotic and is the optical S-(−) isomer of the racemic drug substance ofloxacin. It has a broad spectrum of in vitro activity against Gram-positive and Gram-negative bacteria, as well as certain other pathogens such as Mycoplasma, Chlamydia, Legionella and Mycobacteria spp. Levofloxacin is significantly more active against bacterial pathogens than R- (+) - ofloxacin. Levofloxacin hemihydrate, the commercially formulated product, is 97.6% levofloxacin by weight.
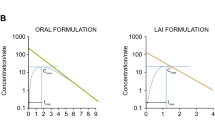
Levofloxacin pharmacokinetics are described by a linear 2-compartment open model with first-order elimination. Plasma concentrations in healthy volunteers reach a mean peak drug plasma concentration (Cmax) of approximately 2.8 and 5.2 mg/L within 1 to 2 hours after oral administration of levofloxacin 250 and 500mg tablets, respectively. The bioavailability of oral levofloxacin approaches 100% and is little affected by the administration with food. Oral absorption is very rapid and complete, with little difference in the serum concentration-time profiles following 500mg oral or intravenous (infused over 60 minutes) doses.
Single oral doses of levofloxacin 50 to 1000mg produce a mean Cmax and area under the concentration-time curve (AUC) ranging from approximately 0.6 to 9.4 mg/L and 4.7 to 108 mg·h/L, respectively, both increasing linearly in a doseproportional fashion. The pharmacokinetics of levofloxacin are similar during multiple-dose regimens to those following single doses. Levofloxacin is widely distributed throughout the body, with a mean volume of distribution of 1.1 L/kg, and penetrates well into most body tissues and fluids. Drug concentrations in tissues and fluids are generally greater than those observed in plasma, but penetration into the cerebrospinal fluid is relatively poor (concentrations approximately 16% of simultaneous plasma values). Levofloxacin is approximately 24 to 38% bound to serum plasma proteins (primarily albumin); serum protein binding is independent of serum drug concentrations.
The plasma elimination half-life (t½β) ranges from 6 to 8 hours in individuals with normal renal function. Approximately 80% of levofloxacin is eliminated as unchanged drug in the urine through glomerular filtration and tubular secretion; minimal metabolism occurs with the formation of no metabolites possessing relevant pharmacological activity. Renal clearance and total body clearance are highly correlated with creatinine clearance (CLcr), and dosage adjustments are required in patients with significant renal dysfunction. Levofloxacin pharmacokinetics are not appreciably affected by age, gender or race when differences in renal function, and body mass and composition are taken into account.
Important drug interactions exist with aluminium- and magnesium-containing antacids and ferrous sulfate, as with other fluoroquinolones, resulting in significantly decreased levofloxacin absorption when administered concurrently. These agents should be administered at least 2 hours before or after levofloxacin administration. Cimetidine and probenecid decrease levofloxacin renal clearance and increase t½β; the magnitudes of these interactions are not clinically significant. Levofloxacin appears to have only minor potential for significantly altering the pharmacokinetics of theophylline, warfarin, zidovudine, ranitidine, digoxin or cyclosporin; however, patients receiving these drugs concurrently should be monitored closely for signs of enhanced pharmacological effect or toxicity. Levofloxacin pharmacokinetics are not significantly altered by sucralfate when administration of these drugs is separated by at least 2 hours.
Article PDF
Similar content being viewed by others


References
Davis R, Bryson HM. Levofloxacin: a review of its antibacterial activity, pharmacokinetics and therapeutic efficacy. Drugs 1994; 47: 677–700
R.W. Johnson Pharmaceutical Research Institute, Raritan, New Jersey, USA. Data on file
Hayakawa I, Atarashi S, Yokohama S, et al. Synthesis and antimicrobial activities of optically active ofloxacin. Antimicrob Agents Chemother 1986; 29: 163–4
Hooper DC, Wolfson JS. The fluoroquinolones: pharmacology, clinical uses, and toxicities in humans. Antimicrob Agents Chemother 1985; 28: 716–21
Imamura M, Shibamura S, Hayakawa I, et al. Inhibition of DNA gyrase by optically active ofloxacin. Antimicrob Agents Chemother 1987; 31: 325–7
Tanaka K-I, Iwamoto M, Maesaki S, et al. Basic and clinical studies on levofloxacin in the treatment of respiratory infections. Jpn J Antibiot 1992; 45: 548–55
Shen LL, Pernet AG. Mechanism of inhibition of DNA gyrase by analogues of nalidixic acid: the target of the drugs is DNA. Proc Natl Acad Sci USA 1985; 82: 307–11
Smith JT. The mode of action of 4-quinolones and possible mechanisms of resistance. J Antimicrob Chemother 1986; 18 Suppl. D: 21–9
Fu KP, Grace ME, McCloud SJ, et al. Discrepancy between the antibacterial activities and the inhibitory effects of Micrococcus luteus DNA gyrase of 13 quinolones. Chemotherapy 1986; 29: 494–8
Lehr K-H, Damm P. Quantification of the enantiomers of ofloxacin in biological fluids by high-performance liquid chromatography. J Chromatogr 1988; 425: 153–61
Okazaki O, Kojima C, Hakusui H, et al. Enantioselective disposition of ofloxacin in humans. Antimicrob Agents Chemother 1991; 35: 2106–9
Nakashima M, Uematsu T, Kanamaru M, et al. Phase I study of levofloxacin, (S)-(−)-ofloxacin. Jpn J Clin Pharmacol Ther 1992; 23: 515–20
Wong FA, Juzwin SJ, Flor SC. Rapid stereospecific high-performance liquid chromatogrphic determination of levofloxacin in human plasma and urine. J Pharm Biomed Analysis 1997. In press
Child J, Mortiboy D, Andrews JM, et al. Open-label crossover study to determine the pharmacokinetics and penetration of two dose regimens of levofloxacin into inflammatory fluid. Antimicrob Agents Chemother 1995; 39: 2749–51
Lode H, Höffken G, Olschewski P, et al. Pharmacokinetics of ofloxacin after oral and parenteral administration. Antimicrob Agents Chemother 1987; 31: 1338–42
Sasaki J, Morishima T, Shiiki K, et al. Clinical study of levofloxacin in treatment of odontogenic infections. Chemotherapy 1992; 40 Suppl. 3: 379–91
Goodwin SD, Gallis HA, Chow AT, et al. Pharmacokinetics and safety of levofloxacin in patients with human immunodeficiency virus infection. Antimicrob Agents Chemother 1994; 38: 799–804
Holland ML, Chien S-C, Corrado ML, et al. The pharmacokinetic profile of levofloxacin following once-or twice-daily 500mg oral administration of levofloxacin hemihydrate [abstract]. 5th International Symposium on New Quinolones; 1994 Aug 25–27: Singapore
Chein SC, Chow AT, Fowler CL, et al. Double-blind evaluation of the safety and pharmacokinetics of multiple oral once-daily 750mg and 1g doses of levofloxacin in healthy volunteers [abstract A14]. American Society of Mircobiology: Abstracts of the 36th Interscience Conference on antimicrobial Agents and Chemotherapy; 1996 Sep 15–18; New Orleans, 3
Holland ML, Chien S-C, Corrado ML, et al. The pharmacokinetic profile of intravenous levofloxacin following once-or twice-daily 500mg administration [abstract]. 5th International Symposium on New Quinolones; 1994 Aug 25–27: Singapore
Dudley MN, Blaser J, Gilbert D, et al. Bactericidal activity of ciprofloxacin against Ps. aeruginosa and other bacteria in an in vitro capillary model. Rev Infect Dis1988; 10: S34–5
Ohi Y, Goto T, Kawahara K, et al. Penetration of fluoroquinolones into human spinal fluid. Chemotherapy 1992; 40: 469–73
Inoue S, Misaki M, Matsumura K. Intraocular penetration of DR-3355. Atarashii Ganka [J Eye] 1992; 9: 487–90
Tomii T, Fukuda M, Sasaki K. Penetration of l-ofloxacin (DR-3355) into the lacrimal fluid. Jpn J Clin Ophthalmol 1991; 45: 1607–10
Baba S, Miyamoto N, Yanai O, et al. Study on the penetration of levofloxacin (DR-3355) into the otorhinolaryngeal tissues and discharges in patients. Chemotherapy 1992; 40 Suppl. 3: 326–33
Nakamori Y, Tsuboi E, Narui K, et al. Sputum penetration of levofloxacin and its clinical efficacy in patients with chronic lower respiratory tract infections. Jpn J Antibiot 1992; 45: 539–47
Nagai H, Yamasaki T, Masuda M, et al. Penetration of levofloxacin into bronchoalveolar lavage fluid. Drugs 1993; 45 Suppl. 3: 259
Hukagawa H, Noga K. A study on the concentration of levofloxacin in the gallbladder tissue and bile of patients. Jpn J Antibiot 1992; 45: 253–7
Ohnishi H, Tanimura H, Ichimaya G, et al. Excretion of levofloxacin into bile and gallbladder tissue. Drugs 1993; 45 Suppl. 3: 260–1
Tanimura H, Ohnishi H, Okamura T, et al. Chemotherapy of biliary tract infections (XXXVII): excretion into bile and gallbladder tissue levels of levofloxacin and its clinical effect in biliary tract infections. Jpn J Antibiot 1992; 45: 557–68
Takahashi H, Mogi S, Kobayashi M, et al. Assay of skin level and clinical investigation of levofloxacin in the treatment of skin infections. Chemotherapy 1992; 40 Suppl. 3: 286–305
Saito I, Suzuki A, Saiko Y, et al. Acute nongonococcal epididymitis: aetiology and levofloxacin therapy. Drugs 1993; 45 Suppl. 3: 379
Saito I, Suzuki A, Saiko Y, et al. Acute nongonococcal epididymitis: pharmacological and therapeutic aspects of levofloxacin. Acta Urol Jpn 1992; 38: 623–8
Yamashita M, Sawada K, Chokyu H, et al. Prostatic tissue levels of levofloxacin. Chemotherapy 1992; 40 Suppl. 3: 203–9
Soyama Y, Mizuhara H, Iwata Y. Fundamental study on levofloxacin in the field of obstetrics and gynecology. Jpn J Antibiot 1992; 45: 265–9
Ito K, Mikamo H, Izumi K, et al. Penetration of levofloxacin into gynecological tissues. Chemotherapy 1992; 40 Suppl. 3: 306–10
Inagaki Y, Nakaya R, Chida T, et al. The effect of levofloxacin, an optically-active isomer of ofloxacin, on fecal microflora in human volunteers. Jpn J Antibiot 1992; 45: 241–52
Murata M, Ohnishi K, Irimajiri S, et al. Clinical trial of levofloxacin (DR-3355) and fecal drug concentration and change in the fecal microflora in infectious enteritis. Chemotherapy (Tokyo) 1992; 40 Suppl. 3: 170–87
Giamarellou H, Kolokythas E, Petrikkos G, et al. Pharmacokinetics of three newer quinolones in pregnant and lactating women. Am J Med 1989; 87 Suppl. 5A: 49–51
Nozaki-Renard J, Lino T, Sato Y, et al. Fluoroquinolones protect the human lymphocyte CEM cell line from HIV-1 mediated cytotoxicity. Cell Struct Funct 1990; 15: 295–9
Pascual A, Garcia I, Perea EJ. Uptake and intracellular activity of an optically active ofloxacin isomer in human neutrophils and tissue culture cells. Antimicrob Agents Chemother 1990; 34: 277–80
Pascual A, Garcia I, Conejo MC, et al. Fluorometric and high-performance liquid chromatographic measurement of quinolone uptake by human neutrophils. Eur J Clin Microbiol Infect Dis 1991; 10: 969–71
Gaja M, Higa F, Yamashiro T, et al. Penetration of levofloxacin, a new quinolone antibacterial agent, into human neutrophils. Chemotherapy 1992; 40 Suppl. 3: 64–7
Taira K, Koga H, Kohno S. Accumulation of a newly developed fluoroquinolone, OPC-17116, by human polymorphonuclear leukocytes. Antimicrob Agents Chemother 1993; 37: 1877–81
Perea EJ, Garcia I, Pascual A. Comparative penetration of lomefloxacin and other quinolones into human phagocytes. Am J Med 1992; 92 Suppl. 4A: 48S–51S
Gladue RP, Bright GM, Isaacson RE, et al. In vitro and in vivo uptake of azithromycin (CP-62,993) by phagocytic cells: possible mechanism of delivery and release at sites of infection. Antimicrob Agents Chemother 1989; 33: 277–82
Carbon C. Clinical relevance of intracellular and extracellular concentrations of macrolides. Infection 1995; 23 Suppl. 1: S10–4
Borner K, Lode H. Biotransformation of certain gyrase inhibitors. Infection 1986; 14 Suppl. 1: S54–9
Monk JP, Campoli-Richards DM. Ofloxacin: a review. Drugs 1987; 33: 346–91
Gaitonde MD, Mendes P, House ESA, et al. The effects of cimetidine and probenecid on the pharmacokinetics of levofloxacin [abstract no. A41]. American Society for Microbiology: Abstracts of the 35th Interscience Conference on Antimicrobial Agents and Chemotherapy; 1995 Sep 17–29: San Francisco, 8
Gisclon LG, Curtin CR, Williams RR, et al. The pharmacokinetics of levofloxacin in subjects with renal impairment, and in subjects receiving hemodialysis or continuous ambulatory peritoneal dialysis [abstract no. A13]. American Society for Microbiology: Abstracts of the 36th Interscience Conference on Antimicrobial Agents and Chemotherapy; 1996 Sep 15–18; New Orleans, 3
Chien SC, Chow AT, Williams R, et al. Absence of an effect of levofloxacin on digoxin pharmacokinetics [abstract]. American Academy of Pharmaceutical Scientists: Annual Meeting Program Supplement; 1995 Jun 5–6: New Brunswick
Lee L-J, Hafkin B, Lee I-D, et al. Effect of food and sucralfate on levofloxacin after a single oral dose of 500 mg in male and female subjects [abstract no. A40]. American Society for Microbiology: Abstracts of the 35th Interscience Conference on Antimicrobial Agents and Chemotherapy; 1995 Sep 17–29: San Francisco, 8
Rogge MC, Chien S-C, Wong F, et al. Single-dose pharmacokinetics of levofloxacin: influence of age and gender [abstract]. 5th International Symposium on New Quinolones; 1994 Aug 25–27: Singapore
Doose DR, Walker SA, Chien SC, et al. Absence of an effect of levofloxacin on cyclosporine pharmacokinetics in healthy adult volunteers [abstract]. American Academy of Pharmaceutical Scientists: Annual Meeting Program Supplement; 1995 Jun 5–6: New Brunswick
Saito A, Oguchi K, Harada Y, et al. Pharmacokinetics of levofloxacin in patients with impaired renal function. Chemotherapy 1992; 40 Suppl. 3: 188–95
Aoki N, Usuda Y, Koda Y, et al. Clinical pharmacology and efficacy of levofloxacin in elderly patients. Jpn J Antibiot 1992; 45: 530–8
Chien SC, Chow AT, Hendrix C, et al. The pharmacokinetics and safety of oral levofloxacin in HIV-infected individuals receiving concomitant zidovudine [abstract no. A33]. American Society for Microbiology: Abstracts of the 35th Interscience Conference on Antimicrobial Agents and Chemotherapy; 1995 Sep 17–29: San Francisco, 7
Radandt JM, Marchbanks CR, Dudley MN. Interactions of fluoroquinolones with other drugs: mechanisms, variability, clinical significance, and management. Clin Infect Dis 1992; 14: 272–84
Spooner KM, Baird BF, Davey RT, et al. Evaluation of the pharmacokinetics and safety of single and multiple high dose regimens of levofloxacin in HIV seropositive subjects [abstract no. LM32]. American Society for Microbiology: Abstracts of the 35th Interscience Conference on Antimicrobial Agents and Chemotherapy; 1995 Sep 17–29; San Francisco, 332
Niki Y, Hashiguchi K, Okimoto N, et al. Quinolone antimicrobial agents and theophylline [letter]. Chest 1992; 101: 881
Preston SL, Drusano GL, Berman AL, et al. Levofloxacin population pharmacokinetics and creation of a demographics model for prediction of individual drug clearance in patients with serious community-aquired infection [abstract A12]. American Society for Microbiology: Abstracts of the 36th Interscience Conference on Antimicrobial Agents and Chemotherapy; 1996 Sep 15–18; New Orleans, 2
Okimoto N, Niki Y, Soejima R. Effect of levofloxacin on serum concentration of theophylline. Chemotherapy 1992; 40 Suppl. 3: 68–74
Beckmann J, Elsässer W, Gundert-Remy U, et al. Enoxacin: a potent inhibitor of theophylline metabolism. Eur J Clin Pharmacol 1987; 33: 227–30
Gisclon LG, Curtin CR, Fowler CL, et al. Absence of a pharmacokinetic interaction between intravenous theophylline and orally administered levofloxacin [abstract no. A39]. American Society for Microbiology: Abstracts of the 35th Interscience Conference on Antimicrobial Agents and Chemotherapy; 1995 Sep 17–29: San Francisco, 8
Tanaka M, Kurata T, Fujisawa C, et al. Mechanistic study of inhibition of levofloxacin absorption by aluminum hydroxide. Antimicrob Agents Chemother 1993; 37: 2173–8
Nix DE, Wilton JH, Schentag JJ, et al. Inhibition of norfloxacin absorption by antacids and sucralfate. Rev Infect Dis 1989; 11 Suppl. 5: S1096–8
Shiba K, Sakai O, Shimada J, et al. Effect of antacids, ferrous sulfate, and ranitidine on absorption of DR-3355 in humans. Antimicrob Agents Chemother 1992; 36: 2270–4
Polk RE, Healy DP, Sahai J, et al. Effect of ferrous sulfate and multivitamins with zinc on absorption of ciprofloxacin in normal volunteers. Antimicrob Agents Chemother 1989; 33: 1841–4
Höffken G, Lode H, Wiley R, et al. Pharmacokinetics and bioavailability of ciprofloxacin and ofloxacin: effect of food and antacid intake. Rev Infect Dis 1988; 10 Suppl. 1: S138–9
Liao S, Palmer M, Fowler CL, et al. Absence of the effect of levofloxacin on warfarin pharmacokinetics and anticoagulation in male volunteers [abstract no. A42]. American Society for Microbiology: Abstracts of the 35th Interscience Conference on Antimicrobial Agents and Chemotherapy; 1995 Sep 17–29: San Francisco, 8
Holland ML, Chow AT, Chien S-C, et al. The pharmacokinetics of oral levofloxacin in HIV-infected individuals with or without concomitant zidovudine [abstract]. 5th International Symposium on New Quinolones; 1994 Aug 25–27: Singapore
Chalkley LJ, Koornhof HJ. Antimicrobial activity of ciprofloxacin against Pseudomonas aeruginosa, Escherichia coli, and Staphylococcus aureus determined by the killing curve method: antibiotic comparisons and synergistic interactions. Antimicrob Agents Chemother 1985; 28: 331–42
Peloquin CA, Cumbo TJ, Nix DE, et al. Intravenous ciprofloxacin in patients with nosocomial lower respiratory tract infections: impact of plasma concentrations, organism MIC, and clinical condition on bacterial eradication. Arch Intern Med 1989; 149: 2269–73
Maderas-Kelly KJ, Ostergaard BE, Hovde LB, et al. Twenty-four-hour area under the concentration-time curve/MIC ratio as a generic predictor or fluoroquinolone antimicrobial effect by using three strains of Pseudomonas aeruginosa and an in vitro pharmacodynamic model. Antimicrob Agents Chemother 1996; 40: 627–32
Palmer SM, Rybak MJ. Pharmacodynamics of once-or twice-daily levofloxacin versus vancomycin, with or without rifampin, against Staphylococcus aureus in an in vitro model with infected platelet-fibrin clots. Antimicrob Agents Chemother 1996; 40: 701–5
Forrest A, Nix DE, Ballow CH, et al. Pharmacodynamics of intravenous ciprofloxacin in severely ill patients. Antimicrob Agents Chemother 1993; 37: 1073–81
Preston SL, Drusano GL, Berman AL, et al. Prospective development of pharmacodynamic relationships between measures of levofloxacin exposure and measures of patient outcome [abstract no. A98]. American Society for Microbiology: Abstracts of the 36th Interscience Conference on Antimicrobial Agents and Chemotherapy; 1996 Sep 15–18: New Orleans, 19
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Fish, D.N., Chow, A.T. The Clinical Pharmacokinetics of Levofloxacin. Clin-Pharmacokinet 32, 101–119 (1997). https://doi.org/10.2165/00003088-199732020-00002
Published:
Issue Date:
DOI: https://doi.org/10.2165/00003088-199732020-00002