
Abstract
Objective
To retrospectively investigate whether optimisation of volume-doubling time (VDT) cutoff for fast-growing nodules in lung cancer screening can reduce false-positive referrals.
Methods
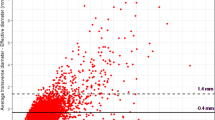
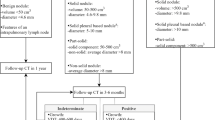
Screening participants of the NELSON study underwent low-dose CT. For indeterminate nodules (volume 50–500 mm3), follow-up CT was performed 3 months after baseline. A negative baseline screen resulted in a regular second-round examination 1 year later. Subjects referred to a pulmonologist because of a fast-growing (VDT <400 days) solid nodule in the baseline or regular second round were included in this study. Histology was the reference for diagnosis, or stability on subsequent CTs, confirming benignity. Mean follow-up of non-resected nodules was 4.4 years. Optimisation of the false-positive rate was evaluated at maintained sensitivity for lung cancer diagnosis with VDT <400 days as reference.
Results
Sixty-eight fast-growing nodules were included; 40 % were malignant. The optimal VDT cutoff for the 3-month follow-up CT after baseline was 232 days. This cutoff reduced false-positive referrals by 33 % (20 versus 30). For the regular second round, VDTs varied more among malignant nodules, precluding lowering of the VDT cutoff of 400 days.
Conclusion
All malignant fast-growing lung nodules referred after the 3-month follow-up CT in the baseline lung cancer screening round had VDT ≤232 days. Lowering the VDT cutoff may reduce false-positive referrals.
Key Points
• Lung nodules are common in CT lung cancer screening, most being benign
• Short-term follow-up CT can identify fast-growing intermediate-size lung nodules
• Most fast-growing nodules on short-term follow-up CT still prove to be benign
• A new volume-doubling time (VDT) cut-off is proposed for lung screening
• The optimised VDT cutoff may decrease false-positive case referrals for lung cancer





Similar content being viewed by others

Abbreviations
- 2D:
-
Two-dimensional
- 3D:
-
Three-dimensional
- CT:
-
Computed tomography
- NELSON:
-
Dutch–Belgian randomised lung cancer screening trial
- NLST:
-
National Lung Screening Trial
- PPV:
-
Positive predictive value
- VDT:
-
Volume-doubling time
References
National Lung Screening Trial Research Team, Aberle DR, Adams AM et al (2011) Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med 365:395–409
Infante M, Lutman FR, Cavuto S et al (2008) Lung cancer screening with spiral CT: baseline results of the randomized DANTE trial. Lung Cancer 59:355–363
Lopes Pegna A, Picozzi G, Mascalchi M et al (2009) Design, recruitment and baseline results of the ITALUNG trial for lung cancer screening with low-dose CT. Lung Cancer 64:34–40
Blanchon T, Brechot JM, Grenier PA et al (2007) Baseline results of the Depiscan study: a French randomized pilot trial of lung cancer screening comparing low dose CT scan (LDCT) and chest X-ray (CXR). Lung Cancer 58:50–58
Gohagan JK, Marcus PM, Fagerstrom RM et al (2005) Final results of the lung screening study, a randomized feasibility study of spiral CT versus chest X-ray screening for lung cancer. Lung Cancer 47:9–15
van Klaveren RJ, Oudkerk M, Prokop M et al (2009) Management of lung nodules detected by volume CT scanning. N Engl J Med 361:2221–2229
Henschke CI, Yankelevitz DF, Naidich DP et al (2004) CT screening for lung cancer: suspiciousness of nodules according to size on baseline scans. Radiology 231:164–168
Swensen SJ, Jett JR, Sloan JA et al (2002) Screening for lung cancer with low-dose spiral computed tomography. Am J Respir Crit Care Med 165:508–513
Yankelevitz DF, Reeves AP, Kostis WJ, Zhao B, Henschke CI (2000) Small pulmonary nodules: volumetrically determined growth rates based on CT evaluation. Radiology 217:251–256
Xu DM, Gietema H, de Koning H et al (2006) Nodule management protocol of the NELSON randomised lung cancer screening trial. Lung Cancer 54:177–184
van Iersel CA, de Koning HJ, Draisma G et al (2007) Risk-based selection from the general population in a screening trial: selection criteria, recruitment and power for the Dutch–Belgian randomised lung cancer multi-slice CT screening trial (NELSON). Int J Cancer 120:868–874
Gietema HA, Schaefer-Prokop CM, Mali WP, Groenewegen G, Prokop M (2007) Pulmonary nodules: interscan variability of semiautomated volume measurements with multisection CT-influence of inspiration level, nodule size, and segmentation performance. Radiology 245:888–894
CBO (2004) Guideline-non-small cell lung cancer: staging and treatment. Van Zuiden Communications BV, Alphen aan de Rijn
Xu DM, van der Zaag-Loonen HJ, Oudkerk M et al (2009) Smooth or attached solid indeterminate nodules detected at baseline CT screening in the NELSON study: cancer risk during 1 year of follow-up. Radiology 250:264–272
MacMahon H, Austin JH, Gamsu G et al (2005) Guidelines for management of small pulmonary nodules detected on CT scans: a statement from the Fleischner Society. Radiology 237:395–400
Xu DM, van Klaveren RJ, de Bock GH et al (2008) Limited value of shape, margin and CT density in the discrimination between benign and malignant screen detected solid pulmonary nodules of the NELSON trial. Eur J Radiol 68:347–352
Nietert PJ, Ravenel JG, Leue WM et al (2009) Imprecision in automated volume measurements of pulmonary nodules and its effect on the level of uncertainty in volume doubling time estimation. Chest 135:1580–1587
Ko JP, Berman EJ, Kaur M et al (2012) Pulmonary nodules: growth rate assessment in patients by using serial CT and three-dimensional volumetry. Radiology 262:662–671
Pedersen JH, Ashraf H, Dirksen A et al (2009) The Danish randomized lung cancer CT screening trial—overall design and results of the prevalence round. J Thorac Oncol 4:608–614
Brewer NT, Salz T, Lillie SE (2007) Systematic review: the long-term effects of false-positive mammograms. Ann Intern Med 146:502–510
van den Bergh KA, Essink-Bot ML, Bunge EM et al (2008) Impact of computed tomography screening for lung cancer on participants in a randomized controlled trial (NELSON trial). Cancer 113:396–404
Wilson DO, Ryan A, Fuhrman C et al (2012) Doubling times and CT screen-detected lung cancers in the Pittsburgh lung screening study. Am J Respir Crit Care Med 185:85–89
Yankelevitz DF, Kostis WJ, Henschke CI et al (2003) Overdiagnosis in chest radiographic screening for lung carcinoma: frequency. Cancer 97:1271–1275
Revel MP, Merlin A, Peyrard S et al (2006) Software volumetric evaluation of doubling times for differentiating benign versus malignant pulmonary nodules. AJR Am J Roentgenol 187:135–142
Winer-Muram HT, Jennings SG, Tarver RD et al (2002) Volumetric growth rate of stage I lung cancer prior to treatment: serial CT scanning. Radiology 223:798–805
Revel MP, Bissery A, Bienvenu M, Aycard L, Lefort C, Frija G (2004) Are two-dimensional CT measurements of small noncalcified pulmonary nodules reliable? Radiology 231:453–458
Mikita K, Saito H, Sakuma Y et al (2012) Growth rate of lung cancer recognized as small solid nodule on initial CT findings. Eur J Radiol 81:e548–e553
Acknowledgments
The NELSON trial was sponsored by: The Netherlands Organisation for Health Research and Development (ZonMw); Dutch Cancer Society Koningin Wilhelmina Fonds (KWF); Stichting Centraal Fonds Reserves van Voormalig Vrijwillige Ziekenfondsverzekeringen (RvvZ); Siemens Germany; Rotterdam Oncologic Thoracic Steering committee (ROTS); G. Ph. Verhagen Trust, Flemish League Against Cancer, Foundation Against Cancer and Erasmus Trust Fund.
The funders played no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Additional information
The institutions where the work was performed:
University of Groningen/University Medical Center Groningen, Groningen, The Netherlands; University Medical Center Utrecht, Utrecht, The Netherlands; Kennemer Gasthuis, Haarlem, The Netherlands; University Hospital Gasthuisberg Leuven, Leuven, Belgium
Rights and permissions
About this article
Cite this article
Heuvelmans, M.A., Oudkerk, M., de Bock, G.H. et al. Optimisation of volume-doubling time cutoff for fast-growing lung nodules in CT lung cancer screening reduces false-positive referrals. Eur Radiol 23, 1836–1845 (2013). https://doi.org/10.1007/s00330-013-2799-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-013-2799-9