
Abstract
Objective
To evaluate the usefulness of B-type natriuretic peptide and troponin I measurements in predicting right ventricular dysfunction (RVD) in non-massive pulmonary embolism.
Design
Prospective observational study.
Setting
University-affiliated emergency unit, cardiology and pneumology departments.
Patients
Sixty-seven patients admitted because of acute pulmonary embolism, without shock on admission, completed the study.
Interventions
Blood samples and echocardiography were obtained on admission for subsequent and independent assessment of B-type natriuretic peptide (BNP) and troponin I levels as well as RVD.
Measurements and results
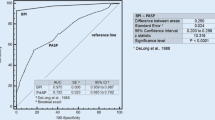
Echocardiographic RVD was diagnosed in 36 patients and was severe in 13 on admission. BNP and troponin I levels were higher in patients with RVD than in those with no RVD [62 (27–105) vs. 431 (289–556) pg/ml for BNP, p < 0.001; 0.01 (0–0.09) vs. 0.16 (0.03–0.32) μg/l for troponin I, p = 0.005]. The area under the receiving operating characteristic curve (AUC) for diagnosing RVD was 0.93 for BNP and 0.72 for troponin I. The troponin I level increased further when RVD was severe, compared with moderate, and the AUC was 0.91 for identifying severe RVD. Diagnoses of RVD and severe RVD were ruled out by BNP ≤ 100 pg/ml (30% of patients) and troponin I 0.10 μg/l (58% of patients), respectively. In-hospital death or circulatory failure occurred in nine patients; all had echographic RVD and level of BNP > 100 pg/ml and troponin I > 0.10 μg/l.
Conclusion
In hemodynamically stable pulmonary embolism, BNP/troponin I measurement is helpful on admission, especially for ruling out RVD, i. e. patients with in-hospital high-risk.


Similar content being viewed by others


Abbreviations
- RVD:
-
right ventricular dysfunction
- BNP:
-
B-type natriuretic peptide
- ECG:
-
electrocardiographic
- AUC:
-
area under the receiving operating characteristic curve
References
Grifoni S, Olivotto I, Cecchini P, Pieralli F, Camaiti A, Santoro G, Conti A, Agnelli G, Berni G (2000) Short-term clinical outcome of patients with acute pulmonary embolism, normal blood pressure, and echocardiographic right ventricular dysfunction. Circulation 101:2817–2822
Goldhaber SZ, Visani L, De Rosa M (1999) Acute pulmonary embolism: clinical outcomes in the International Cooperative Pulmonary Embolism Registry (ICOPER). Lancet 353:1386–1389
Kasper W, Konstantinides S, Geibel A, Tiede N, Krause K, Just H (1997) Prognostic significance of right ventricular afterload stress detected by echocardiography in patients with clinically suspected pulmonary embolism. Heart 77:346–349
Goldhaber SZ, Elliott CG (2003) Acute pulmonary embolism: part I: epidemiology, pathophysiology, and diagnosis. Circulation 108:2726–2729
Konstantinides S, Geibel A, Heusel G, Heinrich F, Kasper W (2002) Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolism. N Engl J Med 347:1143–1150
Goldhaber SZ (2002) Echocardiography in the management of pulmonary embolism. Ann Intern Med 136:691–700
Vieillard-Baron A, Prin S, Chergui K, Dubourg O, Jardin F (2002) Echo-Doppler demonstration of acute cor pulmonale at the bedside in the medical intensive care unit. Am J Respir Crit Care Med 166:1310–1319
Jardin F, Dubourg O, Bourdarias JP (1997) Echocardiographic pattern of acute cor pulmonale. Chest 111:209–217
Jaffe AS, Babuin L, Apple FS (2006) Biomarkers in acute cardiac disease: the present and the future. J Am Coll Cardiol 48:1–11
Jason P, Keang LT, Hoe LK (2005) B-type natriuretic peptide: issues for the intensivist and pulmonologist. Crit Care Med 9:2094–2103
The PIOPED Investigators (1990) Value of the ventilation/perfusion scan in acute pulmonary embolism. Results of the prospective investigation of pulmonary embolism diagnosis (PIOPED). JAMA 263:2753–2759
Schoepf UJ, Goldhaber SZ, Costello P (2004) Spiral computed tomography for acute pulmonary embolism. Circulation 109:2160–2167
Miller GA, Sutton GC, Kerr IH, Gibson RV, Honey M (1971) Comparison of streptokinase and heparin in treatment of isolated acute massive pulmonary embolism. Br Heart J 33:616
Ribeiro A, Juhlin-Dannfelt A, Brodin LA, Holmgren A, Jorfeldt L (1998) Pulmonary embolism: relation between the degree of right ventricle overload and the extent of perfusion defects. Am Heart J 135:868–874
Mansencal N, Joseph T, Vieillard-Baron A, Langlois S, El Hajjam M, Qanadli SD, Lacombe P, Jardin F, Dubourg O (2005) Diagnosis of right ventricular dysfunction in acute pulmonary embolism using helical computed tomography. Am J Cardiol 95:1260–1263
Kostrubiec M, Pruszczyk P, Bochowicz A, Pacho R, Szulc M, Kaczynska A, Styczynski G, Kuch-Wocial A, Abramczyk P, Bartoszewicz Z, Berent H, Kuczynska K (2005) Biomarker-based risk assessment model in acute pulmonary embolism. Eur Heart J 26:2166–2172
Phua J, Lim TK, Lee KH (2005) B-type natriuretic peptide: issues for the intensivist and pulmonologist. Crit Care Med 33:2094–2013
Vieillard-Baron A, Page B, Augarde R, Prin S, Qanadli S, Beauchet A, Dubourg O, Jardin F (2001) Acute cor pulmonale in massive pulmonary embolism: incidence, echocardiographic pattern, clinical implications and recovery rate. Intensive Care Med 27:1481–1486
Nagaya N, Nishikimi T, Okano Y, Uematsu M, Satoh T, Kyotani S, Kuribayashi S, Hamada S, Kakishita M, Nakanishi N, Takamiya M, Kunieda T, Matsuo H, Kangawa K (1998) Plasma brain natriuretic peptide levels increase in proportion to the extent of right ventricular dysfunction in pulmonary hypertension. J Am Coll Cardiol 31:202–208
Kruger S, Graf J, Merx MW, Koch KC, Kunz D, Hanrath P, Janssens U (2004) Brain natriuretic peptide predicts right heart failure in patients with acute pulmonary embolism. Am Heart J 147:60–65
Pruszczyk P, Kostrubiec M, Bochowicz A, Styczynski G, Szulc M, Kurzyna M, Fijalkowska A, Kuch-Wocial A, Chlewicka I, Torbicki A (2003) N-terminal pro-brain natriuretic peptide in patients with acute pulmonary embolism. Eur Respir J 22:649–653
Tulevski II, Hirsch A, Sanson BJ, Romkes H, van der Wall EE, van Veldhuisen DJ, Buller HR, Mulder BJ (2001) Increased brain natriuretic peptide as a marker for right ventricular dysfunction in acute pulmonary embolism. Thromb Haemost 86:1193–1196
Missov E, Calzolari C, Pau B (1997) Circulating cardiac troponin I in severe congestive heart failure. Circulation 96:2953–2958
Logeart D, Beyne P, Cusson C, Tokmakova M, Leban M, Guiti C, Bourgoin P, Cohen Solal A (2001) Evidence of cardiac myolysis in severe nonischemic heart failure and the potential role of increased wall strain. Am Heart J 141:247–253
Kucher N, Printzen G, Goldhaber SZ (2003) Prognostic role of brain natriuretic peptide in acute pulmonary embolism. Circulation 107:2545–2547
ten Wolde M, Tulevski II, Mulder JW, Sohne M, Boomsma F, Mulder BJ, Buller HR (2003) Brain natriuretic peptide as a predictor of adverse outcome in patients with pulmonary embolism. Circulation 107:2082–2084
Pieralli F, Olivotto I, Vanni S, Conti A, Camaiti A, Targioni G, Grifoni S, Berni G (2006) Usefulness of bedside testing for brain natriuretic peptide to identify right ventricular dysfunction and outcome in normotensive patients with acute pulmonary embolism. Am J Cardiol 97:1386–1390
Kucher N, Printzen G, Doernhoefer T, Windecker S, Meier B, Hess PM (2003) Low pro-brain natriuretic peptide levels predict benign clinical outcome in acute pulmonary embolism. Circulation 107:1576–1578
Binder L, Pieske B, Olschewski M, Geibel A, Klostermann B, Reiner C, Konstantinides S (2005) N-terminal pro-brain natriuretic peptide or troponin testing followed by echocardiography for risk stratification of acute pulmonary embolism. Circulation 112:1573–1579
Logeart D, Saudubray C, Beyne P, Thabut G, Ennezat PV, Chavelas C, Zanker C, Bouvier E, Cohen, Solal A (2002) Comparative value of Doppler echocardiography and B-type natriuretic peptide assay in the etiologic diagnosis of acute dyspnea. J Am Coll Cardiol 40:1794–1800
Goldhaber SZ (2001) Thrombolysis in pulmonary embolism: a large-scale clinical trial is overdue. Circulation 104:2876–2878
Goldhaber SZ (2005) Thrombolytic therapy for patients with pulmonary embolism who are hemodynamically stable but have right ventricular dysfunction: pro. Arch Intern Med 165:2197–2199; discussion 2204–2205
Thabut G, Logeart D (2005) Thrombolysis for pulmonary embolism in patients with right ventricular dysfunction: con. Arch Intern Med 165:2200–2203; discussion 2204–2205
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Logeart, D., Lecuyer, L., Thabut, G. et al. Biomarker-based strategy for screening right ventricular dysfunction in patients with non-massive pulmonary embolism. Intensive Care Med 33, 286–292 (2007). https://doi.org/10.1007/s00134-006-0482-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-006-0482-1