
Abstract
Objective
To evaluate the bacteriology of early aspiration pneumonia using a protected specimen brush and quantitative culture techniques, and whether penicillin G is adequate as initial treatment pending culture results.
Patients and methods
52 patients (of which 45 required mechanical ventilation) meeting usual clinical criteria for aspiration pneumonia were prospectively included. On admission, patients were given intravenous penicillin G and a protected specimen brush was performed ≤48 h after.
Results
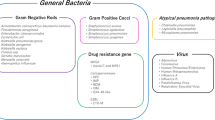
Cultures of the brush were negative (<103 CFU/ml) in 33 patients (1 had blood cultures positive withS. pneumoniae) and positive (≥103 CFU/ml) forS. pneumoniae in 2 patients. Seventeen patients had a positive culture (≥103 CFU/ml) for at least one penicillin G resistant microorganism, with a total of 20 organisms (S. aureus: 6;H. influenzae: 2;Enterobacteriaceae: 8;P. aeruginosa: 3;C. albicans: 1). In 4 of these patients, a penicillin-sensitive pathogen was also recovered in significant concentrations (S. pneumoniae: 2;Streptococcus sp.: 2). These 17 patients with a resistant pathogen did not differ from the 35 other patients with respect to need for ventilatory support and mortality rate. By contrast, they were older (61.1±21.9 vs 42.9±18.8 years;p<0.005) and required longer mechanical ventilation (6.1±4.6 vs. 3.5±2.7 days;p<0.03) and hospitalization (11.2±8.8 vs. 6.7±4.7 days;p<0.02). Of 17 patients 12 with penicillin G resistant organisms versus 0/35 without, were in-hospital patients and/or had a digestive disorder (p<0.001).
Conclusion
The broad range of offending organisms seen in early aspiration pneumonia precludes use of any single empiric regimen, making protected specimen brush mandatory in many patients. Nevertheless, the involvement ofS. pneumoniae in a notable proportion of our patients suggests that routine penicillin prophylaxis after early aspiration (at least in most patients with community-acquired aspiration) is warranted given the potential severity of pneumococcal sepsis in such patients.
Article PDF
Similar content being viewed by others


References
Cameron JL, Mitchell WH, Zuidema GD (1973) Aspiration pneumonia. Clinical outcome following documented aspiration. Arch Surg 106:49–52
Stewardson RH, Nyhus LM (1977) Pulmonary aspiration. Arch Surg 112:1192–1197
Cameron JL, Zuidema GD (1972) Aspiration pneumonia. Magnitude and frequency of the problem. JAMA 219:1194–1196
Bynum LJ, Pierce AK (1976) Pulmonary aspiration of gastric contents. Am Rev Respir Dis 114:1129–1136
Lorber B, Swenson RM (1974) Bacteriology of aspiration pneumonia. A prospective study of community-and hospital-acquired cases. Ann Intern Med 81:329–331
Hickling KG, Howard R (1988) A retrospective survey of treatment and mortality in aspiration pneumonia. Intensive Care Med 14:617–622
DePaso WJ (1991) Aspiration pneumonia. Clin Chest Med 12:269–284
Arms RA, Dines DE, Tinstman TC (1974) Aspiration pneumonia. Chest 65:136–139
Bartlett JG, Gorbach SL, Finegold SM (1974) The bacteriology of aspiration pneumonia. Am J Med 56:202–207
Bartlett JG, Gorbach SL (1975) The triple threat of aspiration pneumonia. Chest 68:560–566
LoCicero J 3d. (1989) Bronchopulmonary aspiration. Surg Clin North Am 69:71–79
Bartlett JG, Gorbach SL (1975) Treatment of aspiration pneumonia and primary lung abscess. Penicillin G vs clindamycin. JAMA 234:935–937
Murray HW (1979) Antimicrobial therapy in pulmonary aspiration. Am J Med 66:188–190
Ducroix JP, Tondriaux A, Smail A, Lobjoie E, Laurens G, Baillet J (1990) Traitement des pneumopathies d'inhalation par la piperacilline. Pathol Biol 38:530–532
Spencer CD, Beaty HN (1972) Complications of transtracheal aspiration. N Engl J Med 286:304–306
Unger KM, Moser KM (1973) Fatal complication of transtracheal aspiration. A report of two cases. Arch Intern Med 132:437–439
Pitts JC III, Brantigan CO, Hopeman AR (1977) Myocardial ischemia associated with transtracheal aspiration. JAMA 237: 2527–2528
Tobin MJ, Grenvick A (1984) Nosocomial lung infection and its diagnosis. Crit Care Med 12:191–199
Wimberley N, Faling LJ, Bartlett JG (1979) A fiberoptic bronchoscopy technique to obtain uncontaminated lower airway secretions for bacterial culture Am Rev Respir Dis 119:337–343
Chastre J, Viau F, Brun P, Pierre J, Dauge MC, Bouchama A, Akesbi A, Gibert C (1984) Prospective evaluation of the protected specimen brush for the diagnosis of pulmonary infections in ventilated patients. Am Rev Respir Dis 130:924–929
Fagon JY, Chastre J, Hance AJ, Guiguet M, Trouillet JL, Domart Y, Pierre J, Gibert C (1988) Detection of nosocomial lung infection in ventilated patients. Use of a protected specimen brush and quantitative culture techniques in 147 patients. Am Rev Respir Dis 138:110–116
Trouillet JL, Guiguet M, Gibert C, Fagon JY, Dreyfuss D, Blanchet F, Chastre J (1990) Fiberoptic bronchoscopy in ventilated patients. Evaluation of cardiopulmonary risk under midazolam sedation. Chest 97:927–933
Djedaini K, Cohen Y, Mier L, Brun P, Gros I, Coste F, Dreyfuss D (1993) Prospective evaluation of the incidence of bacteremia after protected specimen brushing in ICU patients with and without pneumonia. Chest 103:383–385
Legall JR, Loirat P, Alperovitch A et al. (1984) A simplified acute physiologic score for ICU patients. Crit Care Med 12:975–977
Dreyfuss D, Djedaïni K, Weber P, Brun P, Lanore JJ, Rahmani J, Boussougant Y, Coste F (1991) Prospective study of nosocomial pneumonia and of patient and circuit colonization during mechanical ventilation with circuit changes every 48 hours versus no change. Am Rev Respir Dis 143:738–743
Lennette EH, Balows A, Hausler WJ Jr, Shadomy HJ (eds) (1985) Manual of clinical microbiology, 4th edn. American Society of Microbiology, Washington, DC, pp 309–399
Roberts RB (1985)Streptococcus pneumoniae. In: Mandell GL, Douglas RG Jr, Bennett JE (eds) Principles and practice of infectious diseases, 2nd edn. Wiley, New York, pp 1142–1152
Kanter RK, Carroll JL (1983) Early pneumococcal sepsis after pulmonary aspiration and the adult respiratory distress syndrome. Crit Care Med 11:906–907
Mandelli M, Mosconi P, Langer M, Cigada M and Intensive Care Unit Group of Infection Control (1989) Prevention of pneumonia in an intensive care unit: a randomized multicenter clinical trial. Crit Care Med 17:501–505
Johanson WG, Jay SJ, Pierce AK (1974) Bacterial growth in vivo. An important determinant of the pulmonary clearance of diplococcus pneumoniae in rats. J Clin Invest 53:1320–1325
Bordelon JY, Legrand P, Gewin WC, Sanders CV (1983) The telescoping plugged catheter in suspected anaerobic infections. A controlled series. Am Rev Respir Dis 128:465–468
Dines DE, Titus JL, Sessler AD (1970) Aspiration pneumonitis. Mayo Clin Proc 45:347–360
Bartlett JG, Rosenblatt JE, Finegold SM (1973) Percutaneous transtracheal aspiration in the diagnosis of anaerobic pulmonary infection. Ann Intern Med 79:535–540
Bjerkestrand G, Digranes A, Schreiner A (1975) Bacteriological findings in transtracheal aspirates from patients with chronic bronchitis and bronchiectasis. A preliminary report. Scand J Respir Dis 56:201–207
Bartlett JG (1977) Diagnostic accuracy of transtracheal aspiration bacteriologic studies. Am Rev Respir Dis 115:777–782
Higuchi JH, Coalson JJ, Johanson WG (1982) Bacteriologic diagnosis of nosocomial pneumonia in primates. Usefulness of the protected specimen brush. Am Rev Respir Dis 125:53–57
Wimberley NW, Bass JB, Boyd BW, Kirkpatrick MB, Serio RA, Pollock HM (1982) Use of a bronchoscopic protected catheter brush for the diagnosis of pulmonary infections. Chest 81:556–562
Dreyfuss D, Mier L, Le Bourdelles G, Djedaïni K, Brun P, Boussougant Y, Coste F (1993) Clinical significance of borderline quantitative protected brush specimen culture results. Am Rev Respir Dis 147:946–951
Johanson WG, Pierce AK, Sanford JP (1969) Changing pharyngeal bacterial flora of hospitalized patients. Emergence of gram-negative bacilli. N Engl J Med 281:1137–1140
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Mier, L., Dreyfuss, D., Darchy, B. et al. Is penicillin G an adequate initial treatment for aspiration pneumonia?. Intensive Care Med 19, 279–284 (1993). https://doi.org/10.1007/BF01690548
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF01690548