Article Text

Statistics from Altmetric.com
CLINICAL PRESENTATION
A 14-year-old boy was transferred to our paediatric referral centre with a 1-day history of worsening respiratory distress. He had initially presented to a community hospital complaining of dyspnoea, cough and emesis, and was treated with antibiotics and methylprednisolone prior to transfer. He was taking no other medications and his history was notable only for mild wheezing as a young child. He lived in a rural wooded area in the eastern USA and reported riding his motorcycle on dusty roads. He reported inhaling second-hand cigarette smoke on the night prior to presentation.
His temperature on presentation was 37.2°C with mild tachycardia. His respiratory rate was 24 breaths/min with bilateral wheezes and decreased air movement at the right base. His oxygen saturation was 89% when breathing room air. The initial white blood cell count was 31 230/mm3 with 94% neutrophils. A chest radiograph showed interstitial infiltrates in the left upper and right lower lobes.
He was treated with antibiotics for presumptive severe community-acquired pneumonia. His respiratory distress and hypoxaemia worsened so he was placed on BiPAP. A subsequent chest radiograph showed worsening bilateral infiltrates with consolidation in the right middle lobe and the appearance of a pleural effusion. Extensive testing failed to reveal an infectious cause.
Owing to his worsening clinical status, evolving infiltrates and lack of a clear aetiology, flexible bronchoscopy with bronchoalveolar lavage (BAL) and transbronchial biopsy was performed 2 days after presentation. The diagnosis was suggested by initial examination of the BAL fluid and confirmed by further testing including histological examination (fig 1).

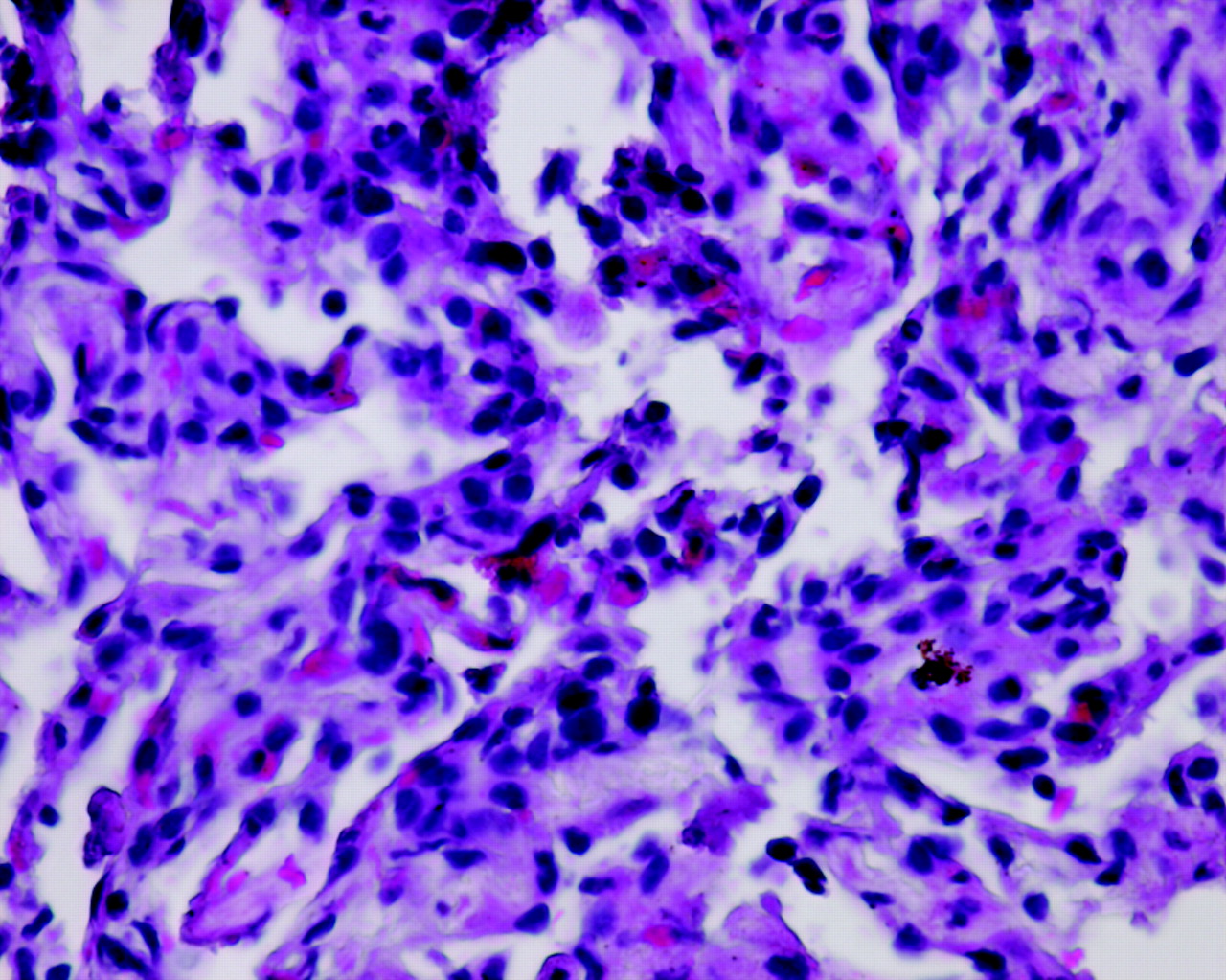{kind=link}
H&E stain of transbronchial biopsy specimen (40× magnification).
QUESTION
What is the aetiology of this patient’s evolving infiltrates and worsening respiratory status?
See page 364.
This case was submitted by:
Parental/guardian consent obtained.
Linked Articles
- Pulmonary puzzle