Article Text

Abstract
Aim: Tumour necrosis factor α (TNFα) is a cytokine recognised as a therapeutic target in chronic inflammatory diseases.
Methods: A randomised, double blind, placebo controlled parallel group trial is reported of etanercept (an IgG1-TNF p75 receptor fusion protein), administered once weekly for 12 weeks in 39 patients with severe corticosteroid refractory asthma. Efficacy was measured by change from the pretreatment baseline in Asthma Related Quality of Life (AQLQ) and Asthma Control (ACQ) Questionnaire scores (the primary endpoints), lung function, peak expiratory flow (PEF) and bronchial hyperresponsiveness (BHR). Sputum and serum inflammatory cells and cytokines, serum albumin and C reactive protein (CRP) as biomarkers of inflammation were also assessed.
Results: There was a small but significant difference in reduction of ACQ scores between treatment and placebo (−1.11 (95% CI −1.56 to −0.75) and −0.52 (95% CI −0.97 to −0.07), respectively, p = 0.037). There was no significant difference in improvements in AQLQ scores, lung function, PEF, BHR or exacerbation rates between the groups. Minor adverse events, including injection site pain and skin rashes, were more frequent with etanercept. There was a significant reduction in sputum macrophages and CRP, and increases in serum TNFα and albumin following treatment, but not in other laboratory parameters.
Conclusion: Etanercept therapy over 12 weeks demonstrated only a small but significant improvement in asthma control and systemic inflammation, as measured by serum albumin and CRP. Larger randomised, placebo controlled trials are required to clarify the role of TNFα antagonism in subjects with severe refractory asthma.
Statistics from Altmetric.com
Asthma is a disorder of the conducting airways characterised by variable airflow obstruction and increased bronchial hyperresponsiveness (BHR) to a range of environmental stimuli. In the majority of patients, mild to moderate asthma airway dysfunction is usually responsive to inhaled corticosteroids that form the mainstay of therapy. As the disease becomes more severe and chronic, it adopts a more aggressive phenotype with evidence of neutrophil infiltration and airway wall remodelling.1 ,2 Patients with asthma with this severe phenotype respond poorly to standard treatments and many are not adequately controlled despite regular systemic corticosteroids and good adherence.3 We have proposed that these changes in asthma phenotype may reflect expression of an additional Th1 inflammatory profile with increased production of tumour necrosis factor α (TNFα), a multifunctional cytokine that augments the activity of many cells implicated in the pathogenesis of asthma, including immune, inflammatory, smooth muscle and epithelial cells.4 A case has been made for TNF as a mediator of asthma in humans where inhaled TNFα causes transient BHR and an influx of neutrophils into the airways.5 Genetic polymorphism of the TNFα gene on chromosome 6 is also associated with asthma, its accompanying severity and BHR.6 ,7
The potential importance of TNF in severe refractory asthma has recently been strengthened by two small clinical trials of etanercept, a p75 IgG1 fusion protein that binds both TNFα and TNFβ, thereby preventing interaction with its cell bound high (p75) and low (p55) affinity receptors. In the first open labelled study on 15 patients, etanercept (Enbrel) 25 mg administered subcutaneously twice weekly for 12 weeks led to a marked reduction in symptoms and BHR but only moderate changes in baseline forced expiratory volume in 1 s (FEV1).4 The second, a crossover, placebo controlled study on 10 patients with refractory asthma using the same regimen for 10 weeks produced almost identical findings, but in addition revealed a substantial increase in Asthma Related Quality of Life (AQLQ) and that circulating mononuclear cell membrane associated TNFα was not only selectively elevated in severe asthma but also predicted the clinical response to etanercept.8 A third parallel group randomised controlled trial of the TNF blocking antibody Infliximab in less severe asthma revealed significant protection against exacerbations of asthma and other endpoints, but failed to achieve significance in the primary endpoint of morning peak expiratory flow (PEF).9
In other chronic inflammatory diseases such as rheumatoid arthritis and psoriasis, TNF blockade has been especially effective in relieving systemic manifestations of the disease, measured by changes in quality of life, fatigue, anxiety and depression scores.10 Here we describe a parallel group randomised controlled trial with etanercept in severe refractory asthma in which asthma control and related quality of life were selected as the primary clinical endpoints. We also measured a number of biomarkers of inflammation in both blood and sputum.
MATERIALS AND METHODS
Patients
The majority of patients were recruited from two difficult asthma clinics at Southampton General and Queen Alexandra Hospitals, and others from Dorset General and St Mary’s Isle of Wight Hospitals, UK. Asthma was confirmed by the presence of objective assessments of variable airflow obstruction and/or BHR. This included an increase in FEV1 by at least 12% after inhalation of 400 μg of salbutamol delivered by a metered dose inhaler and spacer, the concentration of methacholine required to cause a 20% (PC20) reduction in FEV1 of <8 mg/ml (the latter only if subjects had a predicted FEV1 of >50%). All patients also met the Global Initiative for Asthma criteria for severe refractory asthma, which included current treatment with oral prednisolone (2–30 mg/day) and/or high dose inhaled corticosteroids (>2000 μg/day beclomethasone equivalent) and long acting β2 adrenoceptor agonists. A high proportion of patients received one or more theophyllines, leukotriene receptor antagonists and nebulised salbutamol. Current smokers, subjects with a smoking history of >10 pack years, other coexisting lung disease, a history of tuberculosis, multiple sclerosis, systemic lupus erythematosus or other autoimmune diseases were excluded. Patients were also excluded from participation if they had a history of upper respiratory tract infection within 2 months, evidence of tuberculosis (PPD skin test >10 mm or positive chest x ray), history of opportunistic infections within the previous 6 months, previous malignancy and/or a history of lymphoproliferative disease. All patients were considered compliant with treatment by cross checking GP prescription records or measurement of serum theophylline levels as appropriate on a central primary and secondary care database. Patients thought to have uncontrolled asthma as a consequence of coexistent conditions such as gastro-oesophageal reflux, rhinitis or occupational triggers were also excluded. Subjects were asked not to alter any regular controller asthma medications during the study, although they were allowed to adjust reliever medication use as necessary. Patient characteristics at baseline are shown in table 1.
Study design
This was a double blind, parallel, randomised, placebo controlled trial, which was approved by the SE Hampshire and Isle of Wight Research Ethics Committee, and all patients provided informed consent. The trial was investigator initiated and the sponsors were not involved in the study design, data collection, analysis or interpretation of the data. Sample size methods are given in the appendix (available online). Patients attended the clinic for a screening visit followed by an entry visit after a minimum 2 week run-in period for baseline measurements and to confirm eligibility. The study plan is given in fig 1. Patients were randomly allocated at visit “0” to receive 50 mg of etanercept or matched placebo by subcutaneous injections once a week for 12 weeks as add on therapy to their current medication. Selection of the dose and duration of treatment were chosen from initial proof of concept studies of etanercept in severe asthma4 ,8 and from the recent observation in patients with active rheumatoid arthritis.11 Weekly physiological measurements and diary card collections were made on the day of the visit for treatment, which was administered by the investigators/nursing staff. Randomisation was undertaken by Wyeth Pharmaceuticals (Taplow, Berks, UK) using a permuted blocks of four method. All patients were followed-up 4 weeks after completion, and no change was made to the subjects’ regular asthma medication during the 12 week treatment period.

Asthma Quality of Life and Control Questionnaires
The AQLQ was assessed at baseline and at the end of the treatment phase, and the Asthma Control Questionnaire (ACQ) at each weekly visit. A lower AQLQ score indicated increased impairment, and a higher ACQ score indicated worsening asthma control (questionnaire details are covered in the appendix online).
Lung function
Baseline lung function was recorded as FEV1, forced vital capacity (FVC) and expiratory ratio (FEV1/FVC) using a Vitalograph Compact Spirometer (Vitalograph Medical Instrumentation, Buckingham, UK) at baseline and at weekly intervals throughout the trial. The forced expiratory flow between 25% and 75% of FVC (FEV25–75, using Vitalograph Electronic Compact II spirometer; Vitalograph Medical Instrumentation, Kansas, USA) was measured at baseline and at the end of treatment. Daily diary cards were used to monitor morning and evening PEF using the Wright mini peak flowmeter (Clement Clark International Ltd, Harlow, UK).
Bronchial hyperresponsiveness (BHR)
BHR to inhaled methacholine was measured using the 5 breath procedure (described by Chai and colleagues12) at visits 0 and 12. For safety reasons, the test was conducted only on subjects whose FEV1 was >50% predicted. Detailed methods are given in the appendix online. The effect of treatment on BHR was expressed as the change in doubling dilutions of methacholine required to achieve a 20% fall in FEV1 before and after 12 weeks of treatment, logarithmically transformed and a group mean derived.
Sputum and serum biomarkers of inflammation
Venous blood collected at baseline and at the end of the treatment was stored at −80°C. Sputum induction was performed as previously described with aerosolised hypertonic (4.5%) saline using an ultrasonic nebuliser (Devilbliss Ultraneb 2000, Pennsylvania, USA).13 For safety reasons, sputum induction was not undertaken on subjects with a baseline FEV1 <45% of predicted. Details on methods of sputum and serum markers can be found in the appendix online.
Statistical analyses
The primary endpoints were the differences in change in the mean score from baseline (visit 0) and the end of treatment (visit 12) on the AQLQ, and change in mean scores from baseline and the last two treatment visits (visits 11 and 12) for the ACQ. Secondary endpoints were similar differences from baseline to visit 12 for BHR, and to the last two treatment visits for predicted FEV1, FEV1/FVC, morning, evening and average daily PEF, and diurnal variation in PEF (calculated by the difference in the evening and morning PEF values). Differences from baseline for laboratory parameters in sputum and serum were similarly analysed.
The distributions were assessed for normality by Shapiro–Wilks tests and measurement of equality of variance ratios by F tests. Differences between groups in clinical and laboratory outcomes with a normal distribution were compared using unpaired Student’s t tests or the Mann–Whitney U test for non-normal distributions. The data were analysed using Stata version 8 (Stata Corporation, College Station, Texas, USA) and Statview Version 5.1 (SAS Institute, Cary, North Carolina, USA). For missing data the intention to treat methodology was used with missing values being ascribed by last observation carried forward.
The proportion of patients experiencing exacerbations, adverse events or withdrawing from nebulised β2 agonists between treatment and placebo groups were compared by 2×2 contingency tables using χ2 tests. We also explored relationships between baseline characteristics, sputum or serum markers, or changes in these parameters with the changes in the primary and secondary endpoints by analyses of variance.
RESULTS
Baseline characteristics
A total of 59 patients were screened, 39 were enrolled in the study and 19 patients were randomised to active treatment. Overall, there were 20 patients who were excluded after screening (fig 2). Details of age, gender, duration of asthma, lung function at baseline medication usage and other characteristics are shown in table 1. There were three withdrawals, two in the placebo group at weeks 4 and 8 because of “ineffectiveness of treatment” and one in the etanercept group at week 10 as a result of work related stress. Overall, comparison of baseline values of AQLQ, ACQ, lung functions and PC20 were not significantly different between the two treatment groups (p>0.05 for all variables, table 1). Data for AQLQ, ACQ and lung function before and at the end of treatment were available in all patients completing the study. Missing diary card data for PEF was <5%.

Asthma Quality of Life and Control Questionnaires
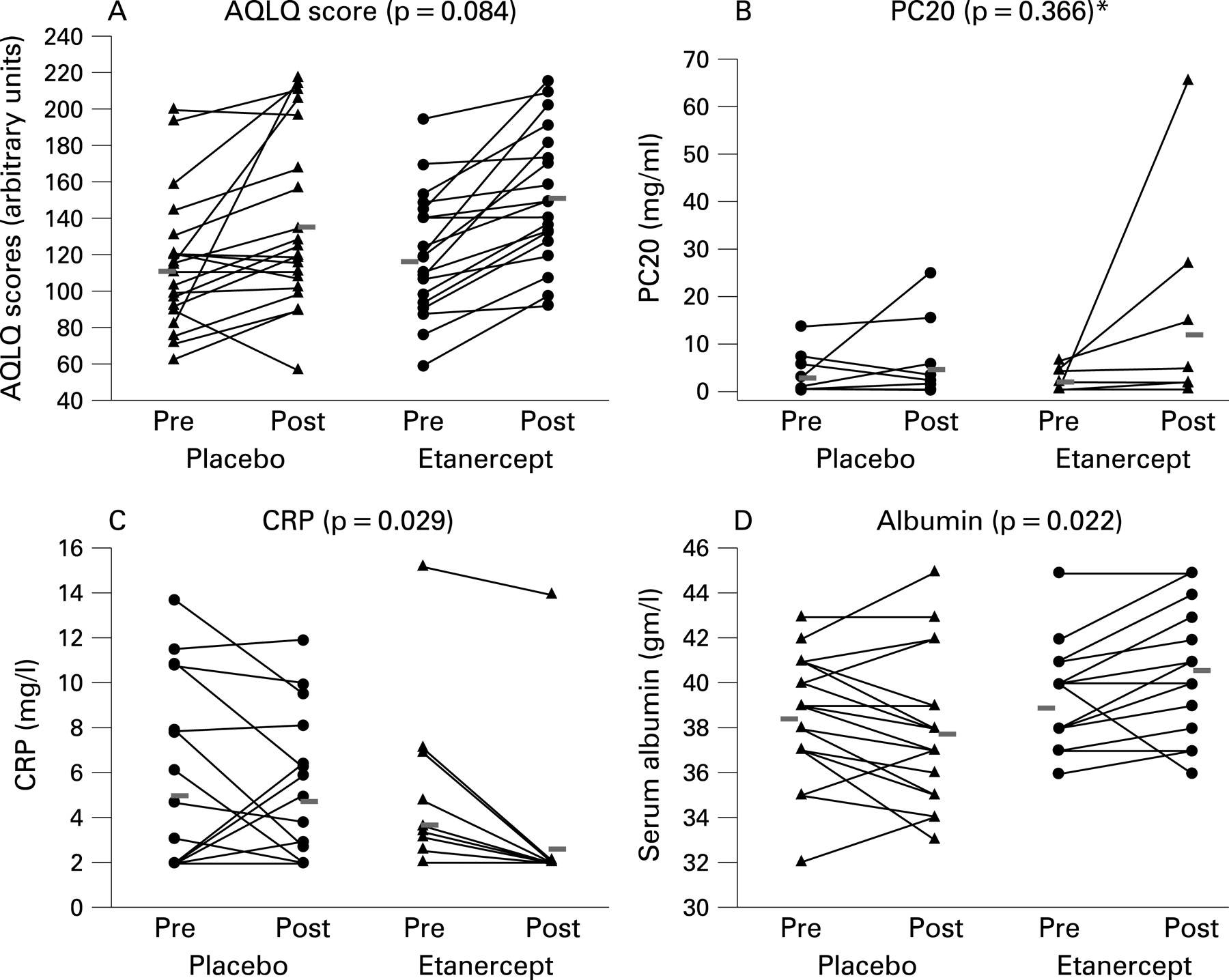
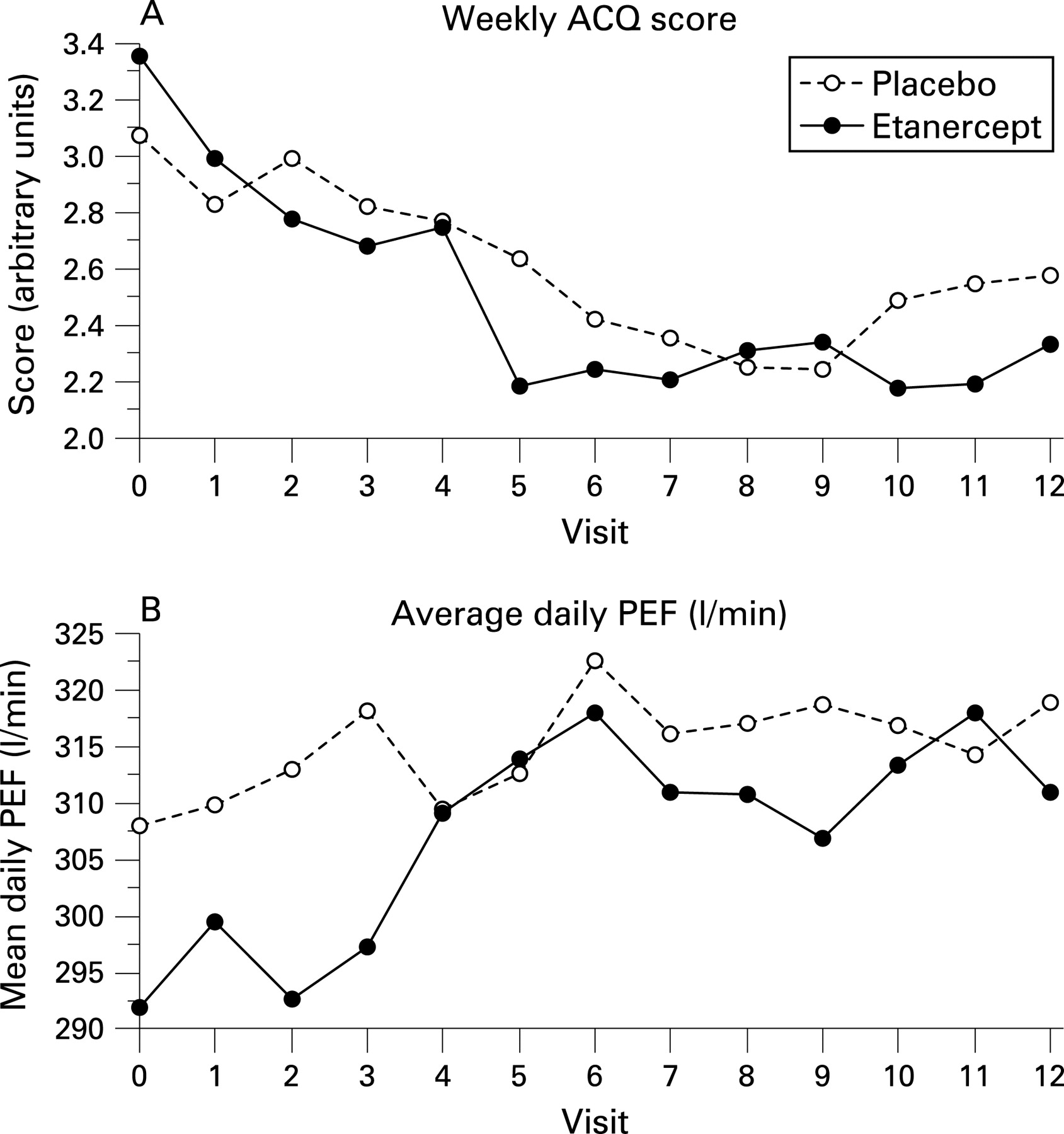
Of the two primary endpoints, there were increases in mean AQLQ scores for both treatment (1.03, 95% confidence interval (CI) 0.64 to 1.39) and placebo (0.68, 95% CI 0.14 to 1.23) but the difference between groups was not significant (p = 0.084) (see fig 3A, table 2). There was however a significant difference in reductions in mean ACQ scores between treatment (−1.11 (95% CI −1.56 to −0.75)) and placebo (−0.52 (95% CI −0.97 to −0.07); p = 0.030) (fig 4A, table 2).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Lung function and PEF
There were small increments in FEV1, per cent predicted FEV1 and FEV25–75 in the etanercept group compared with the placebo group (where there were corresponding decrements), but the differences between groups were not significant (table 2). There were no significant differences in change in morning or evening PEF, or diurnal variation in PEF. The forced expiratory ratio (FEV1/FVC) improved in both groups over the study period although the difference was not significant. The average daily PEF (l/min) also improved over the study period although the difference in improvements between groups was not significant (fig 4B, table 2).
Bronchial hyperresponsiveness
Methacholine bronchoprovocation was performed in 13 patients in the placebo and 11 patients in the etanercept group. There was a greater improvement in PC20 in favour of etanercept compared with placebo, but the differences between groups were not significant (fig 3B, table 2).
Sputum and serum biomarkers of inflammation
Sputum analyses were performed in eight patients in each group (table 2). The differences in numbers of paired serum and sputum samples available for analysis relate to difficulties in venous sampling, quality of specimens and prioritisation of tests for less sufficient clinical samples. Serum TNFα levels were very low at baseline in most of the patients studied but increased dramatically after 12 weeks of etanercept but not placebo treatment (p<0.001) (table 2). There was a significant reduction in CRP in the etanercept group (−1.162 mg/l (95% CI −2.003 to −0.321)) compared with placebo (−0.286 g/l (95% CI −1.706 to 1.134); p = 0.029) (fig 3C), and a significantly greater improvement in serum albumin in the etanercept group (1.00 g/l (95% CI 0.12 to 1.87)) compared with placebo (−0.47 g/l (95% CI −1.43 to 0.49); p = 0.022) (fig 3D, table 2).
Levels of interleukin (IL)6 and IL1β in sputum supernatants were reduced following treatment in the etanercept group but the differences between groups were not significant. There was a small but non-significant increase in sputum eosinophils and neutrophils in the etanercept group. There was a significant reduction in sputum macrophages in the etanercept group (−0.09×106/g (IQR −0.265 to −0.008) compared with placebo (0.11×106/g (IQR −0.033 to 0.195); p = 0.017) (table 2).
Other events
There were seven subjects in each group who required regular high dose nebulised salbutamol (table 1). Four subjects in the etanercept group voluntarily discontinued their nebulised bronchodilators by the end of the study compared with none in the placebo group (p = 0.018). There were equal numbers of asthma exacerbations and upper respiratory tract infections in both treatment groups. Other reported adverse events were mild but local injection site reactions, and skin rashes were more common in the etanercept group (p = 0.014 and p = 0.030, respectively). One patient in each group was admitted to hospital for exacerbation of asthma, with a hospital length of stay of less than 48 h for both. There were no other serious adverse events. Details on adverse events are in the appendix online.
Follow-up
The majority of patients had changes in AQLQ and ACQ scores, and reductions in daily PEF and FEV1 commensurate with deterioration in asthma control and quality of life 4 weeks after the study, but the differences between groups were not significant (data not shown). There were also no serious or minor adverse events at follow-up.
DISCUSSION
This study of etanercept in patients with severe refractory asthma has shown an improvement in one of our two primary endpoints. There was a small but significant improvement in asthma control assessed by questionnaire (ACQ) but not AQLQ after 12 weeks of treatment. There were no improvements in the secondary endpoints of lung function, PEF or BHR (in the small number of subjects in whom challenge was possible). There were no serious adverse events, although minor injection site reactions and skin rashes were more common in the etanercept group, and the rate of exacerbations of asthma was the same in both groups.
It is possible that those patients in the etanercept group reporting voluntary withdrawal of nebulised bronchodilators at the end of the study (compared with none on placebo) could have augmented the observed improvement in AQLQ and ACQ scores. The time course over which changes after etanercept therapy may occur are not known, although based on our previous study and a recent small crossover trial of etanercept in severe refractory asthma which demonstrated improvements after 10 weeks of therapy, we sought to examine similar changes in outcome after 10 weeks by comparing differences from baseline with the mean of weeks 11 and 12, rather than week 12 alone. The treatment duration was chosen based on the previous trials with etanercept4 ,8 and initial trials in rheumatoid arthritis where etanercept was used as a treatment option for 12 weeks.14 Also, administration of treatment once weekly was based on prior studies in rheumatoid arthritis.11 The majority of patients were recruited mainly from two centres, and assessment of recruitment site showed no interaction with any of the outcomes or treatment effects in analyses of covariance with a full effects model (data not shown).
Improvements in the primary and secondary endpoints were seen in both the placebo and treatment groups, although only differences in ACQ scores were significantly different between the groups. A within group change of 0.5 in scores on the ACQ (and AQLQ) is considered clinically significant15 ,16 and we found a between group difference of 0.59. Increased compliance with treatment on recruitment into the study is unlikely to explain the discrepancy as we checked compliance by examining prescription records, clinic attendances and pre-enrolment blood tests, and excluded two patients in the screening period in whom non-adherence to therapy was thought to be significant. Alternatively, it is probable that patients affected by depression as a result of their underlying chronic medical condition are more likely to experience high placebo response rates (see post hoc analyses in the appendix online).17 ,18 When the observations were restricted to patients not taking antidepressants, the differences in improvement in both ACQ and AQLQ scores became more significant between etanercept and placebo compared with differences when the groups were combined. We observed between group differences in ACQ and AQLQ scores of 0.93 and 0.58, respectively, both above the minimal important changes. Despite the potential limitations of such a post hoc analysis, this finding leads us to suggest that future trials of severe refractory asthma should evaluate coexistent depression and anxiety in this subgroup of asthma patients, in addition to asthma specific measures such as the AQLQ and ACQ.
We had calculated the sample size in our study on expected differences in AQLQ and ACQ based on our previous study, but a large proportion of patients enrolled into the study remained too severe to have safely performed methacholine challenge. Therefore, the effect on methacholine BHR may have been underestimated because of the small numbers, even though some patients in the etanercept group showed significant “within patient” differences. It is possible that the improvements in lung function were also not demonstrated because the sample size was calculated on other primary endpoints. Furthermore, it is unlikely we included any patients with hitherto unrecognised chronic obstructive pulmonary disease as the diagnosis of asthma was confirmed in each patient and smokers were excluded. However, we studied patients with asthma with very severe airflow obstruction (mean per cent predicted FEV1 58–59%) and it is possible that we included some with “fixed” airflow obstruction as we did not perform assessments of “corticosteroid responsiveness” in the screening or recruitment period.3 If the airway obstruction was relatively fixed this would reduce the possibility of any improvement. Another possible explanation is that the study measured the post-bronchodilator FEV1 at each visit, and if patients confirmed having taken a short acting β2 adrenoceptor agonist within an hour of the visit, a further bronchodilator was not administered again; we therefore could not prove with certainty that every measurement of FEV1 was after a bronchodilator.
The disparity between impacts on quality of life and disease control in severe asthma and lack of efficacy in lung function has been highlighted in clinical trials of other biological therapies such as anti-IgE treatment.19 ,20 We have similarly demonstrated significant improvements in asthma control and quality of life (in patients not on antidepressants), but not lung function. Trials of etanercept in other chronic diseases such as rheumatoid arthritis and psoriasis10 have also revealed a disproportionate effect on symptoms or quality of life scores, raising the possibility that in these disorders as well as in asthma TNFα generated in the inflamed organ may have systemic or extrapulmonary effects21 and that the discrepancy between quality of life and lung function in severe asthma have different mechanisms of effect.22 We measured the acute phase reactants CRP and albumin as surrogates of systemic inflammatory activity, and confirmed that levels of CRP decreased by a mean 1.162 mg/l and serum albumin increased by a mean 1 g/l in the etanercept group compared with placebo. Both changes occurred within the normal range for healthy adults, using robust assays applicable to most hospital laboratories, even though it is recognised that standard assays for CRP may not be sensitive enough to detect levels of systemic inflammation close to the normal range, as in this study. Other studies have recently reported elevated levels of CRP in mild “corticosteroid naïve” asthma23 and chronic obstructive pulmonary disease,24 and further investigation of this effect in severe asthma using high sensitivity CRP assays are warranted. Our results indicate reduced systemic inflammation with etanercept therapy in asthma, in keeping with similar observations of reduced CRP in rheumatoid arthritis and ankylosing spondylitis after TNF blockade.25 ,26 In this study, the baseline serum CRP or albumin did not predict any of the clinical responses. Overall, these observations support the view that refractory asthma may be a systemic inflammatory disorder and that TNF blockade may be important in the systemic manifestations of the disease.
Despite previously having shown that TNFα is increased in bronchoalveolar lavage fluid (BALF) and bronchial biopsies in patients with severe asthma,4 in keeping with others,27 we were unable to detect any TNFα in the sputum of patients despite the high sensitivity and specificity of the assays. One explanation for this is the effects of dithioerythritol or other media used in recovery of mediators in sputum, which can reduce cytokine recovery.28 We were able to detect other cytokines (IL6, IL8 and IL1β) in preference to TNF, suggesting this effect of laboratory processing less likely. We did nevertheless detect highly immunoreactive TNFα in serum after etanercept therapy compared with placebo, which most likely represents TNFα bound to the etanercept fusion protein,29 but not in the sputum following treatment. This demonstrates that while we were unable to detect this cytokine in the circulation at baseline, etanercept therapy was very effective in binding to TNFα to render it biologically inactive and is consistent with similar observations in the BALF of patients with mild asthma treated with etanercept.29 Previous studies have suggested that elevated levels of IL6 and IL1β in BALF is indicative of symptomatic asthma,30 and in this study levels of IL6, IL8 and IL1β were all reduced in the sputum of patients treated with etanercept compared with placebo, although none was significant. This is consistent with our previous observations and that of others.8 One point of interest is that sputum macrophages were significantly reduced in the etanercept group compared with placebo, while small but non-significant increases in eosinophils and neutrophils were observed in patients after etanercept therapy. The level of sputum macrophages at baseline did not consistently influence any of the main outcomes in the small numbers of patients with available data.
Etanercept treatment was generally well tolerated with no serious adverse events other than one patient in each group admitted to hospital for an exacerbation of asthma. There was however a small increase in local injection site and skin reactions in the etanercept group. We also evaluated the number of asthma exacerbations and upper respiratory infections, and did not find any differences between groups, in contrast with another recent study of anti-TNF therapy in less severe asthma.9
In summary, this randomised controlled trial adds some support for the role of TNFα in the pathogenesis of severe corticosteroid refractory asthma. It confirms small improvements in asthma control and systemic inflammation after 12 weeks of etanercept therapy compared with placebo. Larger multicentre, placebo controlled, randomised controlled trials adequately powered for each clinical outcome, especially BHR, are now required to evaluate this therapeutic option in patients with severe asthma.
Acknowledgments
We thank Lesley-Ann Vickers, Louisa Little, Malcolm North, Sandy Smith and Sumita Kerley, for their invaluable assistance in conducting this trial. We are also grateful to Dr D Murphy and his team at the St Mary’s Hospital, Isle of Wight. We are thankful to Wyeth Laboratories for providing the drugs (placebo and etanercept) free of cost and for the educational grant for the clinical research fellow (JM) and nursing staff. We are grateful to Drs LC Lau and J Ward for help with the laboratory analyses, and to Drs P Vijayanand and D Bagmane for their help in clinical supervision during the study. We would also like to thank Mr B Higgins from the Department of Mathematics, University of Portsmouth, for guidance on the statistical analyses. We also thank Dr H Arshad and Professor R Djukanovic for help in planning this study.
REFERENCES
Supplementary materials
web only appendix 63/7/584
Files in this Data Supplement:
Footnotes
See Editorial, page 571
The appendix is published online only at http://thorax.bmj.com/content/vol63/issue7
Normal range: The normal ranges of serum C reactive protein and albumin described in this study are <7.5 mg/l and 35–48 g/l in healthy adults.
JBM and AJC contributed equally to the study.
Contributors: STH, DED, AJC, JM and KSB contributed to the concept and design of the study. JM, AJC, RP, DED and STH contributed to the analysis and interpretation of data. STH was principal investigator; DED, RD, JM and AJC were coinvestigators. AJC, JM, RP and STH drafted the article and revised it critically for intellectual content. JM and AJC conducted and supervised the study at the clinical sites.
Funding: This study was supported by an educational grant from Wyeth Pharmaceuticals, UK, and they were not sponsors of the study. The trial was investigator initiated and the sponsors were not involved in the study design, data collection, analysis or interpretation of the data. A copy of the manuscript was nonetheless sent to Wyeth before submission. STH is a UK Medical Research Council funded Clinical Professor.
Competing interests: This study was performed with an educational grant from Wyeth Pharmaceuticals. All authors confirm (except JM and STH, see below) that they are not involved in any organisation or entity with a financial interest in or financial conflict with the subject matter or materials discussed in this manuscript. JM was funded by the educational grant to conduct this study. AJC in the past 5 years has received research funding, honoraria for lectures and educational grants from Astra Zeneca, GlaxoSmithKline, Boehringer Ingelheim and Merck, and has been on advisory boards for Astra Zeneca and GlaxoSmithKline. STH is a consultant for Novartis, Synairgen, Merck, Wyeth and Centocor. STH has received lecture fees from their companies. RP is a consultant for Cardiovascular Therapeutics, Duska Therapeutics and NeuroSearch, and has received lecture fees from Merck and Novartis.
Ethics approval: The trial was approved by the SE Hampshire and Isle of Wight Research Ethics Committee.
Linked Articles
- Editorials
- Airwaves