Article Text

Abstract
Introduction Early infant diet might influence the risk of subsequent allergic disease.
Methods The Merthyr Allergy Prevention Study (MAPS) was a randomised controlled trial in infants at high risk of allergic disease. The trial determined whether a cow’s milk exclusion diet for the first 4 months of life decreased the risk of allergic disease including asthma compared with a normal diet. A soya milk preparation was offered to those in the intervention group. A standardised questionnaire for allergic disease was completed at ages 1, 7, 15 and 23 years, with clinical assessment at 1, 7 and 23 years. The effect of the intervention on the risk of atopy, asthma and wheeze at age 23 years was determined.
Findings 487 subjects entered the study; at age 23 years 299 completed the questionnaire, of which 119 attended clinical assessment. Subjects randomised to the intervention group had a significantly increased risk of atopy (adjusted OR 2.97, 95% CI 1.30 to 6.80; p=0.01) and asthma (OR 2.07, 95%CI 1.09 to 3.91; p=0.03) at age 23 years, but not wheeze (OR 1.43, 95%CI 0.87 to 2.37; p=0.16). Earlier exposure to cow’s milk was associated with a decreased risk of wheeze and asthma at age 23 years, while earlier exposure to soya milk was associated with an increased risk of atopy and asthma.
Interpretation In infants at high risk of allergic disease, either cow’s milk exclusion or early soya milk introduction for the first 4 months of life increases the risk of atopy, wheeze and asthma in adulthood.
- asthma
- paediatric asthma
Data availability statement
Data are available upon reasonable request.
Statistics from Altmetric.com
Key messages
What is the key question?
Does cow’s milk avoidance in the first year of life decrease the risk of asthma and allergy in adulthood?
What is the bottom line?
Cow’s milk avoidance (or early soya milk exposure) was associated with an increased risk of asthma and atopy in adulthood.
Why read on?
This trial provides further evidence that delayed exposure to foodstuffs in infancy increases the risk of allergic disease later in life.
Introduction
The prevalence of allergic diseases, including asthma, eczema, allergic rhinitis and food allergy, has increased significantly over the past few decades.1 2 Although there is a strong familial component with an increased risk of both atopy and asthma if either parent has asthma,3 genetic change alone cannot explain the magnitude of effect. Attention has therefore focused on environmental changes, particularly during early life, that might affect the incidence of allergic disease4 including urban affluent lifestyles, environmental and microbial exposures,5 or changes in diet including maternal diet and breastfeeding.6 The identification of contributory risk factors offers the possibility of primary prevention of allergic disease7 through modulation of the early life environment, particularly if one or more parent is allergic. It is thought that the window of opportunity for allergy prevention falls between conception and the first 6 months after birth.7
More than 80 years ago it was first suggested that infants fed cow’s milk formulae had an increased incidence of allergic disease8. Since then, the prevalence of breast feeding in westernised countries has diminished with a concomitant increase in the use of formula feeds. Most studies of breast feeding report a decreased risk of eczema and viral wheezing early in childhood,6 9 but a possible increased risk of asthma in late childhood. Symptomatic cow’s milk allergy occurs in 2–3% of infants in developed countries,10 with a lifetime prevalence of 6%.11 Avoidance of cow’s milk in early life was thus a plausible strategy to decrease allergy, with consideration of alternative feeds including hydrolysed cow’s milk formulae and soya based formulae. Soya based formulae appeared less antigenic than cow’s milk,12 with a significantly decreased risk of allergic disease (primarily asthma and allergic rhinitis) in those who received soya milk.13 It is now recognised that soya is also a major antigen with many infants with cow’s milk allergy being allergic to soya as well, and that soya based formulae should not be administered in early infancy.14
Given the concerns over early cow’s milk exposure and the subsequent risk of allergic disease, the Merthyr Allergy Prevention Study (MAPS) was designed to examine whether withholding cow’s milk protein for young infants at high risk of allergy would reduce their subsequent development of allergic disease including asthma. In an open label extension of MAPS we determined the effect of the intervention on the risk of atopy, asthma and wheeze at age 23 years.
Methods
Full reports on methods and randomisation have been published previously.15–17 MAPS was a randomised controlled trial to determine whether avoidance of cow’s milk in early life decreases the likelihood of developing allergic diseases in early childhood. MAPS was aimed at infants at high risk of developing allergic disease—all had a first degree relative (parent or sibling) with a history of eczema, asthma or hay fever. Potential mothers of eligible infants were recruited at antenatal clinics in a socially deprived area of the South Wales valleys and randomised prior to delivery. Although MAPS did not reach its primary aim of decreasing allergic disease in the first year of life,15 the cohort was subsequently reviewed at regular intervals as an open label follow-up study.
Mothers whose infants were randomised to the intervention group were asked to restrict their cow’s milk intake to half a pint (284 mL) per day for the remainder of the pregnancy, and while they breast fed. Additionally they were asked not to give cow’s milk, or any food made from cow’s milk, to the child for at least the first 16 weeks of the child’s life. For those who did not wish to breast feed, or wanted to supplement breast feeding, a standardised soya milk preparation was provided. Pregnant women randomised to the control group had no restrictions on their cow’s milk intake either during or after pregnancy. Those who did not wish to breast feed were given a standard cow’s milk formulation while in hospital, after which they purchased their preferred formulation.
Baseline demographics were recorded, including social class using the Registrar General’s classification of occupations.18 During the first 26 weeks of life mothers recorded daily food diaries with weekly assessments at home from study dietitians. Age in weeks of the first consumption of cow’s milk and soya milk was recorded. Parents, and later subjects, were asked to complete a standardised questionnaire for allergic disease at age 1, 7, 15 and 23 years. Subjects had a clinical assessment by a clinician (blinded to randomisation group) including skin prick testing to common allergens (house dust mite, grass, tree, moulds, cat, dog, peanut, milk and egg) at 1, 7 and 23 years of age, and blood was taken for measurement of total IgE at 3 months, 7 and 23 years. Milk and soya specific IgE and IgG4 were measured at 3 months. The intention was to take blood at 1 year of age, but due to infant and maternal distress, collection was discontinued after 60 infants were sampled. IgE was measured by radio-allerogosorbent assay at 3 and 12 months, and by enzyme immune assay at 7 years of age. IgG4 was measured by radio-immunoassay. Wheeze was defined as answering ‘yes’ to the question ‘Have you (Has your child) had wheezing or whistling in the chest in the past 12 months?’.19 Asthma was defined as ever having had asthma and reporting wheeze in the past year.19 Atopy was defined as at least one positive skin prick test (weal size 3 mm>negative control). Ever breast feeding was defined as breast feeding for at least 1 week. For those with incomplete data, it was assumed that those who did not breast feed for the first 2 weeks of life did not breast feed. The mothers provided written informed consent while pregnant before entry into the study. Follow-up at age 23 years was approved by the local research ethics committee and subjects gave written informed consent.
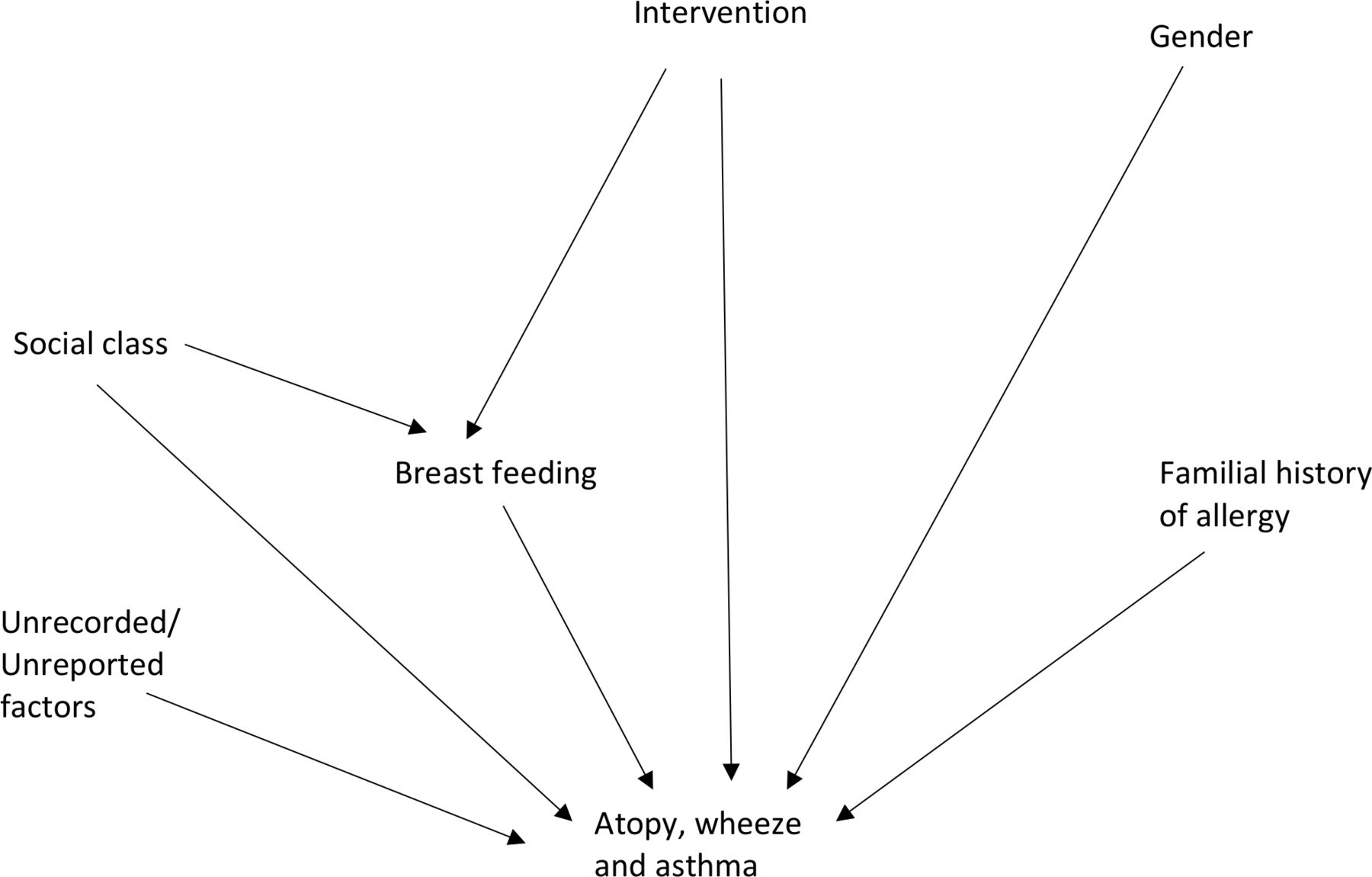
Analysis was by intention to treat (ITT) based on the original randomisation. Effects were modelled using logistic regression, with effect sizes summarised by ORs and 95% CIs. Analyses were adjusted for potential confounders, including social class dichotomised into non-manual and manual workers, gender, parental allergy, randomisation group and breast feeding (figure 1). A per protocol analysis was performed excluding those in the intervention group exposed to cow’s milk in the first 16 weeks of life. Time to first exposure to cow’s milk and also to soya milk during the first 26 weeks of life were modelled using Cox’s proportional hazards model. The Mann-Whitney test was used to compare allergen specific IgG4 and IgE between groups.

Directed acyclic graph for maps.
Results
Between 1982 and 1984, 527 pregnant women consented to the study, and 487 infants were randomised to either the intervention (238) or control (249) group. Full 26 week food diaries were available for 472 (96.9%) infants. The number of subjects at each assessment is shown in figure 2. Of the original 487 subjects, at age 23 years, 129 could not be traced or contacted, and two had died during the trial. Thus, 356 were invited for assessment, of whom 299 completed the questionnaire and 119 attended for clinical assessment. Female subjects were more likely to respond at age 23 years (153/230 (66.5%) vs 146/257 (56.8%); OR 1.51, 95%CI 1.05 to 2.18; p=0.028), while those who wheezed at age 1 year (89/160 (55.6%) vs 200/303 (66.0%); OR 0.66, 95%CI 0.45 to 0.99; p=0.041) or had fathers reported to be unemployed at age 1 year (42/88 (47.7%) vs 249/389 (64.0%); OR 0.51, 95%CI 0.32 to 0.82; p=0.01) were less likely to attend. However, there was no significant difference in response rate between the intervention and the control group (146/238 (61.3%) vs 153/249 (61.4%); OR 1.00, 95%CI 0.70 to 1.45; p=0.98). At age 23 years, 32.8% of subjects reported wheeze, 17.7% reported asthma, and of those who attended for assessment, 59% were atopic.

{kind=link}
{kind=link}
Consort diagram for the maps.
Breast feeding
Of 487 infants, 182 (37.4%) were being breast fed at 1 week of age, 31 of 472 (6.6%) at 16 weeks, and only 11 of 472 (2.3%) were exclusively breast fed for the first 16 weeks. Breast feeding was more common in the control group than in the intervention group (104/249 (42%) vs 78/238 (33%); OR 1.47, 95%CI 1.02 to 2.13), in those who were non-manual workers compared with manual workers (66/119 (56%) vs 114/358 (32%); OR 2.67, 95% CI 1.74 to 4.07), and in those with a history of parental allergy compared with sibling allergy (159/392 (41%) vs 23/95 (24%); OR 2.14, 95% CI 1.28 to 3.56). The effects of breast feeding on subsequent wheeze, atopy and asthma are shown in table 1. Wheeze at age 1 year was significantly less likely in those who were breast fed, but there were no other significant associations.
Association of breast feeding with wheeze, atopy and asthma
Effect of intervention
Of those randomised to the intervention group (cow’s milk free diet), 41 (17.2%) were given cow’s milk before 16 weeks of life, and of those who were randomised to usual diet, 32 (13%) were given soya milk in the first 16 weeks of life. The effect of the dietary intervention is shown in table 2. Subjects randomised to the intervention group had a significantly increased risk of atopy and asthma at age 23 years; the risk of wheeze was increased but not significantly. A per protocol analysis excluding those in the intervention group exposed to cow’s milk in the first 16 weeks of life gave similar results, with an increased risk of atopy (36/51 (70.6%) vs 29/61 (47.5%); OR 2.65, 95% CI 1.21 to 5.80; p=0.015 and asthma (29/125 (23.2%) vs 19/151 (12.6%); OR 2.10, 95% CI 1.11 to 3.96; p=0.022), but again not wheeze (47/125 (37.6%) vs 44/153 (28.8%); OR 1.49, 95% CI 0.90 to 2.47; p=0.12) at 23 years of age.
Effect of randomisation to cow’s milk free diet on wheeze, atopy and asthma
Based on the prospectively collected food diaries for the first 26 weeks of life, earlier exposure to cow’s milk was associated with a significantly decreased risk of wheeze and asthma at age 23 years (table 3); the HR for atopy was very similar, although the sample size was smaller and the result was not statistically significant. Earlier exposure to soya milk was associated with an increased risk of atopy or asthma at age 23 years, with a similar HR for wheeze.
Association of age of first cow’s milk exposure and first soya milk exposure with wheeze, atopy and asthma at age 23 years
Virtually all specific IgE measurements at 3 and 12 months were recorded as the minimum detectable level, and thus the medians in both groups were identical. Median milk IgG4 at 3 months was significantly lower in the intervention group compared with the control group (6.2 vs 12.9 mg/dL; p<0.001). Although the median milk IgG was again lower in the intervention group than the control group at 12 months (10.45 vs 14.75 mg/dL), the numbers are too small to reliably interpret. Median serum total IgE was higher at all ages in those who reported wheeze at age 23 years compared with those who did not (34 vs 6 IU/mL (p=0.016) at age 1 year; 45 vs 43 IU/mL (p=0.48) at age 7 years; and 72.5 vs 41.9 IU/mL (p=0.18) at age 23 years). There were no significant associations between randomisation and skin prick tests to specific allergens at any age.
Discussion
The MAPS study sought to determine whether avoidance of cow’s milk before birth and for the first 16 weeks of life decreased the risk of subsequent allergic disease. To facilitate cow’s milk avoidance in mothers who chose not to breast feed, soya milk was provided to those randomised to cow’s milk avoidance. Although breast feeding was associated with a decreased risk of wheezing at 1 year of age, it had no significant longer-term effects. Unexpectedly the rates of atopy and asthma were significantly higher at age 23 years in those randomised to cow’s milk avoidance. The prospectively collected food diaries suggest that earlier exposure to cow’s milk was associated with a decreased risk of wheeze and asthma at age 23 years, while earlier exposure to soya was associated with increased risk of atopy and asthma.
MAPS was undertaken in a deprived community—18% of the fathers were unemployed and in only 24.9% of families was the father a non-manual worker15—so it is unsurprising that the frequency of breast feeding was low.20 Our findings that only 37.4% of infants were breast fed at 1 week contrasts with more recent studies reporting 89% of infants were breast fed for at least a month.21 Observational studies of the effect of breast feeding on the development of allergic diseases offer conflicting results.6 These may reflect differences in the definition of breast feeding (exclusive, predominant, any), the study population (low or high risk) and whether details of breast feeding are recorded prospectively or retrospectively. Furthermore, there is the potential for reverse causality as parents of babies at high risk of allergic disease may breast feed their babies for longer.22 Most studies of breast feeding report a decreased risk of eczema and viral associated wheezing early in childhood,9 21 but a possible increased risk of asthma in late childhood.23 The only randomised trial of breastfeeding promotion compared with usual care suggested that breast feeding decreases the risk of eczema in adolescence, but there was no effect on asthma.24 Although our finding that breast feeding decreased the risk of wheeze in early life accords with previous reports,21 25 the low rate of breast feeding in MAPS makes further interpretation difficult. Breastfeeding mothers in the intervention group were recommended to reduce cow’s milk intake to potentially decrease allergens in their breast milk, although it is now thought to have little effect.26
The pregnant women entering MAPS were given information on the study and gave signed consent, but the study predated the development of research ethics committees in the UK. Although conducted with the best intentions, it is unlikely the study would now receive a favourable opinion from a research ethics committee. Due to concerns over the long-term consequences of ingestion of phyto-oestogens in soya based formulae, their use below 12 months of age is not recommended.14 Furthermore the soya milk was supplied free to those in the intervention group if not breast feeding, while those in the control group had to buy their own milk. Unsurprisingly the frequency of breast feeding was lower in the intervention group, and it is now accepted that breast milk alternative trials should not provide free formula that might compromise the mother’s commitment to breast feed.27 Similarly MAPS predates the CONSORT statement28 on the reporting of randomised controlled trials, and although the cohort was regularly reviewed, the reporting would not reach CONSORT standards.
In the design of MAPS it was assumed that soya milk was less antigenic than cow’s milk protein,12 and that soya might decrease the risk of allergic disease.13 It is now recognised that although allergy to soya milk may be less frequent than to cow’s milk, there is considerable overlap.29 A systematic review of soy formula for prevention of allergy and food intolerance in infants30 found no significant difference in the incidence of childhood asthma following prolonged use of soy formula compared with cow’s milk formula. It is possible that either a hydrolysed or extensively hydrolysed formula might have been a more suitable comparator.
It is unclear whether the increased risk in the intervention group is due to decreased exposure to cow’s milk early in life, or early exposure to soya milk. There is increasing evidence that earlier introduction of potentially allergenic foods may be beneficial. Observational studies suggest that delayed exposure to foodstuffs—cow’s milk,31 wheat,32 egg33 and peanut34—are associated with increased risks of subsequent allergy to the relevant foodstuff. Prospective clinical trials such as the Learning Early About Peanut (LEAP)35 or Enquiring About Tolerance (EAT)36 trials give stronger evidence. In LEAP, infants at high risk were randomised to either early (age 4–11 months) or delayed (avoidance until age 5 years) introduction of peanut. At 5 years of age the prevalence of peanut allergy was 13.7% in the avoidance group and 1.9% in the consumption group, with early peanut introduction being associated with significantly increased serum peanut IgG4 levels.35 In the EAT trial, exclusively breastfed infants were randomised at 3 months to either early (immediate) or standard (at age 6 months) introduction of six allergenic foods including cow’s milk. There was poor adherence with the early introduction of foods, but a per protocol analysis suggested that the prevalence of food allergy was 76% lower in the early introduction group, with the efficacy dependent on the quantity and duration of consumption of the specific food.36 In contrast, in a study where infants were randomised to breast feed with or without a small amount of cow’s milk for at least the first 3 days of life, atopic disease was common in both groups at age 2 years. However, of those who had atopic disease at age 2 years, asthma and wheeze was twice as frequent at age 6 years in those exposed early to cow’s milk.37 It may be that early exposure alone is insufficient and that both early and prolonged exposure is necessary to decrease the risk of allergy.38
In our study, cow’s milk IgG4 levels were significantly higher at 3 months in the control group compared with the intervention group, suggesting that early oral exposure to cow’s milk induces IgG4 class switching. In addition to the primary prevention of peanut allergy,35 raised IgG4 levels have also been associated with successful immunotherapy for cow’s milk protein allergy.39 The early introduction of cow’s milk is associated with a decreased risk of subsequent IgE-mediated cow’s milk allergy,31 while delayed introduction of cow’s milk is associated with an increased risk of atopy, particularly eczema, at 2 years of age.40 In infants with cow’s milk protein allergy, early exposure to cow’s milk is associated with subsequent decreased bronchial hyper responsiveness to histamine.41 A positive skin prick test to cow’s milk in the first year of life is predictive of asthma aged 22 years.42 Thus, early cow’s milk exposure is associated with increased cow’s milk IgG4 levels, decreases the risk of cow’s milk allergy, and could decrease bronchial hyper responsiveness and potentially asthma in adulthood.
In truth we cannot know whether it is cow’s milk avoidance early in life that decreases the risk of asthma, or whether it is soya milk exposure that increases the risk. Although there are differences in the risks of wheeze and atopy, the hazard ratios appear to be reciprocals of the same effect. On the balance of probabilities the evidence suggests that it is allergen avoidance rather than allergen exposure early in life that increases the subsequent risk of allergic disease, and thus we would speculate that the salient event is cow’s milk avoidance.
There are a number of limitations to our study. It was conducted in a high-risk group and thus our findings might not be applicable to a general population. It was an open label extension study, although those conducting clinical assessments were all blinded to randomisation, and at age 23 years many of the subjects were unaware that they had been in a controlled trial let alone what milk they received. MAPS was conducted in an economically deprived community, and this is reflected in both the low rate of breast feeding and the attrition rate—although 62% of subjects supplied data at age 23 years, only 21% attended for clinical assessment. Although the response rates of both groups at age 23 years are very similar, the low response rate overall nevertheless introduces the possibility of attritional bias and limits the power of the study. Most importantly, the effect of the intervention will have been weakened by crossover of infants between groups, with many infants in the intervention group exposed to cow’s milk at an early age, while some mothers in the control group used soya milk for feeding their infants. An understanding of the mechanisms underlying our findings is weakened by the limits of detection of assays for IgE and IgG4 available in the 1980s. Although we have presented results for many outcomes, the analysis was planned to provide the results for wheeze, atopy and asthma at age 23, and thus we have not adjusted our results for multiple testing.
Despite these caveats, infants randomised to cow’s milk exclusion had a significantly higher risk of asthma and atopy at age 23 years, and the findings remained consistent in a per protocol analysis. These findings are supported by the prospectively collected food diaries for the first 26 weeks of life, where earlier exposure to cow’s milk was associated with a decreased risk of wheeze and asthma. Although not statistically significant, the OR for wheeze in the intervention group is very similar to that for asthma and atopy, while the HR for earlier cow’s milk exposure for atopy is very similar to that for wheeze and asthma. It is noticeable that the rate of reported wheeze at age 23 years (32.8%) is almost double that of reported asthma (17.7%), suggesting underdiagnosis.
In summary, exclusion of cow’s milk protein with replacement with soya supplementation in infancy increased the risk of asthma and atopy in adulthood. Earlier exposure to cow’s milk was associated with decreased risk of wheeze and asthma in adulthood, while earlier exposure to soya was associated with increased risk of atopy and asthma. Diet in infancy affects allergic disease in adulthood.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Acknowledgments
We would like to recognise the late Dr Michael Burr who conceived and initiated the MAPS study and followed the families through to 23 years of age, but was unfortunately unable to follow through to publication of the findings.
References
Footnotes
Contributors SH conceived the study, recruited the subjects at age 23 years, analysed the findings and wrote the paper; KJ conceived the study and wrote the paper; FD conceived the study, analysed the findings and wrote the paper; IJD analysed the findings and wrote the paper.
Funding Welsh Office of Research and Development (now Health and Social Research Wales) WORD ReF05/1/186. The MAPS study received funding from the Welsh Scheme for the Development of Health and SocialCare Research and Wyeth Laboratories. The 23 year year follow upfollow-up was funded by the Welsh Office of Research and Development (subsequently Health and Social Care Research Wales). None of the funders had any role in any of study design; the collection, analysis, and interpretation of data; the writing of the report; and the decision to submit the paper for publication. The corresponding author (ID) confirms that he had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.