Article Text

Abstract
Background Switching inhalers to cheaper equivalent products is often advocated as a necessary cost saving measure, yet the impact on patient’s health and healthcare utilisation has not been measured.
Methods We identified asthma and chronic obstructive pulmonary disease (COPD) patients from UK primary care electronic healthcare records between 2000 and 2016. A self-controlled case series was used to estimate incidence rate ratios (IRR); comparing outcome rates during the risk period, 3 months after the exposure (financially motivated switch), and control periods (preswitch and postrisk period). Four outcomes were assessed: disease exacerbation, general practitioner consultation, non-specific respiratory events and adverse-medication events. Medication possession ratio (MPR) was calculated to assess adherence. 2017 National Health Service indicative prices were used to estimate cost differences per equivalent dose.
Results We identified a cohort of 569 901 asthma and 171 231 COPD regular inhaler users, 2% and 6% had been switched, respectively. Inhaler switches between a brand-to-generic inhaler, and all other switches (brand-to-brand, generic-to-generic, generic-to-brand), were associated with reduced exacerbations (brand-to-generic: IRR=0.75, 95% CI 0.64 to 0.88; all other: IRR=0.79, 95% CI 0.71 to 0.88). Gender, age, therapeutic class, inhaler device and inhaler-technique checks did not significantly modify this association (p<0.05). The rate of consultations, respiratory-events and adverse-medication events did not change significantly (consultations: IRR=1.00, 95% CI 0.99 to 1.01; respiratory-events: IRR=0.96, 95% CI 0.95 to 0.97; adverse-medication-events: IRR=1.05, 95% CI 0.96 to 1.15). Adherence significantly increased post-switch (median MPR: pre-switch=54%, post-switch=62%; p<0.001). Switching patients, in the cohort of regular inhaler users, to the cheapest equivalent inhaler, could have saved around £6 million annually.
Conclusion Switching to an equivalent inhaler in patients with asthma or COPD appeared safe and did not negatively affect patient’s health or healthcare utilisation.
- inhaler devices
- asthma
- COPD epidemiology
Statistics from Altmetric.com
Key messages
What is the key question?
Physicians and patients alike are often reticent to switch to an equivalent inhaler to reduce National Health Service (NHS) costs, but it is a commonly encouraged local policy in the UK due to increasing NHS financial pressures; what is the impact of such a policy on patients’ health (exacerbations and symptoms) and healthcare utilisation (general practitioner (GP) consultations)?
What is the bottom line?
The findings from this real-world study support the cost-saving clinical practice of switching to cheaper equivalent inhalers.
Why read on?
This study assessed four different health outcomes (exacerbations, GP consultations, non-specific respiratory events and adverse-medication events), and multiple factors (eg, inhaler device, inhaler-technique checks) that could influence the impact of this clinical practice.
Introduction
In the UK, over 5.4 million people receive asthma treatment (estimated in 2012), and over 1.2 million people have a chronic obstructive pulmonary disease (COPD) diagnosis.1 2 Inhalers incur a large healthcare cost; due to the prevalence of asthma, three of the top five most expensive drugs in the National Health Service (NHS) budget are inhalers. Over £1.1 billion of the NHS budget is spent directly on asthma, the majority of which is due to medication; an additional £800 million is spent directly on COPD.
Pharmaceutical companies have made huge investments in the development of new inhaled medications, resulting in the availability of over 200 different products; expiration of many patents have led to the growth of generic products. Nonetheless, markets become dominated by only a few inhalers, even when cheaper equivalent products are available. Randomised controlled trials have demonstrated that switching inhalers between specified equivalent products results in comparable effectiveness.3 4 However, trials have optimised participant’s inhaler technique and encouraged high levels of adherence, which does not reflect everyday clinical practice and most respiratory patients do not meet typical trial eligibility criteria.5 6 There is a paucity of real-world studies assessing health outcomes after switching patients to an equivalent inhaler, furthermore, no study has specifically addressed switching for financial gain.7–11
In many European countries regulations allow switching of inhalers to cheaper bioequivalent products, generic or branded, including UK, Germany, Italy, Finland and Netherlands; other countries, including Spain, Belgium and Sweden, regulate against it due to the speculated negative impact on patient’s health and healthcare utilisation.12 In the UK, many local governments strongly advocate switching to cheaper equivalent inhalers, but the effect of this clinical practice on patient’s health and their healthcare use is unknown. Physician opinion appears often to be one of reticence, primarily due to apprehension of the interchangeability of inhalers, although the evidence to support this concern is marginal.13–18 This study aimed to describe the prevalence and health impact of financially motivated inhaler switching, for non-clinical motivation, in the UK and the subsequent health impact.
Methods
Data source
We used the Clinical Practice Research Database (CPRD), a nationally representative database of de-identified electronic healthcare records. CPRD holds data on diagnoses, symptoms, and prescriptions on more than 11 million patients across the UK.19 Globally, it is one of the largest longitudinal healthcare databases, and has been extensively validated.19 Secondary care and mortality information was obtained from the Hospital Episode Statistics (HES) database and Office of National Statistics (ONS), respectively. HES contains information on all admissions to English NHS hospitals. Approximately 60% of practices in CPRD have individual level linkage to HES and ONS, and to socioeconomic data (Index of Multiple Deprivation).
Study design
We conducted a self-controlled case series (SCCS) analyses (figure 1). SSCS is an increasingly popular study design,20–22 it allows each individual to act as their own control (comparing outcome rates during periods of exposure to periods of non-exposure) to therefore implicitly control for confounding factors that do not vary with time. This approach significantly reduces the bias that can occur in observational studies; for example, a cohort or case-control could suffer from confounding by indication which would be an issue with this research question. SCCS is also statistically more efficient than traditional cohort and case-control designs. The SCCS method is the most suitable when there are acute outcomes (eg, exacerbation) and transient exposures (eg, inhaler switch), and that exact timings of these are available.23 Incidence rate ratios (IRR) are calculated, comparing the rate of events during exposed periods (defined as the ‘risk period’) with that during all other observed periods (defined as the ‘control period’). To ensure valid and unbiased estimates, certain assumptions should be met.24 First, the outcome should not affect the occurrence of a further outcome event. As exacerbations are not independent, we studied only the first exacerbation outcome24; therefore, all patients had to have a 12-month exacerbation-free period before entering the SCCS-exacerbation cohort (prior to the control period). The other outcomes were considered to be independent. A second assumption is that the outcome does not affect the probability of exposure. This potential bias is common and simply reduced by using a pre-exposure period that is then not included in the analysis.24 Third, the outcome should not increase the probability of death; the typical approach to deal with this is to carry out a sensitivity analysis excluding patients that died.24
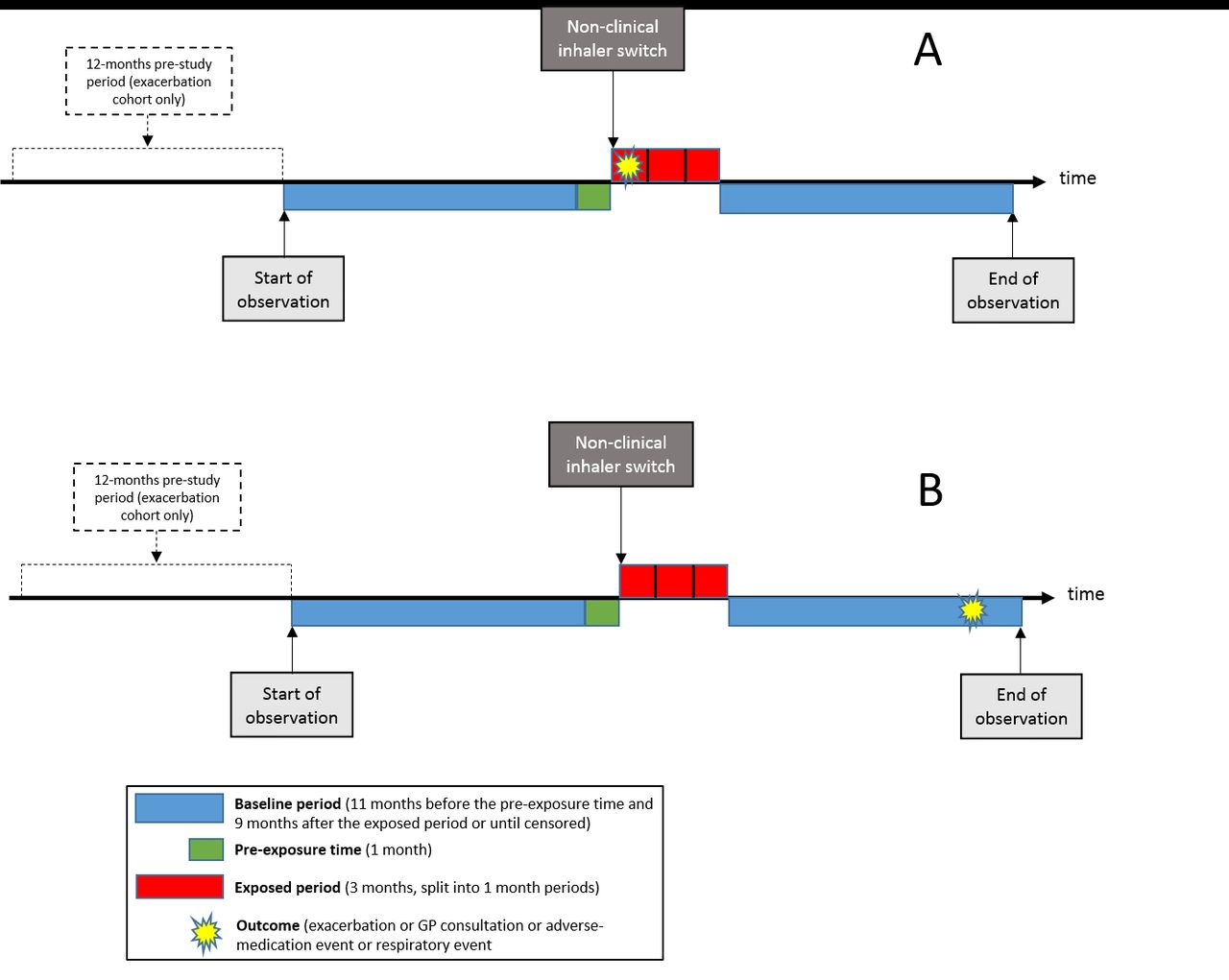
Pictogram (A) represents a patient that exacerbated during the 3-month risk period after their inhaler switch. Pictogram (B) represents a patient that exacerbated during the control period. The study assessed the relative incidence of the outcome during the risk period as compared with the control period.
Study population
Patients were identified as having asthma or COPD using validated algorithms.25 26
Study population: regular inhaler users
Only patients that were on a regular maintenance inhaler were included; this was defined as ≥3 consecutive prescriptions of the same inhaler class, each within 3 months of the next one. Maintenance inhaler classes were inhaled corticosteroid (ICS), long-acting beta agonist (LABA), combination LABA-ICS, long-acting muscarinic antagonist (LAMA), or combination LAMA-LABA. Prescription data were included from the latest date of the following: 1 January 2000, patient’s data were research acceptable (CPRD quality control), patient started a continuous CPRD record, 18th birthday (asthma) or 35th birthday (COPD), or first validated asthma/COPD read code. Follow-up was censored at the earliest date of the following: patient transferred out of CPRD, death, last data collection date, or 31 December 2016.
Main exposure and the four outcomes
Financially motivated inhaler switch (main exposure)
An inhaler switch was defined as at least three consecutive prescriptions of the same inhaler, followed by a subsequent prescription of a different inhaler, in the same therapeutic class, each within 3 months of the previous. For the switch to be defined as financially motivated it must be (1) between the same bioequivalent dosage, (2) occurred on a day without a respiratory symptom or adverse-medication symptom/event and (3) not on the day of another new inhaler. Switches were further broken down into those between brand-to-generic inhaler (financial motivation was the only objective), all other switches (financial motivation was highly likely). Three months use was arbitrarily defined as the time point by which the switch itself would have impacted on the patient’s health as it expected the effect of the ‘switch’ would be reasonably immediate. This was also further broken down by 1-monthly periods to look for any dose affect over time.
Outcomes
The main outcome of interest was exacerbations. COPD exacerbations were identified using a validated algorithm for CPRD data.27 28 Asthma exacerbations were identified as previously defined,29 a short course of oral corticosteroids, a hospital admission for asthma or death secondary to asthma. The other three outcomes were primary care consultations, non-specific respiratory events (including respiratory symptoms, inhaler technique, and other asthma and COPD specific events; online supplementary table 1), and adverse-medication events (online supplementary table 2).
Supplemental material
Populations used in the SCCS-cohorts
The SCCS analysis requires that each included patient should have the outcome (at some point during either the risk or control period), and the exposure—as those without both would not contribute towards the rate ratio estimate (patient exposed but without an outcome would have a rate of zero in all time periods); therefore, four different cohorts were identified for the four different outcomes described above (figure 2). The SCCS cohorts were: (1) exacerbations, (2) general practitioner (GP) consultations, (3) non-specific respiratory events and (4) adverse-medication events. Study follow-up was a maximum of 2 years. All patients entered the SCCS analysis 12 months before the non-clinical inhaler switch, and were censored at the earliest date of: 12 months after the inhaler switch, death, transferred out of CPRD, or last data collection. The exacerbation SCCS-cohort only comprised of patients with linked HES/ONS data (to ensure inclusion of hospital treated exacerbations).

{kind=link}
{kind=link}
Consort diagram of study inclusion and exclusion.
Measuring adherence
Adherence was calculated using the medication possession ratio (MPR); the sum of the days medication was prescribed, divided by the total number of days between the first and the last prescription plus the duration of the last prescription; this number is then expressed as a percentage. MPR was compared between preswitch (12 months before the switch) and postswitch (from the switch until follow-up ended).
Statistical and sensitivity analyses
Event rates were compared during the risk period (for 3 months after exposure) and the control periods (11 months before the pre-exposure 1-month period, and from the end of the risk period until censored) (figure 1). IRRs were also measured for each consecutive 1-month period during the 3-month risk period. The exacerbation analysis was stratified by the type of inhaler that was switched between; switches from a branded to a generic inhaler were analysed separately, as these should only be carried out for financial gain. Other scenarios (switches between: generic to branded, branded to branded, or generic to generic) were analysed separately as it is possible some of these switches may have been carried out for an undocumented clinical reason. IRRs were estimated using fixed effects conditional Poisson regression models. The effect was adjusted for age using age bands (years: 18–45, 45–55, 55–65, 65–75, 75–85, 85–110). Evidence of interaction was assessed using likelihood ratio tests for several time-invariant variables: respiratory condition, gender, therapeutic class, generic/brand switch, device switch, kept/not kept on same inhaler. The effects were reported by stratifying the analysis for each variable. A negative control analysis was also carried out, such that the ‘exposure’ date was a random consecutive inhaler prescription; patients also had to fulfil all eligibility criteria of the SCCS cohort. Stata V.14.0 was used for all analysis.
Cost analysis of switching inhalers
Inhaler prices were obtained using 2017 NHS indicative prices from the NHS Dictionary of Medicines and Devices (dm +d). All costs were calculated per bioequivalent medication dose. Assumptions about how many inhalers could be switched to generic inhalers used NHS product availability in 2017. Cost differences were based on the inhaler cost only.
Ethical approval
Linked pseudonymised data were provided for this study by CPRD. Data are linked by NHS Digital, the statutory trusted third party for linking data, using identifiable data held only by NHS Digital. Select practices consent to this process at a practice level with individual patients having the right to opt-out.
Results
Temporal changes in UK generic and device prescriptions
There has been a fall in the proportion of generic prescriptions for all therapeutic classes in asthma and COPD; most notable in ICS prescriptions (online supplementary figure 1). The proportion of dry powder inhaler (DPI) used in asthma dropped from 50% in 2000 to 30% in 2016, but remained around 50% in COPD (online supplementary figure 2).
Low prevalence of inhaler switching
Over the last decade the proportion of patient’s that had their inhalers switched within the same therapeutic class was low, although it slightly increased over time (2006–2016: asthma N=5 69 901, 2%–6% switched; COPD N=1 71 321, 3%–10% switched) (online supplementary figure 3). Around two-thirds of switches were for non-clinical reasons, the majority were between branded and generic products, and around one-third were for increases in medication dose or adverse-medication effects. Inhaler switching peaks were in 2001 (Becotide, a phased-out ICS), 2007/2008 (chlorofluorocarbons, phased out MDIs), and 2014 onwards (LAMA and combination LABA-ICS inhalers).
SCCS-cohorts were similar to the regular inhaler users
Of those with a non-clinical inhaler switch, 5242 patients met eligibility criteria for the exacerbation SCCS-cohort, 50 289 for the consultations SCCS-cohort, 51 659 for the respiratory events SCCS-cohort and 3258 for the adverse-medication events SCCS-cohort (figure 2). The four SCCS-cohorts were broadly similar in characteristics to the populations they were derived from table 1). The SCCS-cohorts were also similar to the much larger population of regular inhaler users (online supplementary table 3). The SCCS-cohorts were equivalent in terms of inhalers prescribed, frequency of inhaler technique checks (around 40%) and proportion that had experienced adverse-medication events (around 2%) (table 1); except for the adverse-medication events SCCS-cohort, as would be expected.
Description of the demographics and characteristics of each of the SCCS cohorts, and the study population of patients that they were drawn from
Most non-clinical inhaler switches occurred with ICS and LABA-ICS. Around 90% were between an identical drug (table 1), approximately three-quarters were between the same device type, and around 80% were between generic and brand. Around 95% of patients kept the inhaler that they were switched to.
Health impact of non-clinical inhaler switching
The IRR of an exacerbation was significantly lower after switching (brand-to-generic: crude IRR=0.74, 95% CI 0.63 to 0.87, age-adjusted IRR=0.75, 95% CI 0.64 to 0.88; all other switches: crude IRR=0.78, 95% CI 0.70 to 0.87, age-adjusted=0.79, 95% CI 0.71 to 0.88). Differences in patient characteristics, or differences in measured factors related to the inhalers, did not significantly modify the rate of exacerbations; these characteristics were differences in patient condition (COPD/asthma), gender, therapeutic class (ICS, LABA-ICS, LABA, LAMA), device switch (MDI/DPI) and inhaler technique check (LRT p>0.05, tables 2 and 3). Exacerbation rates were not significantly different each consecutive month of the 3 months after the inhaler switch (p<0.05, online supplementary tables 4 and 5). A sensitivity analysis excluding patients who died (N=80) showed negligible difference in the IRRs.
Age-adjusted incidence rate ratios (IRR) of exacerbations, in the 3-month risk period after a brand-to-generic inhaler switch, compared with stable periods
Age-adjusted incidence rate ratios (IRR) of exacerbations, in the risk period compared with stable periods, after an inhaler switch (brand-to-brand, generic-to-generic or generic-to-brand)
There was no significant association between the rate of consultations and switching (age-adjusted IRR=1.00, 95% CI 0.99 to 1.01; table 4). There was a very slight reduction in respiratory events (age-adjusted IRR=0.96, 95% CI 0.94 to 0.97). There was a non-significant minor increase in the risk of adverse events (age-adjusted IRR=1.05, 95% CI 0.96 to 1.15); the risk decreased with each consecutive month, during the 3-month risk period (online supplementary table 6).
The incidence rate ratios (IRR) of general practitioner (GP) consultations, respiratory events, and adverse-medication events, in the risk period after an inhaler switch compared with stable periods
The negative control analyses found no effect on exacerbations (age-adjusted IRR=0.99, 95% CI 0.96 to 1.02).
Impact of switching on adherence
Inhaler adherence improved after the inhaler switch. The median MPR (IQR) for the 12 months preinhaler switch was 54.8% (39.1–78.2), compared with 62.6% postinhaler switch (47.0–93.9) (p<0.001). Postinhaler switch adherence was not different between patients that were switched on the day of a GP consultation or not (median MPR=62.6%, p>0.05).
Potential cost saving of switching to cheaper inhalers
In the exacerbation SCCS cohort, 1184 of the 5242 switches (23%) could have been switched to a cheaper equivalent generic product in 2017. This could have saved an estimated £14 308, or annual saving of around £172 000 (assuming an inhaler prescribed per month) (online supplementary table 7). In the same cohort, 2125 of the 5242 switches (41%) could have been switched to a cheaper bioequivalent branded product (same therapeutic class and bioequivalent dose, although drug may differ). This could have saved £28 231, or annual saving of around £339 000 (online supplementary table 8).
Supplemental material
In the total cohort of 665 105 regular inhaler users, there was an alternative cheaper equivalent generic inhaler available for 28% of prescriptions (LABA-ICS or LAMA) in 2016; switching to these could have saved approximately £1.97 million. An estimated additional £4.1 million could have been saved if all inhalers had been switched to the cheapest bioequivalent product (including generic or branded products), assuming all patients were suitable for switching to the alternative.
CPRD represents at least 5% of the UK population, extrapolating our findings indicates that, if implemented across the UK, switching to the cheapest available bioequivalent product (generic or branded), could have saved the NHS approximately £112 million (1.5% of the total primary care annual prescribing costs).
Discussion
Principal findings
From this study of over 0.65 million asthma patients and just under 0.2 million COPD patients, it was observed that inhaler switching for financial-motivation was uncommon; in keeping with the only other nationally representative study of inhaler switching.7 The increase in switches from generic to branded inhalers is likely due to the increase in the availability of cheaper branded inhalers in the UK; the cheapest LABA-ICS in 2017 was a branded inhaler. We found that switching slightly reduced the risk of an exacerbation. This risk was not significantly affected by the patient’s age, gender, type of respiratory disease, whether the switch was between MDI/DPI devices or not, whether the patient had a documented inhaler check that year, or the medication class that was switched. Around 95% of the patients remained on their switched inhaler. Interestingly, adherence to the switched inhaler was significantly higher than adherence to the pre-switch equivalent inhaler. This may partially explain the observed reduction in exacerbations as, although the study was not designed to measure adherence as a primary outcome, the increase was only slightly below the considered clinically minimal important difference of 10%.30 Further analyses, of over 50 000 patients, showed that non-clinical inhaler switching did not affect the rate of GP consultations, but slightly decreased the rate of non-specific respiratory events (including symptoms) and slightly increased the rate of adverse medication events, however, these effects were not statistically significant. Overall this clinical practice appears to occur infrequently in the UK. The cost analyses estimated significant savings could potentially be gained from switching expensive popular inhalers to bioequivalent cheaper (generic or branded) ones.
A less commonly advocated, but arguably as important, reason to switch an inhaler, is to reduce the large environmental impact that MDI inhalers produce.31 Hydrofluorocarbon inhalers are estimated to contribute 4% of the NHS’s entire carbon footprint, with MDIs identified as a ‘carbon hotspot’ in the NHS.32 Switching from a MDI to a DPI is thought to decrease the carbon footprint by a factor of 18.31 Discerningly, our observations suggest only around a third of inhalers prescribed for asthma patients, and half of those prescribed for COPD patients, are DPIs; yet switching between MDIs and DPIs did not seemingly impact on exacerbations, adverse medication events or respiratory events.
Comparison to previous studies
There have been few real-world studies addressing switching inhaler therapy of equivalent medication and dose. A small UK asthma study, 1993–2003, looked at ICS switching of 824 patients, at GP practice-level, not individual-level; they found no change in exacerbations.11 Another UK study, considered 979 asthma patients, switching from any ICS to a particular inhaler, the reason was not reported and may have often been clinical; they found no worsening of clinical outcomes.8 A more recent observational UK study addressed switching of 382 asthma patients from one commonly used LABA-ICS inhaler to the cheapest one.10 Although the product drugs differed, the study found a decline in exacerbations, improvement in asthma control, and reduction in healthcare costs; however, the reason for the switches was not described, and due to the design there may have been confounding by indication. One large Dutch study, including 70 053 patients, investigated adherence to inhaler medication after switching to generic products; this study found an increase in adherence in patients switched between a branded to a generic inhaler.7 Our findings in respect to adherence levels are also in keeping with previous studies.7 33 Evidence is even sparser for COPD patients,15 with only a small retrospective Japanese observational study of 57 patients that had switched between specific LAMA inhalers.9 None of these studies comprehensively addressed the overall impact of non-clinical inhaler switching, nor directly examined the impact of switching from a branded to a generic inhaler.
Strengths and weaknesses of the study
One advantage was the use of real-world data; whereas in most trials, inhaler technique is optimised, and adherence is encouraged. The SCCS cohorts were similar to the large nationally representative population that they were drawn from. Therefore, these two features provide results likely to be generalisable to the UK, and other similar populations. However, it is also probable that most patients were only switched if deemed appropriate by their GP practice, therefore, these results would only be generalisable to such patients. Switching may also have led to improved adherence and/or inhaler technique if the GP practice or patient’s pharmacist provided education at the time of the switch.
Another advantage was that the SCCS design is less prone to confounding and statistically more efficient than traditional cohort designs. To prevent violation of the SCCS assumptions, in the exacerbation cohort alone, an eligibility criterion of a 12-month period of no exacerbations prior to the observation period was set. This could have reduced generalisability (as a patient must have 1-year exacerbation-free period), but, the SCCS-exacerbation cohort was very similar to the reference population and analyses with the three other outcomes, which did not have this eligibility stipulation, showed comparable findings. It’s also possible that the effect of inhaler switching had a shorter or more prolonged affect than 3 months, however, this would only have underestimated the relative risk. Although the prescription data quality was high, we did not know if the prescription was dispensed or taken. However, a very low proportion did not stay on the switched prescription (suggesting the medication was dispensed). The respiratory and adverse-medication events measured were only those that were recorded, potentially some were not. If such under recording was equally likely throughout follow-up, this would only lead to reduced power, rather than generating a biassed estimate. Mild exacerbations were not included as an outcome as identifying these from the data would not have been accurate. However, the assessment of symptom changes, should have identified milder clinical effects. The potential cost savings, depended on the assumption that all patients were suitable; but, we recognise this is unlikely as not all inhaler devices suit everyone. The cost analysis did not take into account savings from reductions in exacerbations. Since 2016 it is possible switching prevalence has changed, although this would not affect the effect estimates from switching.
Implications of these findings
Treatment with combination inhalers is increasing; as these are some of the most expensive products, this will continue the escalation in respiratory spending. Our findings suggest that financially driven inhaler switching occurs infrequently. This is likely due to physician reticence, related to concern that switching is detrimental to a patient’s health. This apprehension has been discussed in several reviews, and questionnaires found that doctors across Europe believe that inhalers are not interchangeable.12–18 34–36 Reassuringly, we have shown here, that exacerbations, respiratory symptoms, and adverse-medication events did not increase; in fact, only 5% of patients did not stay on their new inhaler. We propose that the temporary decrease in exacerbations could be related to a temporary increase in inhaler adherence, due to intensified medication awareness or related to adherence discussion at the time of the inhaler switch. There may have been, predictable or unpredictable, reasons why inhaler switching was successful in these patients, but the parameters we were able to consider did not reveal any influencing characteristics. Further studies are therefore needed to determine the factors that will ensure a successful outcome, and which patients and circumstances are not suitable.
These findings have important implications and could help inform national policy; they suggest that switching inhalers is safe, if implemented correctly (which should include appropriate patient selection and mandating the importance of providing inhaler education), and could help to redirect the respiratory healthcare budget towards more effective use.
References
Footnotes
Contributors All authors provided substantial contributions to the work. CIB, ID, LS and JKQ devised the study. CIB analysed, interpreted the data and produced draft manuscripts. ID, JO and GA provided specific input for the analysis and interpretation. All authors reviewed and edited the manuscript. All were happy with the final version and approved it for submission for publication.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests CIB reports grants from MRC, AsthmaUK, Chiesi and AstraZeneca outside the submitted work. ID reports grants from GSK and the British Pharmaceutical Industry outside the submitted work. JO has nothing to disclose. GA reports personal fees from AstraZeneca, BI, Chiesi, GSK,Pfizer, Napp, Novartis and Teva outside the submitted work. LS reports grants from Wellcome, MRC, NIHR, GKS, BHF and Diabetes UK outside the submitted work; reports personal fees and is a Trustee of the British Heart Foundation. JKQ reports grants from The Health Foundation, MRC, British Lung Foundation, GSK, grants and personal fees from BI, grants and personal fees from AstraZeneca, Chiesi, GSK, BI, AZ, Teva, Bayer, IQVIA and Insmed; personal fees from Chiesi, GSK, BI, AZ, Teva, Bayer and Insmed.
Patient consent for publication Not required.
Ethics approval The protocol for this research was approved by the Independent Scientific Advisory Committee (ISAC) for MHRA Database Research (protocol number 17_090RAR) and the approved protocol was made available to the journal and reviewers during peer review. Generic ethical approval for observational research using CPRD with approval from ISAC has been granted by a Health Research Authority (HRA) Research Ethics Committee (East Midlands—Derby, REC reference number 05/MRE04/87).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data may be obtained from a third party and are not publicly available.