Article Text

Abstract
Background Conventional measures to evaluate COPD may fail to capture systemic problems, particularly musculoskeletal weakness and cardiovascular disease. Identifying these manifestations and assessing their association with clinical outcomes (ie, mortality, exacerbation and COPD hospital admission) is of increasing clinical importance.
Objective To assess associations between 6 min walk distance (6MWD), heart rate, fibrinogen, C reactive protein (CRP), white cell count (WCC), interleukins 6 and 8 (IL-6 and IL-8), tumour necrosis factor-alpha, quadriceps maximum voluntary contraction, sniff nasal inspiratory pressure, short physical performance battery, pulse wave velocity, carotid intima-media thickness and augmentation index and clinical outcomes in patients with stable COPD.
Methods We systematically searched electronic databases (August 2018) and identified 61 studies, which were synthesised, including meta-analyses to estimate pooled HRs, following Meta-analysis of Observational Studies in Epidemiology (MOOSE) and Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.
Results Shorter 6MWD and elevated heart rate, fibrinogen, CRP and WCC were associated with higher risk of mortality. Pooled HRs were 0.80 (95% CI 0.73 to 0.89) per 50 m longer 6MWD, 1.10 (95% CI 1.02 to 1.18) per 10 bpm higher heart rate, 3.13 (95% CI 2.14 to 4.57) per twofold increase in fibrinogen, 1.17 (95% CI 1.06 to 1.28) per twofold increase in CRP and 2.07 (95% CI 1.29 to 3.31) per twofold increase in WCC. Shorter 6MWD and elevated fibrinogen and CRP were associated with exacerbation, and shorter 6MWD, higher heart rate, CRP and IL-6 were associated with hospitalisation. Few studies examined associations with musculoskeletal measures.
Conclusion Findings suggest 6MWD, heart rate, CRP, fibrinogen and WCC are associated with clinical outcomes in patients with stable COPD. Use of musculoskeletal measures to assess outcomes in patients with COPD requires further investigation.
Trial registration number CRD42016052075.
- copd epidemiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is the key question?
What is the existing knowledge on the association between selected cardiovascular and musculoskeletal biomarkers and the occurrence of clinical outcomes within a COPD population?
What is the bottom line?
There is a need to further examine the association between musculoskeletal biomarkers and clinical outcomes in COPD.
Why read on?
This study systematically summarises and examines the association between multiple clinical outcomes (ie, mortality, exacerbation and COPD hospital admission) and multiple biomarkers including 6 min walk distance, resting heart rate, fibrinogen, C reactive protein, white cell count, interleukins 6 and 8, tumour necrosis factor-alpha, quadriceps maximum voluntary contraction, sniff nasal inspiratory pressure, short physical performance battery, pulse wave velocity, carotid intima-media thickness and augmentation index.
Introduction
COPD is one of the leading causes of death worldwide, with the prevalence of 5.6% (3.2 million) in 2015 projected to increase to 7.8% by 2030.1 The consequent socioeconomic burden of COPD is high, causing reduced quality of life (QOL), loss of productivity, increased hospital admissions and premature mortality. One important and cost-effective intervention is smoking cessation.2 3 However, increasing importance is placed on improving risk factors and slowing down disease progression by addressing non-pulmonary aspects of the condition.4–8
Spirometry is the most widely used marker of disease severity and progression. No longer is it believed that all patients will worsen over time with increasing airflow limitation. Clinicians have now identified that COPD is heterogeneous and existing measures such as FEV1 may fail to capture systemic disease9 and have divergent trajectories.10
COPD also leads to systemic problems, such as skeletal muscle weakness and cardiovascular disease, the latter accounting for a third of deaths in COPD.11 While multiple studies have shown that quadriceps involvement in COPD is associated with worse outcomes,12–14 it has also been postulated that these features result from an increase in inflammatory markers like C reactive protein (CRP) and fibrinogen,15 with a spillover effect of inflammatory response proposed as the underling mechanism.16 Thus, capturing systemic manifestations such as exercise intolerance, cardiovascular abnormalities, skeletal muscle weakness and plasma biomarkers are recognised to be of increasing clinical importance.17
We aim to systematically synthesise the published evidence on the associations between selected cardiovascular and musculoskeletal biomarkers that are not yet widely used in clinical practice but may potentially better capture systemic problems in COPD than conventional measures, and the occurrence of clinical outcomes including exacerbations, hospitalisation and mortality within a COPD population. Individual studies and a limited number of reviews18–20 have assessed the association between selected biomarkers and clinical outcomes; however, to our knowledge, no published study has systematically synthesised this evidence.
Methods
Search strategy
The systematic review includes electronic searches in the Ovid versions of MEDLINE, Embase, Cochrane Library, CINAHL and Web of Science. Search terms related to pulmonary disease were combined with terms related to cardiovascular and musculoskeletal measure, clinical outcome and study design (online supplementary table S1). A meta-analysis was carried out following MOOSE guidelines and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines to identify prospective studies assessing the relationship between cardiovascular or musculoskeletal measures and the occurrence of clinical outcomes in COPD.21 22
Supplementary file 2
Biomarkers and outcomes
Biomarkers that may capture systemic problems in COPD and are not yet widely used in clinical practice were included: 6 min walk distance (6MWD), resting heart rate, quadriceps maximum voluntary contraction (QMVC), sniff nasal inspiratory pressure (SNIP), short physical performance battery (SPPB), pulse wave velocity (PWV), carotid intima-media thickness (CIMT) and augmentation index (AIx). Data relevant to inflammation were fibrinogen, CRP, white cell count (WCC), interleukin-6 (IL-6) and interleukin-8 (IL-8) and tumour necrosis factor-alpha (TNF-α). Clinical outcomes of interest included: mortality, exacerbation and hospitalisation. Mortality was defined as all-cause mortality. Exacerbation was defined as patients who either had a change in medication, which required increase or initiation of steroids or antibiotics, or were admitted to hospital due to COPD. Hospitalisation, a subset of COPD exacerbation by definition, was limited to only exacerbations that resulted in admissions related to COPD.
Two reviewers independently completed the selection and review of articles. Full-text papers and reviews found in the initial search were cross-referenced. Studies that satisfied the full-text paper selection criteria included: (1) primary research; (2) had a sample size ≥50 with COPD; (3) assessing a relevant biomarker; (4) full-text paper in English; (5) a general population (eg, not a single gender); (6) did not include unstable COPD patients (eg, currently in acute exacerbation, currently hospitalised or recruited on discharge); and (7) were prospective studies with a follow-up period ≥6 months.
Data extraction and quality assessment
Where possible, adjusted (ie, age, sex, BMI and smoking status) and unadjusted HRs for mortality were collected, as well as model performance measures (eg, C-statistic). Sample sizes, mean values and SD of the biomarkers for individuals with and without the event (ie, mortality, exacerbation or hospitalisation) were extracted from published studies to estimate standardised mean differences (SMDs). Where data were not published, the corresponding authors were contacted and asked to provide data by completing a data collection form (online supplementary material). Three reminders were sent over a period of 4 months. For studies reporting the same cohort, data from the study with the most completed outcome data, largest sample size or with the longest follow-up were used. The quality of each study was based on Quality Assessment of Diagnostic Accuracy Studies 2 (QUADAS-2) quality assessment criteria.23 Scoring was based on the follow-up period, sample size, reporting of adjustment factors, method of defining COPD, age of study participants and study type (online supplementary table S2). Scores range from 0 to 15, where 15 is considered of highest quality.
Supplementary file 1
Statistical analysis
To synthesise and analyse quantitative data, while accounting for heterogeneity by incorporating between study variability of effect sizes, results from the studies were assessed with random effects meta-analysis. Data were graphically displayed using forest plots. Where necessary and possible, HRs were converted to the selected unit effect measure. HRs for log-transformed biomarkers represent a twofold increase in the biomarker. To address uncertainty, we excluded studies with a quality score in the bottom QUADAS-2 score tertile (first: 15–12; second: 11–9; third: 8–0). Funnel plots were generated to assess potential publication bias. Galbraith plots were generated to assess heterogeneity in effect sizes.24 Results from a fixed-effects meta-analysis were compared against those from a random-effects meta-analysis. Finally, meta-regression was conducted, where possible, to analyse the impact of length of follow-up, year of publication and the mean age of the cohort. Trend analysis was performed using analysis of variance.
Results
The systematic review yielded 2852 unique references from five electronic databases. After screening the abstracts, 61 articles met the selection criteria (figure 1 and online supplementary table S3). The age of participants of the included studies ranged from 40 years to 80 years, with an approximate median age of 65 years. The sample sizes ranged from 53 to 20192 subjects, with a median size of 237. The follow-up period ranged between 6 months and 423 months, with an approximate median time of 36 months. The Evaluation of COPD Longitudinally to Identify Predictive Surrogate End-points (ECLIPSE) and Body mass index, airflow Obstruction, Dyspnea and Exercise (BODE) cohorts were the most studied cohorts.

Flow diagram of studies included in the review based on the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols.21 Records identified: MEDLINE: n=1175; Embase: n=1597; Cochrane: n=56; CINAHL: n=143; and Web of Science: n=765.
Included biomarkers
The most frequently reported biomarkers in the studies were: 6MWD (56%), CRP (39%), fibrinogen (28%), IL-6 (25%), IL-8 (16%), WCC (16%), TNF-α (11%) and resting heart rate (8%), with few assessing CIMT, PWV and AIx. With the exception of the 6MWD, very few musculoskeletal biomarkers (ie, QMVC, SNIP and SPPB) have been reported for their association with clinical outcomes within COPD. The majority of studies (n=34) included mortality as an outcome measure, followed by exacerbation (n=25) and hospitalisation (n=15). Of these, 11 studies investigated two outcomes, and only one investigated all three outcomes.
Data synthesis
All 61 studies are included in the qualitative review, with 32 studies included in the quantitative data synthesis (figures 2–4 and online supplementary table S1–3) and the sensitivity analyses (online supplementary table S6–11). Twenty (69%) studies reported data on mortality, nine (28%) reported data on COPD exacerbations and eight (25%) reported data on COPD hospitalisation (Data from Faganello et al 25 except for IL-8 were excluded as the same cohort but with a longer follow-up period was examined by Ferrari et al. 26 Data from Spruit et al 27 were also excluded as the ECLIPSE cohort was examined in a more recent publication by Müllerova et al. 28 Additionally, data from Agusti et al (ECLIPSE cohort)29 and Durheim et al (INSPIRE-II cohort)30 were not included as more data were made available through Celli et al 31 and Blumenthal et al,32 respectively. Results of the 6MWD reported by de Torres et al 33 (BODE cohort, n=218) were not included because these were covered by Cote et al using a larger study sample (n=365) and longer follow-up time34).

Pooled HRs for the risk of mortality with 95% CIs, by biomarker. Studies included: Ferrari et al,26 Celli et al,31 Blumenthal et al,32 de Torres et al,33 Cote et al,34 Dajczman et al,36 Waschki et al,37 Dreyse et al,40 Ozgür et al,42 Mannino et al,43 Jensen et al,46 Valvi et al,48 Liu et al, 49 Grolimund et al,51 Budweiser et al,54 Husebø et al,55 Antonelli-Incalzi et al,68 Cano et al,69 Lacasse et al 70 and Warnier et al.71 See online supplementary figure S1 for full study details. Bars, 95% CIs.
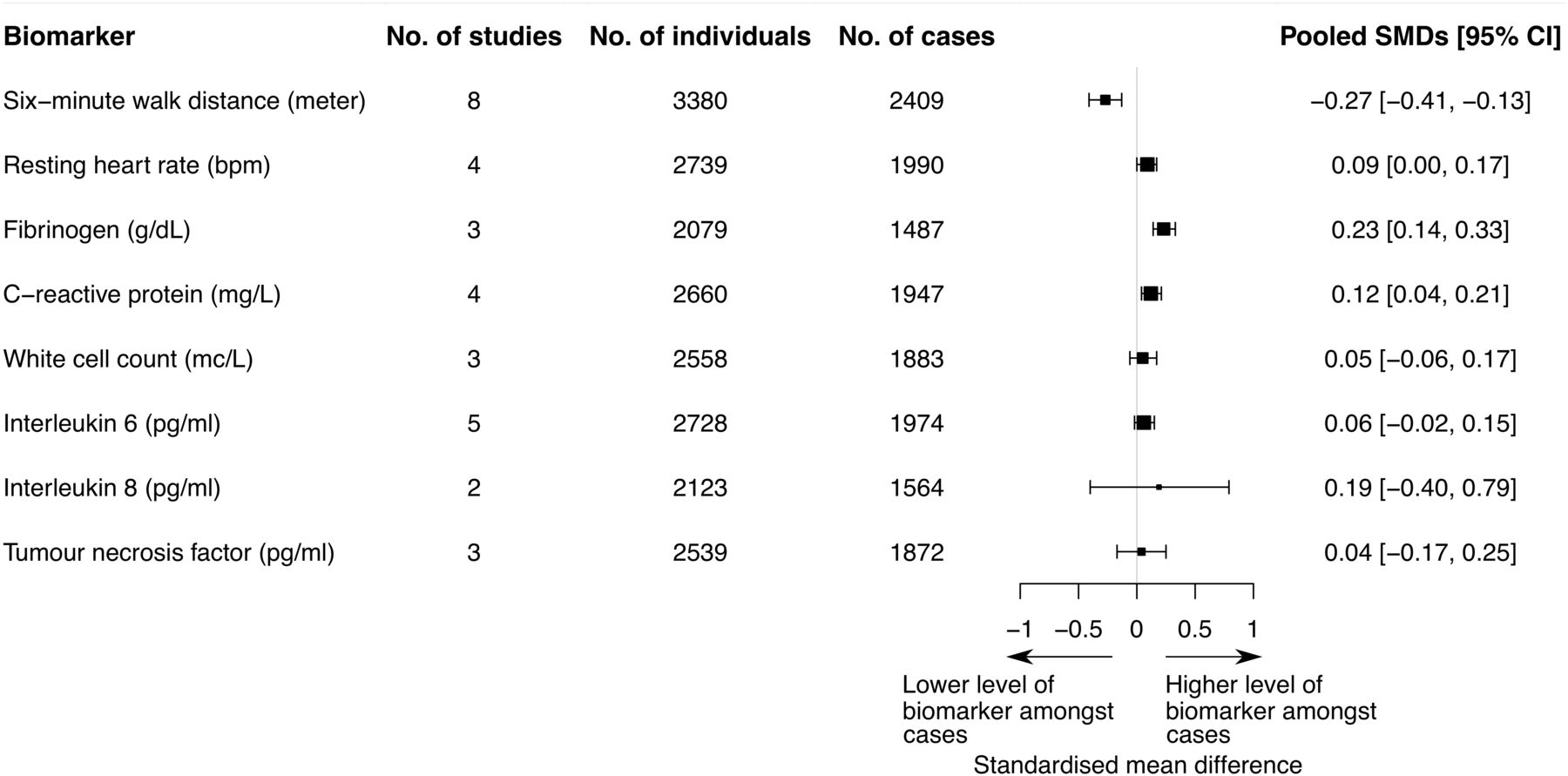
Pooled SMDs with 95% CIs for exacerbation by biomarker. Studies included: Faganello et al,25 Cote et al, 34 Dreyse et al,40 Ferrari et al,41 Monninkhof et al, 44 Hurst et al,53 Husebø et al,55 Wedzicha et al,56 Jennings et al 72 and Marino et al.73 See online supplementary figure S2 for full study details. Bars, 95% CIs. SMD, standardised mean differences.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Pooled SMDs with 95% CIs for hospitalisation by biomarker. Studies included: Ferrari et al,26 Müllerova et al,28 Dreyse et al,40 Monninkhof et al,44,Jensen et al,46 Groenewegen et al,52 Husebø et al,55 Cano et al,69 Jennings et al 72 and Dahl et al.74 See online supplementary figure S3 for full study details. Bars, 95% CIs. SMD, standardised mean differences.
Association between cardiovascular and musculoskeletal measures, and clinical outcomes
Six-minute walk distance
Multiple studies, including ECLIPSE (n=2138), BODE (n=1379) and Investigational Study of Psychological Intervention in Recipients of Lung Transplant (INSPIRE-II;n=326), reported that COPD patients with a shorter 6MWD at baseline have a higher number of clinical events over a follow-up period of at least 6 months. A 6MWD of less than 350 m was associated with higher risk of early mortality, according to Cote and colleagues,35 while only Dajczman et al found a significant difference in mortality with a cut-off point of 6MWD ≤150 m.36 The 6MWD-based model, authored by Cote et al, had a C-statistic of 0.75 similar to Waschki et al (C-statistic=0.77)37 and higher than Casanova et al (C-statistic=0.70),38 and Spruit et al (C-statistic=0.67) for a 6MWD threshold of 334 m.27 The remaining studies, with relatively small sample sizes, indicated no statistically significant difference in 6MWD between those with and without exacerbation.39–41 Meta-analysis indicated that longer walking distances at baseline were associated with early mortality (HR 0.80 per 50 m increase, 95% CI 0.73 to 0.89, p<0.01, I2 = 99.4 %), COPD exacerbation (SMD −0.27, 95% CI −0.41 to −0.13, p<0.01, I2 = 53.0 %) and hospitalisation (SMD −0.48, 95% CI −0.66 to −0.30, p<0.01, I2 = 61.3 %). Galbraith plots indicated that Ozgür et al,42 Mannino et al,43 Monninkhof et al 44 and Dreyse et al 40 were the least consistent with the overall results, potentially causing bias (online supplementary figure S5). Removal of these studies did not alter findings. After removing studies with a quality score in the bottom tertile (≤8), SMDs for exacerbation (SMD −0.27 to −0.15) and hospitalisation (SMD −0.48 to −0.35) had a substantial change, resulting from the removal of studies with small sample sizes and short follow-up times. Meta-regression indicated no differences in HRs for studies with longer follow-up time or those more recently published but suggests higher HRs for studies with older participants (p=0.03; online supplementary figure S12).
Resting heart rate
Jensen et al estimated that having a resting heart below 65 beats per minute (bpm) compared with above 85 bpm (C-statistic=0.59), was associated with increased survival of approximately 10 years in Global initiative for chronic Obstructive Lung Disease (GOLD)45 stage I, ~7 years for GOLD stage II and ~6 years in GOLD stages III–IV.46 Meta-analysis indicated that higher resting heart rates at baseline were associated with early mortality (HR 1.10 per 10 bpm, 95% CI 1.02 to 1.18, p=0.01, I2 = 99.4 %), exacerbation (SMD 0.09 bpm, 95% CI 0.00 to 0.17, p=0.05, I2 = 0.0 %) and hospitalisation (SMD bpm 0.21, 95% CI 0.15 to 0.28, p<0.01, I2 = 10.0 %). After removing studies with a quality score in the bottom tertile, HRs for mortality increased (1.10–1.15) and SMD (0.09–0.08) lost significance for exacerbation.
Fibrinogen
Within the Copenhagen City Heart Study and Copenhagen General Population Study (n=8020), Thomsen et al reported a higher risk of exacerbation with elevated fibrinogen levels, however, only in combination with elevated levels of CRP and WCC at baseline (C-statistic=0.73).47 Celli et al reported a similar C-statistic of 0.70 when including fibrinogen together with WCC, CRP and other inflammatory markers to their predictive model.31 Meta-analysis indicated that for mortality, there was a positive association with fibrinogen (HR 3.13 per twofold increase, 95% CI 2.14 to 4.57, p<0.01, I2 = 0.0 % and HR 1.24 per 100 g/dL, 95% CI 1.11 to 1.39, p<0.01, I2 = 83.5 %).43 48 49 Higher levels of fibrinogen were also associated with exacerbation (SMD 0.23 g/dL, 95% CI 0.14 to 0.33, p<0.01, I2 = 0.0 %).
C reactive protein
Moy et al suggested that combining CRP with step count is a good predictor of acute exacerbations (C-statistic=0.59) and hospital admission (C-statistic=0.69).50 However, de Torres et al (BODE cohort, n=218), reported no statistically significant associations between baseline CRP levels and mortality,33 along with Grolimund et al (ProHOSP, n=469),51 Ferrari et al 26 and Waschki et al.37 There was also no difference in CRP levels at baseline for COPD exacerbation in the COSMIC study.52 Meta-analysis indicated that individuals with higher levels of CRP measured at baseline had a higher risk of early mortality (HR 1.17 per twofold increase, 95% CI 1.06 to 1.28, p<0.01, I2 = 81.5 %). Higher levels of CRP were also associated with COPD exacerbations (SMD 0.12 mg/L, 95% CI 0.04 to 0.21, p<0.01, I2 = 0.0 %) and hospitalisation (SMD 0.33 mg/L, 95% CI 0.13 to 0.53, p<0.01, I2 = 92.8 %). After removing studies with a quality score in the bottom tertile, HRs for mortality increased (1.25–1.31) and decreased for hospitalisation (0.20–0.13). Meta-regression indicated no statistical significant difference for studies with longer follow-up time, with older participants and more recently published (online supplementary figure S13).
White cell count
Only a few studies compared baseline measures with clinical outcomes over time (≥6 months). Several studies reported COPD patients with higher WCC levels at baseline to be at a higher risk of clinical outcomes.28 31 47 53 54 Husebø et al, however, did not find higher baseline measures to be associated with a higher number of exacerbations during 3 years of follow-up.55 Additionally, Grolimund et al (ProHOSP, n=469) did not find a statistically significant difference between WCC levels and mortality.51 Meta-analysis indicated an association between higher levels of WCC at baseline and a higher risk of earlier death (HR 2.07 per twofold increase, 95% CI 1.29 to 3.31, p<0.01, I2 = 75.3 %). However, WCC levels were not associated with exacerbation (SMD 0.05, 95% CI −0.06 to 0.17, p=0.38, I2 = 18.7 %) or hospitalisation (SMD 0.20, 95% CI −0.05 to 0.44, p=0.12, I2 = 72.5 %). After removing studies with a quality score in the bottom tertile, HRs for mortality increased for fibrinogen (5.18–5.99; online supplementary figure S6).
Interleukin 6
Hurst et al (ECLIPSE, n=2138) did not find higher baseline measures to be associated with a higher number of exacerbations.53 Additionally, Waschki et al 37 and Wedzicha et al 56 did not find higher IL-6 baseline levels to be associated with a higher risk of mortality. Meta-analysis indicated no association between IL-6 and earlier mortality (HR 1.10 per twofold increase, 95% CI 0.92 to 1.32, p=0.28, I2 = 66.1 %). Neither was there an association with exacerbation (SMD 0.06, 95% CI −0.02 to 0.15, p=0.16, I2 = 0.0 %). Increased levels were, however, associated with hospitalisation (SMD 0.12, 95% CI 0.04 to 0.20, p=0.01, I2 = 0.0 %).
Interleukin 8
IL-8 levels and its relation with clinical outcomes in COPD is not well reported. Within the ECLIPSE study (n=2138), Hurst et al, found that IL-8 levels at baseline was not a statistically significant predictor for exacerbations after 1 year of follow-up.53 However, Celli et al, who also used data from ECLIPSE (n=1843) did find increased levels at baseline to be associated with a higher risk of mortality after 3 years of follow-up.31 Meta-analysis indicated no association between IL-8 and exacerbation (SMD 0.19, 95% CI −0.40 to 0.79, p=0.52, I2 = 83.5 %).
Tumour necrosis factor-alpha
Celli et al (ECLIPSE, n=1843) did not find a statistically significant difference between those who died after 3 years of follow-up and those still alive.31 Hurst et al (ECLIPSE, n=2138) reported similar findings for exacerbations after 1 year of follow-up.53 Additionally, Groenewegen et al reported no statistically significant difference between the baseline TNF-α measure and clinical outcomes in the COSMIC cohort (n=277) after 1 year of follow-up.52 Meta-analysis indicated no associations between elevated levels of TNF-α and the risk of earlier death (HR 0.94 per twofold increase, 95% CI 0.88 to 1.01, p=0.07, I2 = 0.0 %), nor for exacerbation (SMD 0.04, 95% CI −0.17 to 0.25, p=0.71, I2 = 62.4 %), or hospitalisation (SMD −0.01, 95% CI −0.09 to 0.07, p=0.88, I2 = 0.0 %).
Quadriceps maximum voluntary contraction
In recent years, there has been an increasing interest in examining the predictive value of functional activities of the musculoskeletal system. The quadriceps muscle is of particular interest, being assessed using QMVC as a surrogate marker. However, only two studies assessing the same cohort of patients have assessed QMVC in relation to clinical outcomes, where quadriceps muscle function of 184 patients with COPD using QMVC was found to be a good predictor of mortality after 4 years of follow-up (HR 0.88, 95% CI 0.77 to 1.00) with higher levels reducing risk.13 57
Sniff nasal inspiratory pressure
Moore et al reported a statistically significant association between baseline SNIP and mortality (HR 0.73 per 10 cmH2O, 95% CI 0.63 to 0.84, C=0.68) and suggest that, compared with pulmonary plethysmographs, a test commonly performed to measure functional residual capacity, SNIP is recommended because of its low cost and efficiency.57
No studies included in our systematic review reported associations with SPPB, PWV, CIMT and AIx.
Publication bias
Publication bias was present in most biomarkers for all outcome measures, indicated through asymmetrical funnel plots (online supplementary figure S4). Bias seemed to primarily occur due to the poor quality of small studies, which deviated most from the other studies. Removal of studies that fell outside of the funnel plot did not alter findings.
Discussion
This study systematically summarises and examines the association between multiple outcomes and biomarkers that may potentially better capture systemic problems in patients with COPD and are not yet widely used in clinical practice. Our main findings indicate that patients with stable COPD had higher risks of premature death when presenting with a shorter walking distance and higher resting heart rate, fibrinogen, CRP and WCC at baseline, when followed-up over a period of at least 6 months. Only a shorter walking distance and higher fibrinogen and CRP levels indicated a higher risk of COPD exacerbation. The risk for COPD-related hospital admission was higher with a shorter walking distance and higher resting heart rate and CRP and IL-6 levels.
No studies evaluating SPPB, CIMT, PWV and AIx were included in our systematic review. However, a small number of publications have assessed these in relation to clinical outcomes in COPD (which did not meet our inclusion criteria). Based on a meta-analysis of 17 studies, mainly in the general population, an SPPB score <10 (range 0–12) was found to be predictive of all-cause mortality.58 The gait speed, one of SPPBs components, was also found to predict hospital readmission in elderly patients with COPD.59 The non-invasive CIMT and its role in clinical outcomes in patients with COPD has not been largely investigated. However, it has been shown that patients with COPD, in particular smokers, are at higher risk of an elevated CIMT due to atherosclerotic plaque formation and developing arterial stiffness as a result of hypoxaemia.60–62 Other studies found associations with PWV63 and AIx.64 We have identified gaps in the literature that need to be examined in order to address these research questions, and while the recommendation for clinical utility differs slightly, the evidence across the studies suggest that the use of musculoskeletal measures to assess outcomes in patients with COPD are worth further investigation.
This review has some potential limitations. By focusing on stable (ie, non-hospitalised) patients, our results may not be generalisable to patients with unstable COPD. Additionally, study hetereogeneity exists due to differences between studies in definitions of stable COPD, the duration of stability prior to study enrolment, patient selection criteria, length of follow-up and outcome definitions. We aimed to address this by using random effects modelling using SMDs (which are robust to varying lengths of follow-up65) and sensitivity analysis. We did not have access to individual patient data, which would allow us to model time-to-event data, adjust for a common set of confounders and estimate the discriminative ability of the biomarkers. Where possible, HRs are presented with adjustment for age, sex, BMI and smoking status. Ideally, studies should be adjusted for comorbidities like hypertension and diabetes.66
Other potential sources of bias include, for example, history of sleep apnoea, number of previous hospital admissions prior study enrolment and years of COPD.
Future investigation should focus on evaluating and validating the predictive ability of COPD biomarkers, preferably in large studies with longer follow-up time. Emphasis should be placed on ensuring biomarkers are generalisable (ie, more diversity in ethnicity and comorbidities) and practical for clinical use. Tests such as the 6MWD are not well adopted for clinical practice as they require time and space.32 Future research could focus on the validation of fast and simple tests such as the SPPB or its components. These are easier and faster to conduct, require less space and patients are less likely to require oxygen. Newly developed risk models could help monitor clinically diagnosed patients with COPD in an early stage of disease to identify patients at high risk for mortality, exacerbation and hospitalisation. Some work is already underway, with the SPIROMICS study group developing a debility score aiming to identify COPD patients with debility, that is, extreme breathlessness, decreased exercise capacity and poor health status.67 Additionally, the Evaluating the Role of Inflammation in Chronic Airways disease study cohort could help provide answers to these questions aiming to fill the biomarker gap.
Conclusions
Findings suggest that 6MWD, resting heart rate, fibrinogen, CRP, WCC and IL-6 are associated with clinical outcomes in COPD. The review process elicited very few studies that examined the association between musculoskeletal measures (eg, SPPB and QMVC) and COPD. While the recommendation for clinical utility differs slightly, the evidence across the studies suggest these are worth further investigation.
Acknowledgments
The corresponding author and coauthors had full access to the data in the study and take responsibility for the integrity of the data, the accuracy of the analyses and the decision to submit for publication.
References
Footnotes
Contributors JMF and AMW designed the study. JMF, MTJ, RF, VAPDL, JLM, PS, HW, BW and HM contributed to the data collection. JMF and KLM extracted the data. JMF conducted the analysis and produced the results figures and tables. AMW and KLM provided statistical support. JMF wrote the initial draft of the manuscript. KLM, MIP, IBW and AMW contributed to the writing of the manuscript. All coauthors read and commented on the manuscript.
Funding This study was funded by GlaxoSmithKline (RG79358).
Disclaimer The views and opinions expressed are those of the authors and do not necessarily reflect those of the University of Cambridge. The funder of the study had no role in study design, data collection, data analysis, data interpretation or writing of the report.
Competing interests GlaxoSmithKline, a consortium partner, funded JMF. HM is an employee of GSK and own shares and stock options of GSK Plc. MIP received grants from GSK outside the submitted work. IBW received grants from GSK during the conduct of the study and outside the submitted work.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Most of the data used in the meta-analysis are publicly available. Where data were unpublished and obtained from the corresponding author, summary statistics can be requested.
Patient consent for publication Not required.
Linked Articles
- Airwaves