Article Text

Abstract
Background In children with asthma, web-based monitoring and inflammation-driven therapy may lead to improved asthma control and reduction in medications. However, the cost-effectiveness of these monitoring strategies is yet unknown.
Objective We assessed the cost-effectiveness of web-based monthly monitoring and of 4-monthly monitoring of FENO as compared with standard care.
Methods An economic evaluation was performed alongside a randomised controlled multicentre trial with a 1-year follow-up. Two hundred and seventy-two children with asthma, aged 4–18 years, were randomised to one of three strategies. In standard care, treatment was adapted according to Asthma Control Test (ACT) at 4-monthly visits, in the web-based strategy also according to web-ACT at 1 month intervals, and in the FENO-based strategy according to ACT and FENO at 4-monthly visits. Outcome measures were patient utilities, healthcare costs, societal costs and incremental cost per quality-adjusted life year (QALY) gained.
Results No statistically significant differences were found in QALYs and costs between the three strategies. The web-based strategy had 77% chance of being most cost-effective from a healthcare perspective at a willingness to pay a generally accepted €40 000/QALY. The FENO-based strategy had 83% chance of being most cost-effective at €40 000/QALY from a societal perspective.
Conclusions Economically, web-based monitoring was preferred from a healthcare perspective, while the FENO-based strategy was preferred from a societal perspective, although in QALYs and costs no statistically significant changes were found as compared with standard care. As clinical outcomes also favoured the web-based and FENO-based strategies, these strategies may be useful additions to standard care.
Trial registration number Netherlands Trial Register (NTR1995).
- Asthma
- Health Economist
- Paediatric asthma
Statistics from Altmetric.com
Key messages
What is the key question?
Does the clinical effectiveness of FENO-based and web-based monitoring outweigh healthcare costs and societal costs in children with allergic asthma?
What is the bottom line?
Both FENO-based and web-based monitoring were economically preferred from societal and healthcare perspectives, as compared with standard care.
Why read on?
This paper extends the favourable clinical outcomes of FENO-based and web-based monitoring with a detailed assessment of the health economic effects showing a higher probability of cost-effectiveness of both strategies.
Introduction
Asthma treatment aims at achieving and maintaining asthma control and therefore adjusting therapy is based on regular assessment of the level of asthma control.1 Effective disease management requires simple, reliable and affordable tools to assess asthma control. However, guidelines offer little practical guidance for monitoring asthma in children and in clinical practice a substantial proportion of children does not achieve adequate asthma control which leads to increased healthcare costs and productivity loss of parents.2–5
Web-based self-monitoring may improve asthma control in children.6 A simple and affordable tool that can be offered via internet is the Asthma Control Test (ACT, for children >11 years) or Childhood ACT (for children 4–11 years).7–10 In addition, since chronic airways inflammation is the target for treatment with inhaled corticosteroids (ICS) monitoring of airways inflammation is another opportunity to tailor therapy and improve asthma outcomes.11 ,12 Measuring the FENO is a non-invasive and simple method to quantify eosinophilic airways inflammation.
In a recent study in children with asthma between 4 years and 18 years of age, we evaluated the effectiveness of 1 year treatment based on two different asthma monitoring strategies as compared with standard care: (1) web-based monitoring with monthly ACT and; (2) a 4-monthly FENO-based monitoring strategy.13 The primary end point of symptom-free days did not differ between the three strategies. However, web-based monitoring led to a significant and clinically relevant reduction in ICS dose with similar asthma control, suggesting better, personalised asthma management. The FENO-based strategy improved asthma control as assessed with the ACT without the need for higher ICS doses, and therefore both monitoring strategies might be considered to improve childhood asthma from clinical and patient perspectives.13 However, to date it is unknown to what extent the clinical benefits outweigh the costs and whether the strategies can be recommended from a health economic perspective.
To that end, we performed an economic evaluation alongside the randomised trial.13 We hypothesised that web-based monitoring of asthma control and monitoring of airways inflammation by FENO, in addition to standard care, are cost-effective.
Methods
This economic evaluation was conducted alongside the ‘Better Asthma Treatment: Monitoring with ACT and Nitric oxide’ study. This three-arm multicentre randomised, partly blinded parallel group trial with 12 months follow-up was conducted from February 2010 through November 2012 in The Netherlands. All parents and all children above 12 years of age gave written informed consent before entering the study. Procedures were in accordance with the Helsinki Declaration, and this trial is registered in the Netherlands Trial Register (NTR1995). The methodological details of the trial are reported elsewhere and briefly summarised here.13 The CONSORT checklist is available online.
Patients
Children with allergic asthma (age range 4–18 years) were recruited from five general hospitals and two tertiary referral centres as described previously.13 Patients used ICS during at least 3 months before the study. Exclusion criteria were active smoking, lung disease other than asthma, recent (<1 year) or multiple admissions to an intensive care unit for asthma, and/or the use of omalizumab.
Design
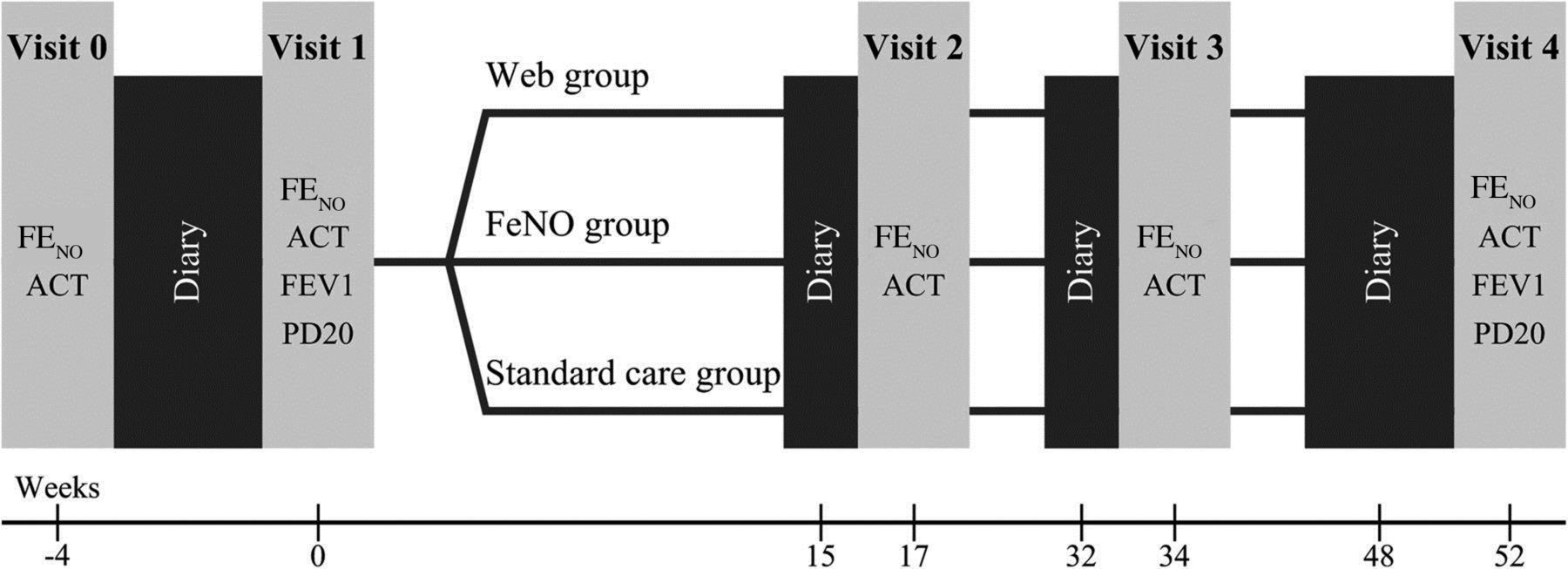
Children were automatically and randomly allocated to one of three strategies by a randomisation programme in a 1:1:1 ratio: (1) standard care; (2) web-based monitoring and (3) FENO-based monitoring, stratified for age (<12 years or ≥12 years), centre and dosage of ICS. Patients visited the outpatient clinic at a baseline visit 4 weeks prior to randomisation and every 4 months over the course of 1 year. At these visits asthma control was assessed using the ACT score. In standard care the ACT score during clinic visits directed treatment. In the web group, treatment was adapted monthly according to the web-based ACT score, while in the FENO group, treatment was adapted to FENO and ACT score at clinic visits every 4 months (figure 1). Patients in all three strategies filled out questionnaires as described below at baseline and after 4 months, 8 months and 12 months.

Time line study protocol. ACT, Asthma Control Test; PD20, provocation dose causing a 20% decline in FEV1.
Utilities and quality-adjusted life years
The health economic outcome of this study was the costs per quality-adjusted life year (QALY) gained from healthcare and societal perspectives. Utilities reflect the individual preferences for different health states. Health-related quality of life was reported using the EuroQoL classification system (EuroQoL-5 dimensions (EQ-5D) version 3L).14 In patients under 12 years of age, their parents filled out the questionnaire. In children 12 years and older, the patients filled out the questionnaires aided by their parents.14 QALYs were obtained by calculating the area under the health state utility curve based on the Dutch tariff of EQ-5D.15 In addition, we calculated QALY estimates using EuroQoL-visual analogue scale (EQ-VAS) scores,16 but according to protocol the EQ-5D classification system was used as input for the cost-effectiveness analysis.
Costs
We assessed the costs from both healthcare and societal perspectives, using a cost questionnaire. Patients reported healthcare use, paid labour absenteeism and hours spent on unpaid labour.
Healthcare costs consisted of both asthma and non-asthma-related contacts with healthcare providers (clinical consultations, telephonic consultations and home visits), emergency room visits, hospital admissions and medication. We requested the participant's permission to collect pharmacist data about medications. Total medication costs were assessed by obtaining all medication prescriptions from local pharmacy records, using standard Dutch pricing.6 In the FENO-based and web-based strategies, additional costs of the intervention were added to these costs. Patients reported each type of consultation for each type of healthcare provider (general practitioner, paediatrician, other type of specialist, paramedic or complementary care) separately. We used standard Dutch prices for consultations per type of healthcare provider,17 and standard prices for medication determined by the Dutch authority of insurance companies. The intervention costs for the FENO-based strategy consisted of purchase and exploitation costs of the FENO analyser, and for the web-based strategy we estimated the information and communications technology costs and the costs of a nurse practitioner who communicated with the children or parents when they filled out the ACT.
Societal costs consisted of the above-mentioned healthcare costs, time and travel costs for that healthcare and the loss of productivity in both paid and unpaid self-reported labour. Paid labour absenteeism due to the child's health for the parents (for children <12 years of age) or for the child (for children ≥12 years of age) was valued using age-specific wages.18 Hours spent on unpaid volunteer work (housekeeping, grocery shopping, etc) were valued using a standard voluntary work compensation and relative to the average hours in the study populations (so negative costs reflect above-average hours of unpaid work). Total costs were obtained by adding the costs of three relevant categories: all healthcare costs, productivity loss and intervention costs, consisting of additional costs for the measurement of FENO-based or web-based support. Because the follow-up was 1 year, costs were not discounted.
Statistical analysis
Patients were analysed according to intention to treat. To correct for possibly selective non-response, we first imputed missing data using linear regression modelling. We constructed 10 sets of imputations, with study group, age, gender, centre and available utilities as regression variables. Then we used Rubin’s rules to congregate the imputation sets to single values.19 After imputation we compared the differences between the different strategies performing independent sample Student's t tests with the following pairwise contrasts: standard care versus web-based, standard care versus FENO-based and FENO-based versus web-based for each category of costs. As there is still debate about how to adjust for multiple testing, and we didn't specify how to adjust for this in our protocol, we chose to report non-adjusted p values below 0.05, which should be interpreted in the light of multiple comparisons. Statistical uncertainty of cost-effectiveness was analysed using the net benefit (NB) approach.20 The NB is defined as λ×ΔQALY−Δcosts, where λ is the willingness to pay for a gain of one QALY. This way, the observed QALY difference is reformulated into a monetary difference. To assess the likelihood of cost-effectiveness of the intervention strategies, we used two different perspectives: a healthcare perspective and a societal perspective, as described above. The probability of each strategy to be the most cost-effective of the three strategies was assessed in acceptability curves using bootstrap analysis, from healthcare and societal perspectives at different λ levels. We assessed whether there were differences between the study arms in the EQ-5D dimensions using mixed models. All analyses were performed with Stata/IC V.11.0.
Results
Recruitment and baseline characteristics
In total, 481 children satisfied the inclusion criteria and were approached for the study, of whom 201 refused to participate. Prior to randomisation, eight children were excluded for non-adherence to the study protocol. The remaining 272 participants were randomised over the different study arms: 89 in the standard care group, 91 in the web-based group and 92 in the FENO group. Missingness of data comprised 10 out of 1088 records (0.9%). Baseline characteristics are shown in table 1. There were no significant differences between the strategies for age, sex, FENO, lung function and ICS dose.13 Although asthma control at baseline was better in the web-based group compared with the FENO-based group, asthma control was not significantly different from the standard care group for both novel monitoring strategies.13 In addition, there were no statistically significant differences in patient utilities at baseline between the strategies.
Baseline characteristics
Costs
The healthcare costs of the different strategies are shown in table 2. Total healthcare costs varied between €837 and €924 per patient per year across the different strategies, which was not significantly different. Among healthcare cost categories, only the amount of nurse practitioners’ consultations differed significantly between the strategies: the web-based strategy accounted for an average of €129 annual expenditure (1.79 consultations per year per patient×€72 per consultation), whereas standard care accounted for €86 (1.20 consultations per patient per year, p=0.001) and FENO-based care accounted for €96 (1.33 consultations per patient per year, p=0.01).
Health economic outcomes
Patient utilities
The scores of the EQ-5D domains are shown in table 3. These domains range from 1 to 3, where 1 represents the most favourable score. There were no between-strategy differences in EQ-5D domains.
Average scores of EQ-5D subdomains over 1 year follow-up
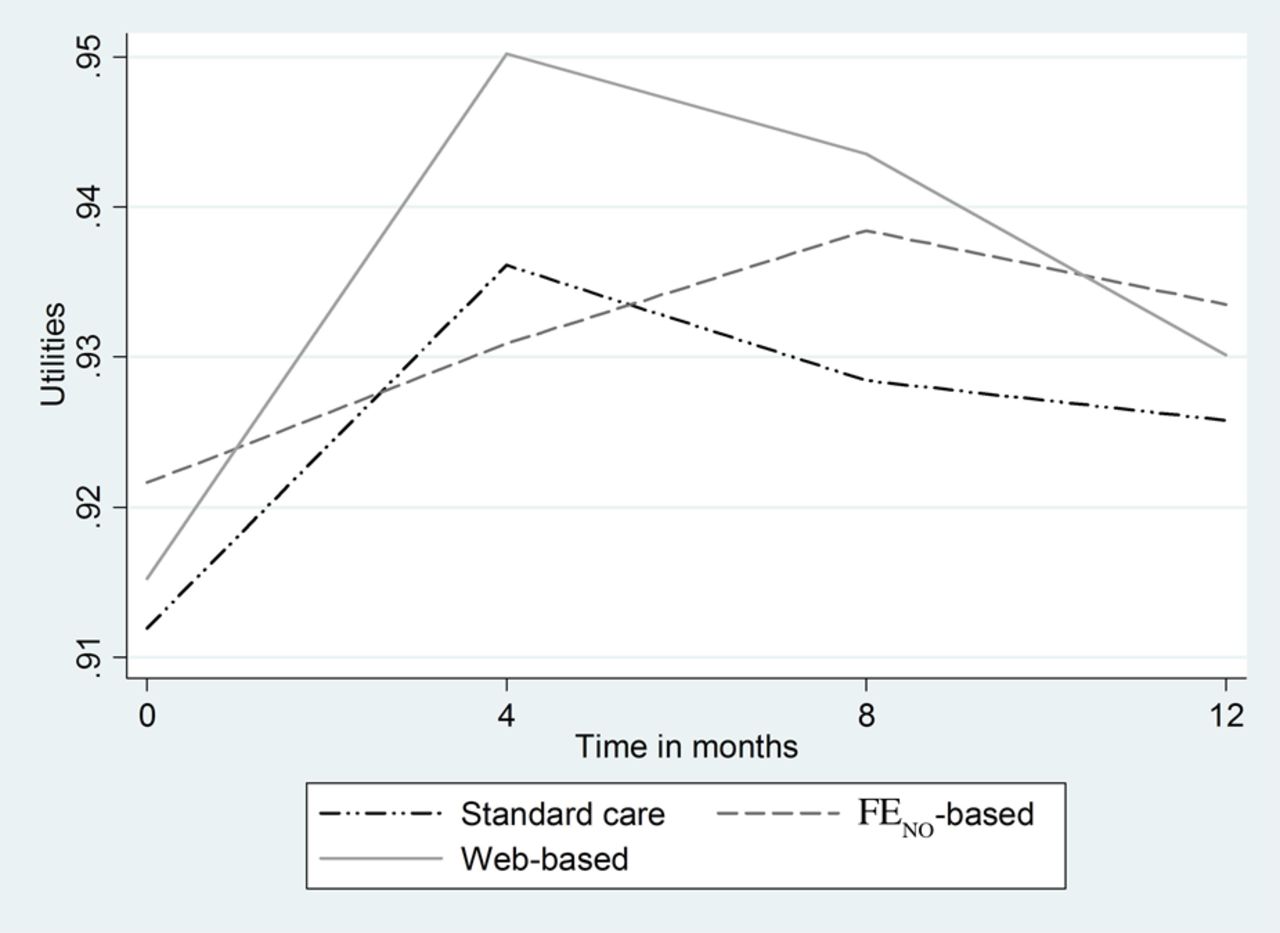
The changes in patient utilities during follow-up are shown in figure 2. The best outcomes were seen in the web-based strategy at 4 months follow-up (p=0.26 compared with standard care, p=0.15 compared with FENO). Although the differences of these outcomes were statistically non-significant, they accounted for the higher overall QALY in the web-based strategy. The standard care group and the web-based group show a similar pattern over time, with a peak after 4 months follow-up, with a subsequent decrease in quality of life. The FENO-based strategy offers a more constant pattern, with a slight non-significant peak after 8 months follow-up.

Patient utilities over time.
QALYs are shown in table 2. These results, although statistically not significantly different, slightly favour the web-based strategy. The mean utility scores across the strategies vary between 0.928 and 0.939, indicating relatively high utilities in this population.
Cost-effectiveness
The probability that a strategy is more cost-effective compared with the two other strategies at different willingness to pay per QALY levels was assessed by cost-effectiveness acceptability curves (CEACs) from a healthcare perspective (figure 3A) (based on healthcare costs only) and from a societal perspective (including both healthcare costs and costs due to loss of productivity) (figure 3B). From a healthcare perspective, the web-based strategy showed the highest probability of cost-effectiveness over a wide range of willingness-to-pay values (€10 000–€100 000/QALY). Specifically, at a generally acceptable willingness-to-pay threshold of €40 000/QALY,21 ,22 the web-based strategy was 77% likely to be the most cost-effective, while this was 3% for the standard care and 20% for the FENO-based strategy. At a threshold of €80 000/QALY, which is mentioned in the Netherlands as the maximum costs considered acceptable,21 ,22 the web-based strategy has an 85% likelihood of being most cost-effective. From a societal perspective, uncertainty was substantially higher, favouring the FENO-based strategy over a wide range of willingness-to-pay values, which has the highest 83% chance of being most cost-effective at a willingness to pay of about €40 000/QALY (figure 3B).

{kind=link}
{kind=link}
{kind=link}
(A) Cost-effectiveness acceptability curve—healthcare perspective. (B) Cost-effectiveness acceptability curve—societal perspective. QALY, quality-adjusted life year.
Discussion
In this study we assessed the cost-effectiveness of a web-based and an FENO-driven monitoring strategy compared with standard care in children with asthma in secondary care and tertiary care. Both monitoring strategies were introduced in addition to standard care. Although we found no significant differences in costs and QALYs between the strategies, the web-based strategy was most likely to be cost-effective over a wide range of acceptable willingness-to-pay values for a gain in quality-adjusted life and was the preferred strategy from the healthcare perspective. From a societal perspective the FENO-based strategy was the preferred strategy with an overall higher probability of cost-effectiveness as compared with the web-based strategy and standard care.
Studies regarding the cost-effectiveness of monitoring strategies with asthma are scarce, especially in children.23–25 This study was performed alongside a clinical study which showed that both the web-based monitoring strategy and an FENO-driven strategy did not improve the number of symptom-free days more than the standard care strategy.13 However, monthly web-based symptom monitoring did result in a clinically relevant decrease of ICS, while maintaining asthma control. Remarkably, the FENO-based strategy improved asthma control as assessed with ACT and as compared with standard care, without increasing medications. This cost-effectiveness analysis fits in with the results of the clinical outcomes, since it is likely that improved asthma control in the FENO-based strategy positively impacts productivity costs and therefore the cost-effectiveness from a societal perspective.5 We observed relatively high patient utilities of around 0.93 in this population. Hence it would be interesting to compare the different strategies in a population with more severe disease, accompanied with more room for improvement.
The results of this study might be influenced by differences at baseline, missing data or selection bias. We think that this was unlikely for the following reasons. First, with respect to patient utilities there were no statistically or clinically important differences between the strategies at baseline. However, asthma control was somewhat better, although not statistically significant, in the web-based strategy at baseline and therefore left less room for improvement. Therefore, it is unlikely that the statistically non-significant improvement in utilities in the web-based strategy can be explained by baseline differences. Second, there was a low frequency of missing values, which was not associated with a particular strategy, and sensitivity analyses using different imputation methods all showed similar results. Third, a potential limitation of this study might be selection bias at enrolment. About 50% of eligible children refused participation. However, non-participating children did not differ from participants regarding age, lung function and ICS dose.13 As children from seven clinics all over the Netherlands were included in this study, and inclusion criteria were rather loose, this study is representative for Dutch children with allergic asthma treated in second line and third line centres. Finally, socioeconomic factors were not included as randomisation strata.
One of the strengths of this study was the comprehensive coverage of costs by questionnaires and medication prescriptions from local pharmacy records. Besides the more clearly defined healthcare costs, we assessed productivity costs by a number of relevant variables. There is increasing evidence that children with uncontrolled asthma experience asthma-related night-time awakenings, and it is not unlikely that their caregivers too are awakened more often at night.5 This could be a driving factor in impaired work performance the next day.5 However, the valuation of productivity losses of children and their parents is still a methodological challenge. No consensus exists about the calculation of costs of unpaid labour, parent's absence of work due to their children's health status and the long-term economic impact of absence of school. Therefore the outcome from the societal perspective might be more sensitive to subjective choices of valuation than outcomes from the healthcare perspective.
How can we interpret the current findings? The conclusions could be more convincing and persuasive if the differences in utilities and costs were both statistically significant. However, a CEAC incorporates these uncertainties and could hypothetically be more significant than the costs and utilities separately. Therefore a CEAC offers additional insights in the cost-effectiveness to the utilities and costs alone. The CEACs show a probability for the web-based strategy to be cost-effective of 77% and 83% from a healthcare perspective and a societal perspective, respectively, at a generally accepted willingness to pay of €40.000. Even at a willingness to pay of €20.000, the web-based strategy had clearly the highest chance of being cost-effective. Therefore, although our results do not establish the cost-effectiveness beyond any scientific doubt (ie, beyond p≤0.05 statistical significance), this study provides relevant and useful information for policy making, including an appropriate reflection of the associated uncertainty. One could argue that the cost-effectiveness of web-based care might be further improved if some of the 4-monthly clinic visits are substituted by an e-consult. In addition, the FENO-based strategy was overall the preferred strategy from the societal perspective irrespective of the uncertainty in the valuation of productivity costs.
We conclude that both web-based and FENO-based monitoring on top of standard care have additional value and are likely to be more cost-effective than standard care alone. This is in line with the earlier findings of additive value in clinical outcomes.13 The present analysis supports the case for a web-based and/or FENO-driven monitoring strategy in addition to standard care in children with allergic asthma from a health economic perspective.
Acknowledgments
The authors thank the involved paediatricians, paediatric asthma nurses and lung function technicians for their help and active guidance throughout the study: Simone Suelmann, Hannie Achterberg, Bas Harzing, Dorine de Hond, Saskia ten Raa (Amphia Hospital), Coosje Sintnicolaas, Cindy Hugen, Jessie Jacobs, Petra Theissen (Radboud University Medical Center), Christel Linssen, Martin Claassens (Catharina Hospital), Linda van Gilst, Gracé Theunissen, Mark Holewijn, Annejet Plaisier (Rijnstate Hospital), Renata de Ridder, Else Stoter (De Kinderkliniek), Prof Wim van Aalderen, Saeeda Lone and Erik-Jonas van de Griendt (Amsterdam Medical Center).
References
Footnotes
Contributors MWP, JCdJ, AAV-V, HJB, AML, NJvdB, PJM and JKS were involved in the design of the study. SV-vB, AAV-V, HJB, AML, NJvdB, PJM, MWP and JCdJ participated as investigators in this trial, recruited patients and performed the treatments. TB, SV-vB, WBvdH, JKS contributed to data analysis. TB, JKS and MWP drafted the manuscript, which was critically revised by all authors. The manuscript has been read and approved by all authors.
Funding This study was funded by Lung Foundation Netherlands, The Netherlands Organization for Health Research and Development (ZonMW) and Fund NutsOhra.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Medical Ethics Committee, Erasmus Medical Center, Rotterdam.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves