Article Text

Abstract
Background Ototoxicity is a severe side effect of aminoglycoside antibiotics. Aminoglycosides are recommended for the treatment of multidrug-resistant TB (MDR-TB). N-Acetylcysteine (NAC) appears to protect against drug- and noise-induced hearing loss. This review aimed to determine if coadministering NAC with aminoglycoside affected ototoxicity development, and to assess the safety and tolerability of prolonged NAC administration.
Methods Eligible studies reported on the efficacy of concomitant NAC and aminoglycoside administration for ototoxicity prevention or long-term (≥6 weeks) administration of NAC regardless of indication. Pooled estimates were calculated using a fixed-effects model. Heterogeneity was assessed using the I2 statistic.
Results Three studies reported that NAC reduced ototoxicity in 146 patients with end-stage renal failure receiving aminoglycosides. Pooled relative risk for otoprotection at 4–6 weeks was 0.14 (95% CI 0.05 to 0.45), and the risk difference was −33.3% (95% CI 45.5% to 21.2%). Eighty-three studies (N=9988) described the administration of NAC for >6 weeks. Abdominal pain, nausea and vomiting, diarrhoea and arthralgia were increased 1.4–2.2 times.
Discussion This review provides evidence for the safety and otoprotective effect of NAC when coadministered with aminoglycoside. It represents a strong justification for a clinical trial to investigate the effect of concomitant NAC treatment in patients receiving aminoglycosides as part of MDR-TB treatment.
- Tuberculosis
Statistics from Altmetric.com
Key messages
What is the key question?
Does coadministration of N-acetylcysteine (NAC) with aminoglycosides prevent the development of ototoxicity and is it safe?
What is the bottom line?
Coadministration of NAC reduces the risk of ototoxicity by 80% and was found to be safe.
Why read on?
NAC may be an effective strategy to reduce ototoxicity in patients treated with aminoglycoside in the context of multidrug-resistant TB.
Introduction
Ototoxicity is a potentially severe side effect of aminoglycoside antibiotics. Aminoglycosides induce apoptosis of the inner and outer hair cells—the auditory and vestibular sensory receptors within the cochlea. This apoptosis is mediated by disruption of mitochondrial protein synthesis with the subsequent generation of free radicals.1 ,2 As the sensory epithelium of the mammalian cochlea has little regenerative capacity,3 this apoptosis leads to irreversible loss of hearing and balance.4 Hearing loss, which mainly affects high-frequency tones, may progress even after discontinuation of the drug because of the accumulation of free radicals and is irreversible.5
Multidrug-resistant (MDR)-TB is defined as resistance to isoniazid and rifampicin, with or without resistance to other anti-TB drugs. The second-line injectable drugs, including the aminoglycosides (amikacin and kanamycin) and the polypeptides (capreomycin), are among the main anti-TB antibiotics used for the treatment of MDR-TB, with a recommended minimum treatment duration of 8 months.6 If aminoglycoside-induced hearing loss is detected early, through systematic and regular audiological examination, it may be possible to intervene before the hearing loss reaches the frequencies that might affect communication (mid- and low-frequency ranges). However, audiology assessment is often inadequate in both resource-limited and -rich settings, and even regular assessment may not be timely enough to prevent rapid hearing loss for some patients. In addition, the incidence of, and risk factors for, ototoxicity in patients treated for MDR-TB remain poorly characterised. A recent systematic review identified 35 studies reporting the frequency of ototoxicity in patients receiving MDR-TB treatment, but the majority (86%) of these studies failed to specify the testing and classification methods used. In the five studies that used standardised testing and classification methods, the frequency of ototoxicity ranged from 18% to 62%.7
There are limited interventions available to prevent or ameliorate hearing loss in patients receiving second-line injectable drug treatment for MDR-TB. Streptomycin (an aminoglycoside previously used in retreatment of TB but now rarely used) and capreomycin are thought to be less ototoxic than amikacin or kanamycin,8 ,9 but may be less efficacious.10 Increasing the dose interval to thrice weekly rather than daily has not been shown to have any impact on ototoxicity.8 Although therapeutic drug monitoring is recommended for amikacin and streptomycin, this is not readily available for capreomycin and kanamycin, particularly in low-resource settings where the majority of MDR-TB is managed. The main options that can be used to prevent the progression of hearing loss once it has been detected include stopping the drug, reducing the dose, or increasing the dose interval. However, none of these strategies has been systematically evaluated, and, to date, evidence of any benefit of alteration in dose and interval is lacking. Furthermore these options may reduce treatment efficacy and lower the chance of cure through compromising the regimen.
As the cochlear hair cell damage is caused by reactive oxygen species, it is theoretically possible to mitigate these effects by coadministration of antioxidants.11 ,12 Aspirin, an established antioxidant, has been shown to protect against hearing loss in adults treated with gentamicin.13 More recently, several studies in patients undergoing dialysis have shown a protective auditory effect of N-acetylcysteine (NAC) when coadministered with either gentamicin or amikacin.14–17 NAC, a thiol-containing antioxidant, is a successful and established treatment which ameliorates hepatic and renal toxicity in acetaminophen (paracetamol) overdose and contrast-induced kidney injury.18 ,19 Moreover, NAC has been used in both animals and humans to reduce cisplatin- and noise-induced ototoxicity.20–26
NAC has been available in clinical practice for several decades, and is predominantly used to treat acetaminophen intoxication. It can be administered intravenously, orally or by inhalation. Oral bioavailability is 6–10% because of first-pass metabolism.27 Intravenous NAC carries a small risk of an anaphylaxis-like reaction, including rash, pruritus, angioedema, bronchospasm and, rarely, hypotension.28 NAC given orally is associated with low toxicity, with reported non-life-threatening side effects including nausea, vomiting, rhinorrhoea, pruritus and tachycardia.
To date, studies investigating whether NAC can prevent aminoglycoside-induced ototoxicity have only evaluated the administration of NAC for short durations (10–14 days), and no studies have evaluated the impact of NAC on the polypeptides. However, if NAC were to be used in the context of MDR-TB to reduce aminoglycoside-induced ototoxicity, it would need to be administered for many months. NAC has been used for prolonged periods in patients with cystic fibrosis, COPD and psychiatric disorders.29–31 To date, however, studies have not specifically evaluated the safety profile and side effects associated with prolonged NAC use.
In order to assess the potential for NAC use in MDR-TB treatment, this review aimed to determine the effect of NAC on the development of ototoxicity when coadministered with aminoglycosides, as well as the safety and side effect profile of prolonged (>6 weeks) NAC administration.
Methods
This review was conducted according to the criteria of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses group, and a protocol was developed before the review was conducted.32
Randomised controlled trials and comparative observational studies were eligible for inclusion if they reported efficacy of concomitant NAC administration on ototoxicity prevention in patients receiving aminoglycoside treatment or if NAC was administered long term (≥6 weeks) regardless of indication. Case reports and case series (<20 patients) were excluded. No date, geographical or language restrictions were applied.
The primary outcome for the efficacy review was ototoxicity (proportion with any hearing loss, proportion with tinnitus and/or vertigo, and degree of hearing loss across different auditory frequencies). The primary outcome measures for the safety review included the number of adverse drug reactions, the number of individuals with an adverse event and/or side effect, and the number of individuals with each specific side effect associated with ≥6 weeks NAC administration. Secondary outcomes included the number of adverse drug reactions resulting in treatment discontinuation and mortality, and the total number of discontinuations and deaths.
Search strategy
A compound search strategy was developed (see online supplementary table S1) to identify all relevant studies regardless of language or publication status. The following electronic databases were searched: Medline (OVID), Embase (OVID), Web of Science, Current Controlled Trials, and the Cochrane database of systematic review. All references were imported into EndNote, and titles and abstracts were examined after duplicates were removed independently by two reviewers (WFE and KK). The full-text articles of all potentially relevant studies were obtained, and the inclusion criteria were applied using a standardised eligibility form. The full text of studies included in 26 previously published reviews investigating the effect of NAC on various chronic conditions was obtained and the studies were screened by two authors (WFE and KK) for inclusion.29 ,31 ,33–57 Reference lists of all studies identified by the above methods and bibliographies of systematic reviews or meta-analyses were examined. Final agreement on study inclusion was determined through consensus (WFE, KK).
Data extraction and management
Data extraction was performed independently, in duplicate, using a standardised data extraction form. Data regarding efficacy included information on the intervention (number of individuals in the intervention (receiving NAC) and control groups, and dose, frequency, duration and serum concentration of aminoglycoside and NAC), outcomes (number of individuals with evidence of ototoxicity per group) and patient characteristics (age, sex and presence of comorbidities). For the review investigating safety, the underlying condition for which NAC was administered, exclusion criteria, age, sex and comorbidities were recorded, as well as NAC dose, frequency and duration, number of adverse events, number of total deaths and withdrawals attributable to NAC.
Quality of included studies
For randomised trials investigating the efficacy of ototoxicity, the Cochrane risk of bias tool for quality assessment of randomised controlled trials was used, and this information was used to inform an overall assessment of quality using GRADE. Studies reporting safety data were assessed taking into account the design (retrospective/prospective), allocation of intervention (randomised, non-randomised), placebo use, blinding of participants and/or investigators, and monitoring strategy.
Data analysis
Relative risk (RR), risk difference and the frequency of events and corresponding 95% CIs for prevention of otoxicity and side effects/adverse events were calculated. For relative effect measures, the Haldane method was applied in the event of zero outcomes in one arm; for frequencies, data were transformed before pooling using standard methods.58 ,59 Data were pooled using a fixed-effects model, and heterogeneity assessed using the I2 statistic.60 Pooled frequency estimates, risk ratios, risk difference and corresponding 95% CIs for specific side effect, total withdrawals and death and withdrawals attributable to NAC were calculated. Only placebo-controlled studies and studies in which solely NAC was administered were included to calculate the pooled estimates for side effects. Weighted medians were calculated for dosage and duration of NAC. All data analysis was performed using Stata V.12.0.
Results
From 5941 unique citations identified, 86 studies were included in this review, among which only three studies reported on the efficacy of NAC to prevent ototoxicity in the context of aminoglycoside use, and 83 reported on long-term (≥6 weeks) NAC use for other purposes (see online supplementary figure S1). No studies assessing the use of NAC together with aminoglycoside for the treatment of MDR-TB were indentified.
Prevention of ototoxicity
Three randomised trials reported on the efficacy of NAC to prevent ototoxicity including a total of 146 patients with end-stage renal disease receiving aminoglycosides for the treatment of bloodstream infections (table 1). Two of these trials were open-label,14 ,16 and one was a randomised, placebo-controlled trial.17 Patients received 600 mg NAC twice daily for the duration of aminoglycoside treatment,16 for a total of 14 days17 or for up to 7 days14 after completion of aminoglycoside treatment. The aminoglycosides used were amikacin (n=2) and gentamicin (n=1). Two of the studies measured the mean hearing loss (in dB) 1–2 and 4–6 weeks after enrolment and found a significant reduction in aminoglycoside-induced hearing loss at both time points.14 ,16 The pooled RR for otoprotection at 4–6 weeks was 0.14 (95% CI 0.05 to 0.45) and the pooled risk difference was −33.3% (95% CI −45.5% to −21.2%) (figure 1). One study compared transient-evoked otoacoustic emissions (OAEs) and distortion-product OAEs among 23 patients receiving placebo and 23 receiving NAC. This study reported a significant improvement in patients receiving NAC at 1500 and 2000 Hz when measured using transient-evoked OAEs and at 1000 and 800 Hz in terms of distortion-product OAEs.17 Overall the aminoglycosides caused the greatest hearing loss at high frequencies, and so it was at these frequencies that the most protective effect of NAC was seen.
Studies investigating the effect of NAC in preventing aminoglycoside-induced ototoxicity

Effect of N-acetylcysteine on aminoglycoside-induced ototoxicity.
The risk of bias was high because two of the three trials were open-label and did not include a control group with placebo (table 2). The overall quality of the evidence was rated as low/very low because of risk of bias and indirectness (different patient population).
Quality assessment of studies included to assess the effect of NAC on aminoglycoside-induced ototoxicity
Long-term NAC use
We identified a total of 83 studies describing the administration of NAC for >6 weeks. NAC was used for psychiatric (N=15), respiratory (N=26) and rheumatological conditions (N=6), blood-borne viruses (N=14), kidney disease (N=6), obstetric and gynaecological conditions (N=5), male infertility (N=2) and other conditions (N=9) such as non-alcoholic fatty liver disease, diabetes mellitus and Alzheimer’s disease (see online supplementary table S2). The majority of studies were randomised, placebo-controlled trials (N=52); the remainder were randomised, placebo-controlled crossover trials (N=11), randomised crossover trials without placebo (N=2), randomised trials without administration of a placebo (N=17), and a quasi-experimental study with patients choosing to take NAC (N=1). Six studies described the administration of NAC or placebo in combination with metformin, cotrimoxazole, omeprazole, lipoic acid and interferon. A total of 5014 patients received a median of 1200 mg (IQR 600–1800) of NAC per day over a median of 24 weeks (IQR 12–54), and 4974 patients served as a control group. The majority of studies were conducted in Europe (N=44), and 13 studies were conducted in the USA. The age of participants ranged from 5 to 80 years, and severe liver and renal impairment was common. Two studies were conducted exclusively among pregnant woman, with a total of 220 pregnant woman receiving NAC. Specific side effects were reported in only 23 (28%) studies. A statement regarding adverse drug reactions was included in 32 (39%) studies in the results section (see online supplementary tables S3 and S4). The remaining 28 (34%) studies provided no information on adverse drug reactions.
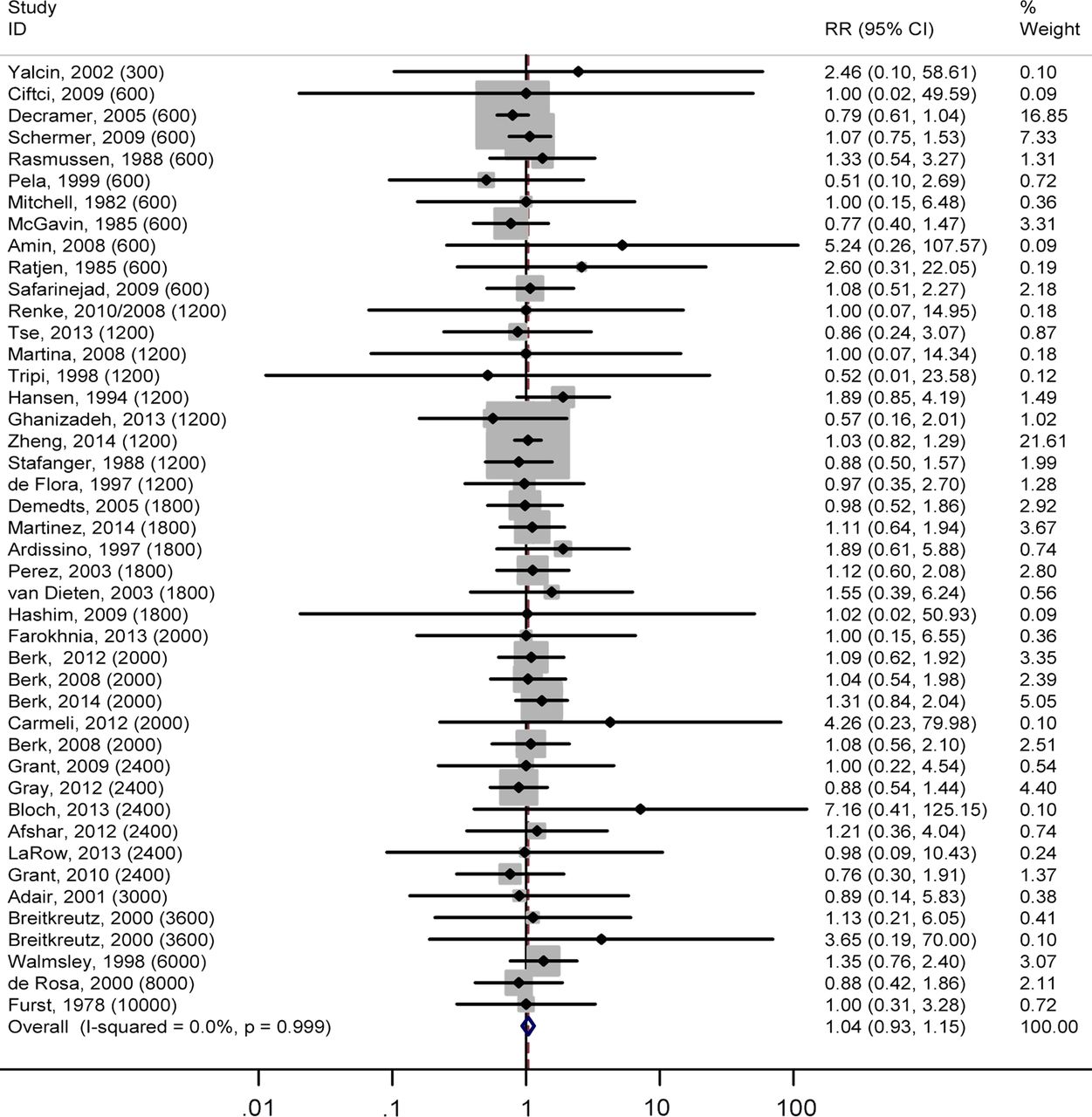
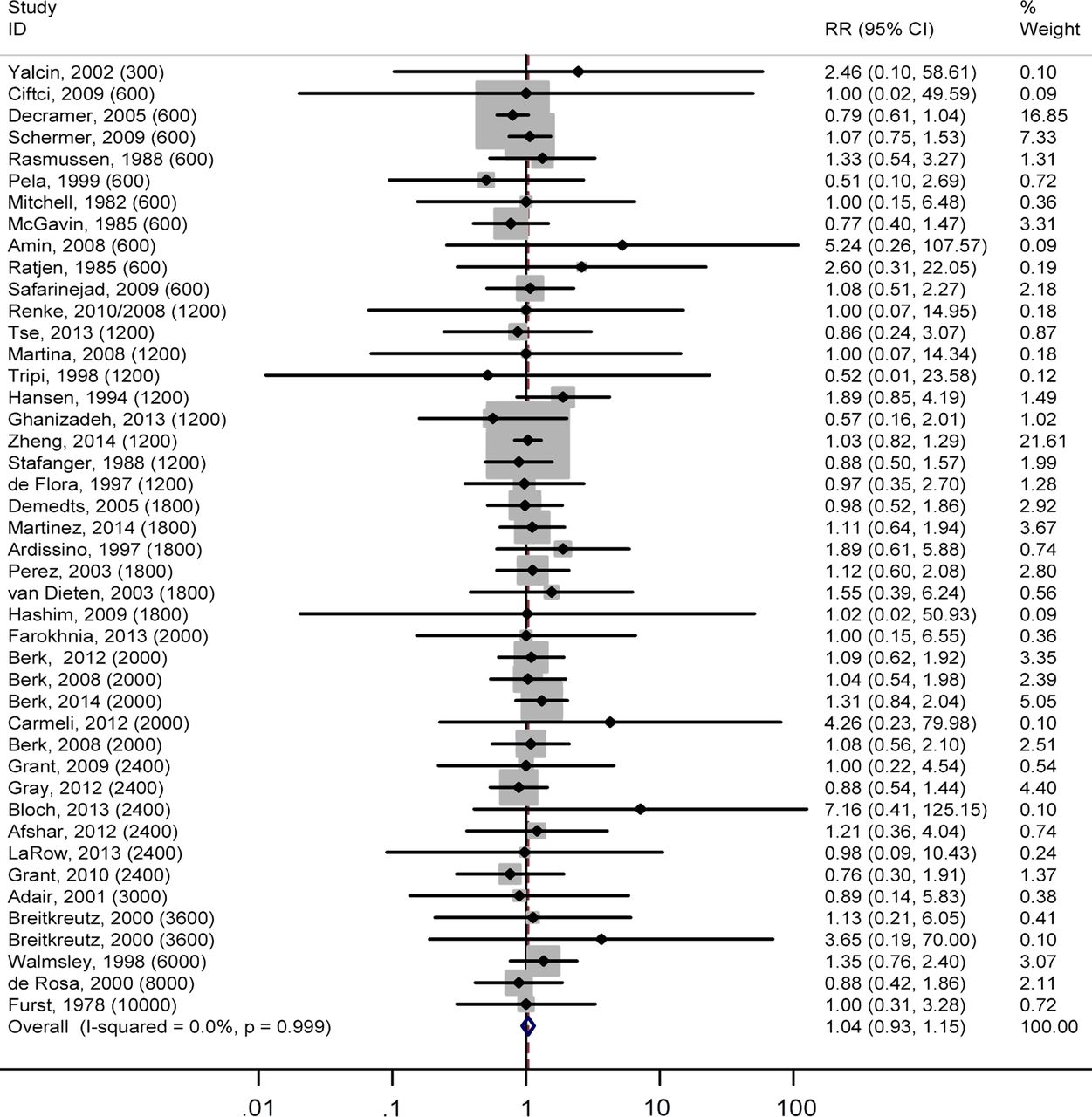
More than half of the studies (n=49) reported the number of patients withdrawn from the study; of those, 34 reported the reason for withdrawal. No deaths were reported as being attributable to NAC administration. There was no difference in the risk of overall withdrawal with a pooled RR of 1.06 (95% CI 0.96 to 1.17, I2 0%) and a pooled risk difference of 0.9% (95% CI 0.6% to 2.5%, I2 0%) in the NAC compared with the control group. Furthermore, there was no increased risk of withdrawal attributable to NAC (pooled RR 0.74 (95% CI 0.59 to 0.93, I2 31%)) and the pooled risk difference was −1.6% (95% CI −2.8% to 0.0%, I2 67%) when comparing NAC with placebo or control group (figure 2). The pooled mortality was 1.1 (95% CI 0.91 to 1.31, I2 0%) across the seven studies reporting data on deaths.
{kind=link}
{kind=link}
Risk of withdrawals attributable to N-acetylcysteine.
Pooled estimates for specific side effects are presented in table 3. The most commonly reported side effects were abdominal pain, nausea, and vomiting and diarrhoea. The risk of abdominal pain (pooled RR 1.4 (95% CI 1.1 to 2.8)), nausea and vomiting (pooled RR 2.0 (95% CI 1.3 to 3.0)), diarrhoea (pooled RR 1.8 (95% CI 1.0 to 3.2)) and arthralgia (pooled RR 2.2 (95% CI 1.2 to 4.1)) were all significantly increased in patients receiving NAC compared with placebo. However, the pooled risk differences for all these side effects were relatively small, ranging from 1.6% for diarrhoea to 6.1% nausea. The risks of headache, rash, dizziness, cramps and drowsiness were not significantly increased.
Pooled estimates of the frequency of specific side effects with risk ratios and risk differences
Quality assessment was challenging, as procedures for side effect ascertainment were not reported. Furthermore, the majority of studies failed to report death and discontinuation of treatment because of side effects (see online supplementary table S5).
Discussion
This review identified three randomised trials reporting a protective effect of NAC in preventing aminoglycoside-induced ototoxicity in patients with end-stage renal failure. The short duration of aminoglycoside administration (maximum 3 weeks) and the selected patient population mean that limited inference regarding the applicability of these results to MDR-TB can be made. The overall quality of evidence informing this intervention was rated as low.
The safety of prolonged NAC administration was also addressed in this review, with 83 studies identified in which oral NAC was administered for a minimum of 6 weeks. Specific side effects were only reported in 23 of 83 studies included for review. Pooled RRs for specific adverse side effects showed a 1.4–2.2 times increased risk of abdominal pain, nausea and vomiting, diarrhoea and arthralgia in patients receiving NAC compared with placebo. The proportion of patients developing specific side effects was highly heterogeneous across studies, which is not surprising given the variety of clinical conditions, the wide age ranges, and difference in NAC dosing. The pooled risk difference was highest for nausea and vomiting (6.1%) and lowest for diarrhoea (1.8%). Thirty-two studies commented on side effects and adverse events without providing detailed information on specific adverse side effects. An additional 28 studies administered NAC, but neither reported nor commented on side effects. Most studies did not report data on discontinuation of treatment due to adverse events. However, withdrawal overall and withdrawal attributable to side effects was comparable in patients receiving NAC and placebo or control, where reported. Furthermore, mortality was comparable in the few studies that reported deaths stratified by treatment group.
This review provides evidence for the safety of prolonged NAC administration. However, the reported side effects associated with NAC use are potentially additive to those associated with second-line TB drugs other than the aminoglycosides.61 ,62 Gastrointestinal side effects, such as nausea and vomiting, are associated with thioamides, para-aminosalicylic acid and fluoroquinolones, and, while not life-threatening, severely affect regimen tolerability and therefore potentially default from MDR-TB treatment. Failure to complete MDR-TB treatment is a significant contributor to poor treatment outcomes and generates further resistance.63 In addition, the pill burden associated with MDR-TB treatment is considerable and the impact of adding further medication has to be considered carefully, weighing risks and benefits.
Patients receiving prolonged NAC had a variety of clinical conditions including respiratory, renal, liver, infectious (HIV and hepatitis C), obstetric and psychiatric diseases. The severity of diseases and the frequency of other comorbidities, including drug and alcohol misuse, were heterogeneous across studies, with some studies including patients with life-threatening conditions such as idiopathic lung fibrosis, systemic sclerosis and end-stage liver disease. The age of included subjects spanned children less than 1 year of age to patients aged over 80 years. Three studies specifically included pregnant women, with a total of 220 receiving NAC. The safe administration of NAC across such a broad spectrum of patients is reassuring when considering its use as adjuvant treatment in patients with MDR-TB. HIV infection, alcohol and drug misuse, and smoking are common in patients with MDR-TB.64–66 Furthermore, a considerable proportion of patients treated for MDR-TB experience depression, or develop hepatic and renal impairment as a result of treatment.67–69 Thus, the safety of any adjunctive therapy needs to be assessed in the context of both the comorbidities and the side effect profile of MDR-TB treatment.
This review was unable to assess potential drug interactions between NAC and drugs used for the treatment of TB. The trials investigating the otoprotective effects of NAC did not report any drug interactions between NAC and aminoglycosides. However, aminoglycosides and NAC were coadministered for a relatively short duration (2–4 weeks) compared with the 8 months of aminoglycoside that is currently recommended for treatment of MDR-TB. Data on interactions between NAC and other anti-TB drugs are lacking, with only one trial conducted in patients on first-line treatment in Iran70; this trial randomised 60 patients being treated with first-line four-drug TB therapy (isoniazid, rifampicin, ethambutol and pyrazinamide) to either receiving 600 mg NAC twice daily for 2 weeks or no additional treatment. The authors hypothesised that NAC would reduce the frequency of drug-induced hepatitis because of its antioxidative properties. The trial reported a significant reduction of alanine aminotransferase and aspartate aminotransferase after 2 weeks of treatment, but drug interactions were not specifically reported.
The strengths of this review include a broad compound search strategy across five different databases and no restrictions with regards to date of publication, language and setting. The safety review included studies administering oral NAC for a minimum of 6 weeks regardless of the disease studied. This permitted the assessment of safety across a broad range of diseases and severity.
This review served to identify a number of important limitations to the existing evidence base. Notably, no studies were identified that investigated the otoprotective potential of NAC in patients receiving aminoglycosides for the treatment of MDR-TB. Furthermore, most studies identified in the safety review failed to provide sufficient information on specific side effects, resulting in a poor quality rating for the purpose of the safety review. The frequency of investigations carried out to assess side effects was only reported in a minority of studies. Thus, the ascertainment of side effects might have been of different quality within and across studies. The review was unable to establish the quality of ascertainment systematically because of lack of information.
Notwithstanding these limitations, the results of this review together with recent findings explaining the mechanism of aminoglycoside-induced ototoxicity and the established antioxidative properties of NAC provide a strong justification for a clinical trial to investigate the effect of concomitant NAC treatment in patients receiving aminoglycosides as part of MDR-TB treatment. The roll-out of the Xpert MTB/RIF (a test to detect TB and rifampicin resistance directly from sputum) in countries with limited laboratory capacity is likely to increase the number of MDR-TB diagnoses and consequently those receiving aminoglycoside therapy, many in areas with limited capacity to monitor ototoxicity.71 While the desired aim for MDR-TB treatment is to develop shortened, more tolerable and aminoglycoside-sparing regimens,72 this may be some way from reality. Published studies of novel combinations are promising.73 Nevertheless, a promising 9-month regimen, piloted in Bangladesh which showed good results in the absence of fluoroquinolone resistance,74 and which is now being evaluated in the STREAM trial, has aminoglycosides as a key part of the regimen.75 While we await the incorporation of bedaquiline and delamanid, two newly registered second-line anti-TB drugs, into recommended second-line treatment regimens, it is likely that aminoglycosides will remain a key pillar of MDR-TB treatment, albeit potentially for shortened periods.75
Acknowledgments
Isatou N'jie and Timo Pilgram from the Knowledge and Library Services, Barts Health NHS trust for helping with retrieval of references.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors WFE, FD and KK conceptualised the idea. KK developed the protocol and conducted the literature searches. KK and WFE screened the titles and abstracts and the full-text manuscripts for eligibility, and performed the data extraction. The meta-analysis was performed by KK and NF. KK wrote the paper with input from WFE, HC, JAS, NF and FD. All authors read and approved the final version of the manuscript.
Funding This study was funded by internal funds (National Mycobacterium Reference Laboratory, Public Health England).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All authors had full access to all data and can take responsibility for the integrity of the data and the accuracy of the data analysis.
Linked Articles
- Airwaves