Article Text

Statistics from Altmetric.com
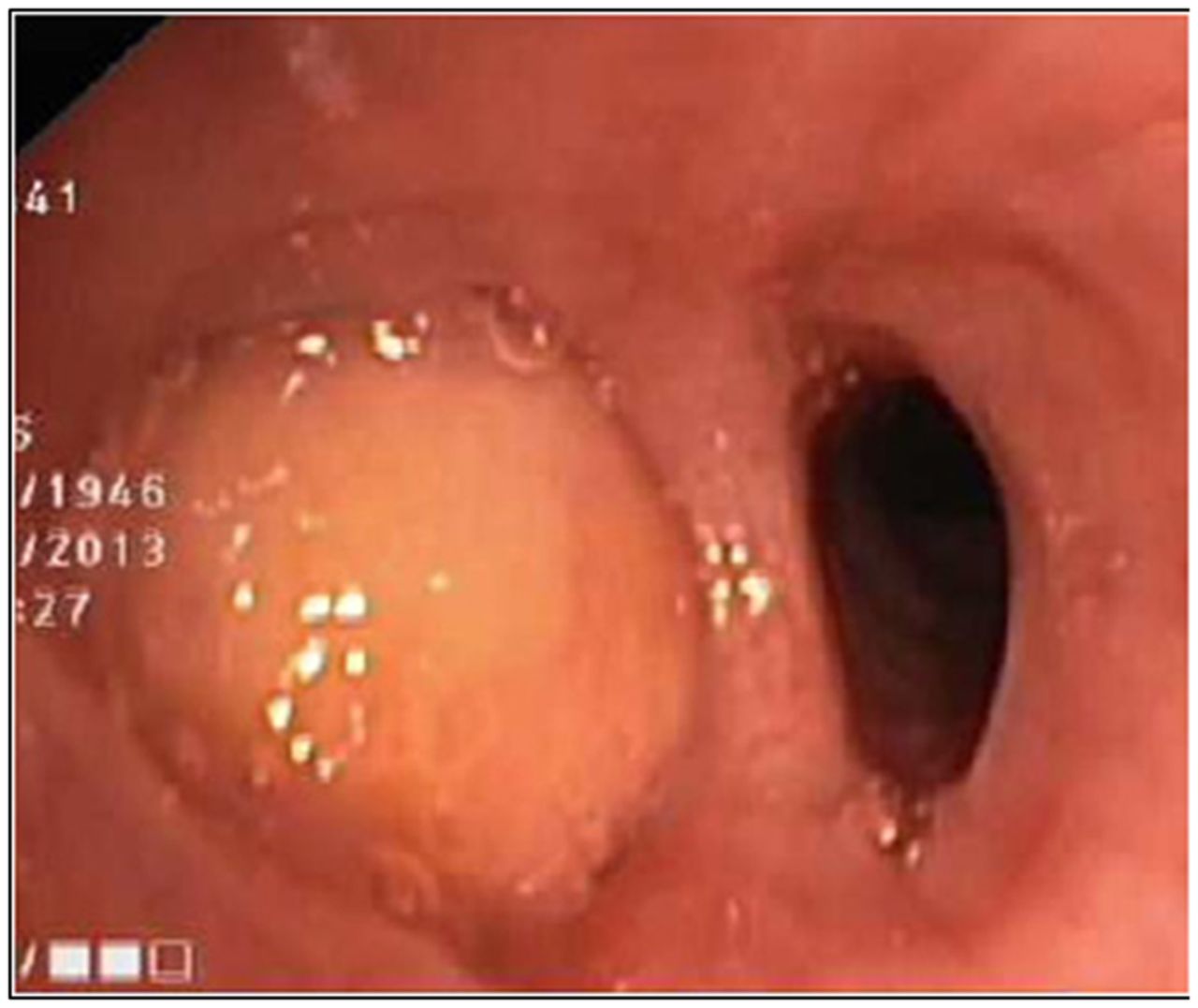
A 68-year-old smoker on aspirin/clopidogrel due to recent percutaneous coronary intervention (PCI) / stenting presented with intermittent haemoptysis. Bronchoscopy revealed an endoluminal tumour in a right-lower-lobe segment (figure 1). No biopsy was taken due to bleeding risk. Aspirate analysis showed sparse cells with granular cytoplasm, and a presumptive diagnosis of bronchial carcinoid was made. CT scan showed no lymphadenopathy. After stopping clopidogrel and absent signs for progression on CT scan/bronchoscopy, right-lower lobectomy was performed. Histological analysis revealed a submucosal lipoma (figure 2).

Bronchoscopic view of a well-circumscribed, yellowish polypoid mass obstructing a segment of the right lower lobe.
{kind=link}
{kind=link}
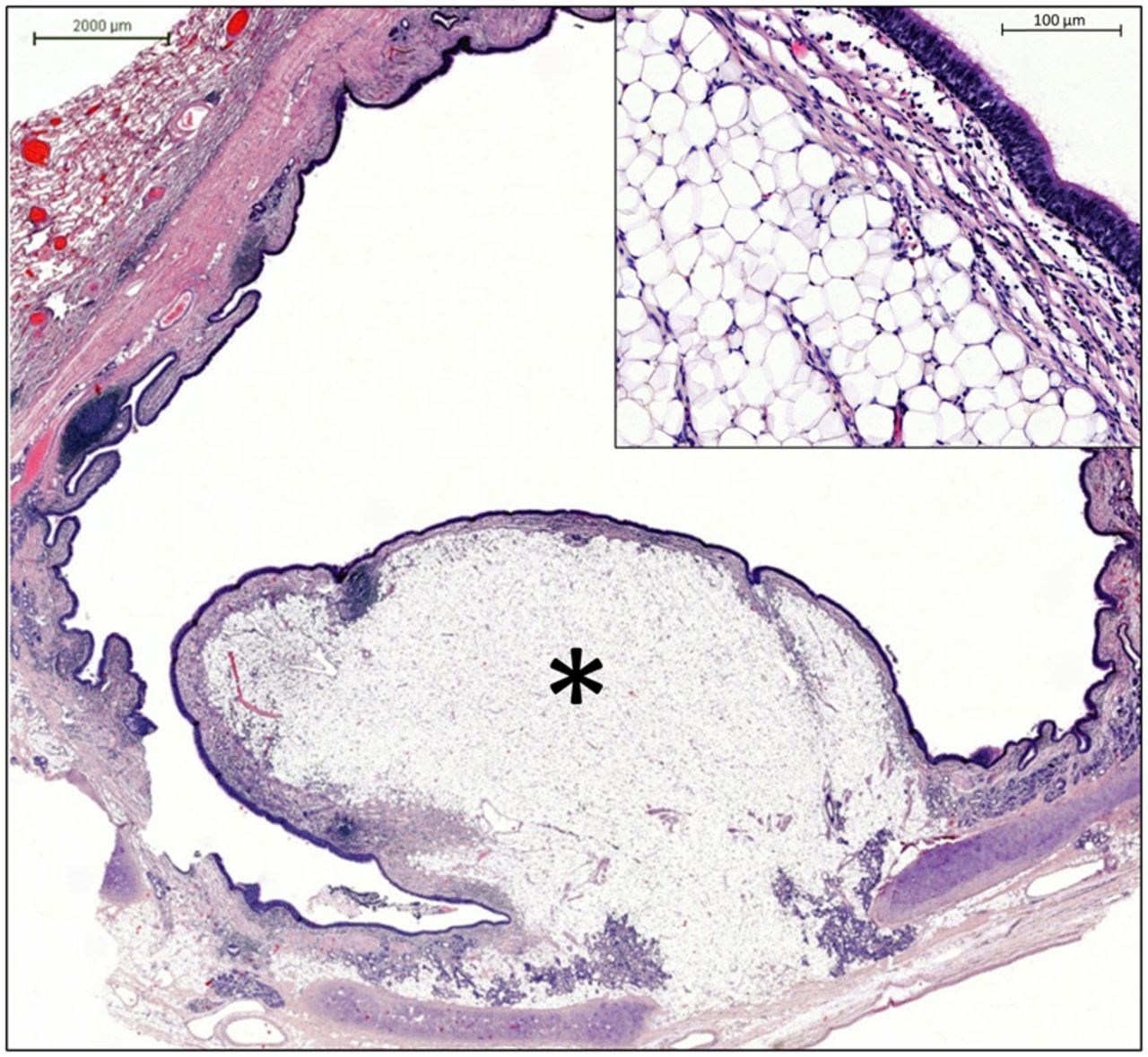
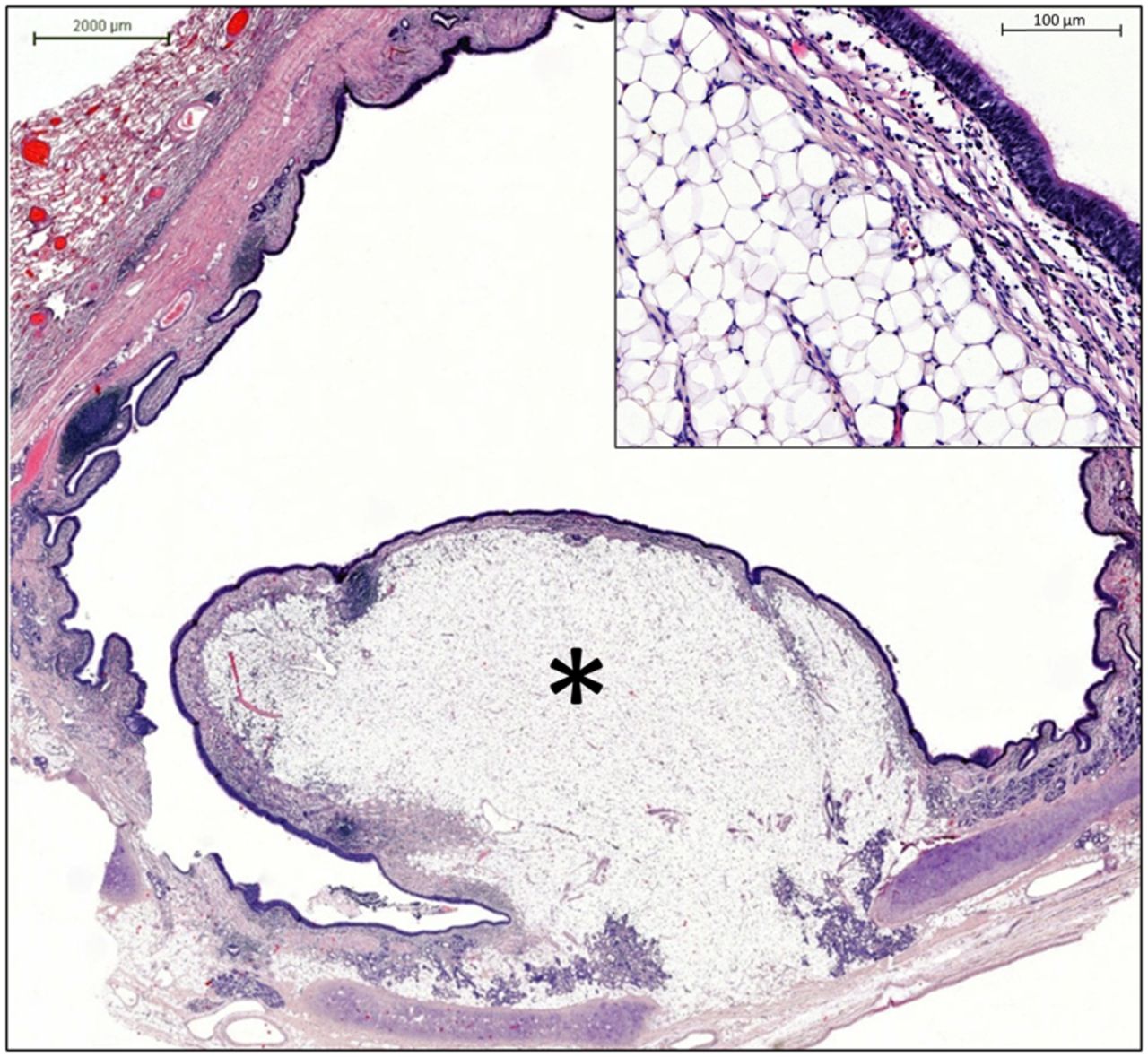
Sagittal section through the bronchus containing the endobronchial tumour (asterisk). The tumour originates from the submucosal layer of the bronchus. Upper edge: magnification of the tumour surface. The tumour is composed of mature fat and covered by respiratory epithelium.
Differential diagnosis of endobronchial tumours encompasses benign (eg hamartoma, lipoma)1 and malignant lesions (eg bronchial carcinoid, metastasis, mucoepidermoid or adenocystic carcinoma).2 Biopsy has to be weighed against bleeding risk especially if a bronchial carcinoid is considered. Retrospectively, a lipoma could have been suspected based on the density of the lesion (−122 HU) and the endoscopic appearance. The management of our case was misled by the cells with granular cytoplasm in the aspirate—arising from a ganglion beside the lipoma—and underlies the importance of a multistep-based diagnostic algorithm.
Footnotes
Contributors YN-O was responsible for data collection and writing the manuscript. FU was responsible for the acquisition of the figures. FR and RT revised the manuscript.
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; internally peer reviewed.
Linked Articles
- Airwaves