Article Text

Abstract
Spirometry is used worldwide to diagnose respiratory disease, and it is a validated measure to assess airway obstruction. Irreversible airway obstruction is the defining feature of chronic obstructive pulmonary disease (COPD). Thus, an FEV1/FVC ratio <70% is used to diagnose COPD, and the severity is thereafter based on the level of FEV1. This definition is widely used in clinical practice and research, yet may lead to confusion with respect to the diagnosis associated with the presence of airway obstruction. The three main reasons are the following: (1) fixed airflow obstruction may be the result of specific diagnoses such as cystic fibrosis; (2) FEV1/FVC ratio changes with ageing, and it is therefore inappropriate to use the same ratio at 40 and 90 years, leaving aside gender differences; (3) even when specific diagnoses are excluded, fixed airflow obstruction may be the end-stage of many different underlying processes. The authors believe that they have strong arguments that a COPD diagnosis based solely on spirometric values is nonsense. More sophisticated lung function tests, such as plethysmography, forced oscillation and lung clearance index, may help further to delineate the characteristics of low lung function. However, these are not feasible in most clinical contexts and in epidemiologic studies. Therefore, the authors throw down the gauntlet: spirometry is an essential tool in patient evaluation but dangerous for disease diagnosis, and the term COPD should only be used in the appropriate clinical (diagnostic) context.
- COPD
- umbrella
- asthma
- spirometry
- diagnosis
- COPD mechanisms
- lung physiology
- asthma
- COPD epidemiology
- COPD exacerbations
- COPD pathology
- COPD pharmacology
- emphysema
- lung proteases
- pulmonary embolism
- tobacco and the lung
- asthma guidelines
- cystic fibrosis
- exhaled airway markers
- lung physiology
- paediatric asthma
- paediatric lung disease
- allergic lung disease
- asthma
- asthma genetics
Statistics from Altmetric.com
- COPD
- umbrella
- asthma
- spirometry
- diagnosis
- COPD mechanisms
- lung physiology
- asthma
- COPD epidemiology
- COPD exacerbations
- COPD pathology
- COPD pharmacology
- emphysema
- lung proteases
- pulmonary embolism
- tobacco and the lung
- asthma guidelines
- cystic fibrosis
- exhaled airway markers
- lung physiology
- paediatric asthma
- paediatric lung disease
- allergic lung disease
- asthma
- asthma genetics
Key messages
What is the key question?
What is the use of irreversible airway obstruction for a chronic obstructive pulmonary disease diagnosis?
What is the bottom line?
Spirometry is an essential tool in patient evaluation but dangerous for disease diagnosis, and the term chronic obstructive pulmonary disease should only be used in the appropriate clinical (diagnostic) context.
Why read on?
Spirometry is being used for disease diagnosis, but is this a valid tool?
Opinion
Spirometry is used worldwide to diagnose respiratory disease, and it is a validated measure to assess airway obstruction.1 Irreversible airway obstruction is the defining feature of chronic obstructive pulmonary disease (COPD). Thus, an FEV1/FVC ratio <70% is used to diagnose COPD, and the severity is thereafter based on the level of FEV1.2 This definition is widely used in clinical practice and research, yet may lead to confusion with respect to the diagnosis associated with the presence of airway obstruction. The three main reasons are the following: (1) fixed airflow obstruction may be the result of specific diagnoses such as cystic fibrosis (CF)3; (2) FEV1/FVC ratio changes with ageing, and it is therefore inappropriate to use the same ratio at 40 and 90 years, leaving aside gender differences4 5; and (3) even when specific diagnoses are excluded, fixed airflow obstruction may be the end-stage of many different underlying processes.6 We believe that we have strong arguments that a COPD diagnosis based solely on spirometric values is nonsense.
With regard to diagnosis, fixed airflow obstruction is a feature of many diseases, such as CF, primary ciliary dyskinesia and non-CF bronchiectasis.3 Children with CF died young in the past but may live in this era into middle age and beyond as a result of earlier disease diagnosis and better treatment options being available. They develop airway obstruction with advanced disease frequently comparable with the spirometric values found in COPD.7 Does this then mean that patients with CF develop COPD if they live long enough? Does this imply that doctors should change from CF to COPD treatment protocols? Rightly, as clinicians, we do not do this. The more surprising is that this is what we seem to do to patients with asthma. When an adult patient with lifelong asthma comes into a hospital to be treated for an asthma lung attack,8 the patient may be discharged with a diagnosis of COPD because irreversible airway obstruction is present, yet this has been shown not only to occur in COPD but in long-standing asthma as well.5 9 This is important because patients with asthma need not only long-acting bronchodilators but also inhaled steroids, the mainstay of asthma treatment. Thus, this change in diagnosis, particularly when the level of FEV1 is above the 50% predicted, may not serve these patients well.
In addition, there exists ‘non-smoking’ COPD that is attributed to biomass fuel exposure.10 One can assume that this will not have the same patterns of inflammation as COPD in smokers. There has been much speculation that the survivors of premature birth and bronchopulmonary dysplasia may be at risk for COPD, but such evidence as exists is that they do not have airway inflammation.11 Thus, treatment strategies trialled in patients with ‘smoking COPD’ may be inappropriate in other forms of persistent airflow obstruction.
The above is also important in studies assessing the genetic background of lung function loss, using FEV1 as a single endpoint for analysis. The degree of airway obstruction at birth is determined by in utero processes, and lung function can be compromised at birth, for example, in low birth weight babies or children whose mothers smoked in pregnancy.12 This then tracks throughout life, resulting in a lower plateau at approximately 20–25 years of age and lower levels of FEV1 with further ageing. It is likely that the genetic mechanisms underlying low lung function due to the in utero environment affecting the developmental stage of the lung are completely different from those in individuals with similar spirometry starting with normal weight and lung function at birth and having 40 pack-years of smoking in later life. Thus, by pooling all individuals with low FEV1 for genetic analyses, significant results may be missed. This may well be one reason why it has proved difficult to identify genes that increase susceptibility to COPD defined on spirometric criteria alone. Indeed, recent candidate gene and genome-wide studies of lung function have shown that a number of genes that are associated with spirometry in adult life are also associated with lung function in childhood, highlighting the key role of early life lung function growth13 14 in low FEV1/FVC ratios in some patients (as opposed to smoking or other exposures in adulthood).
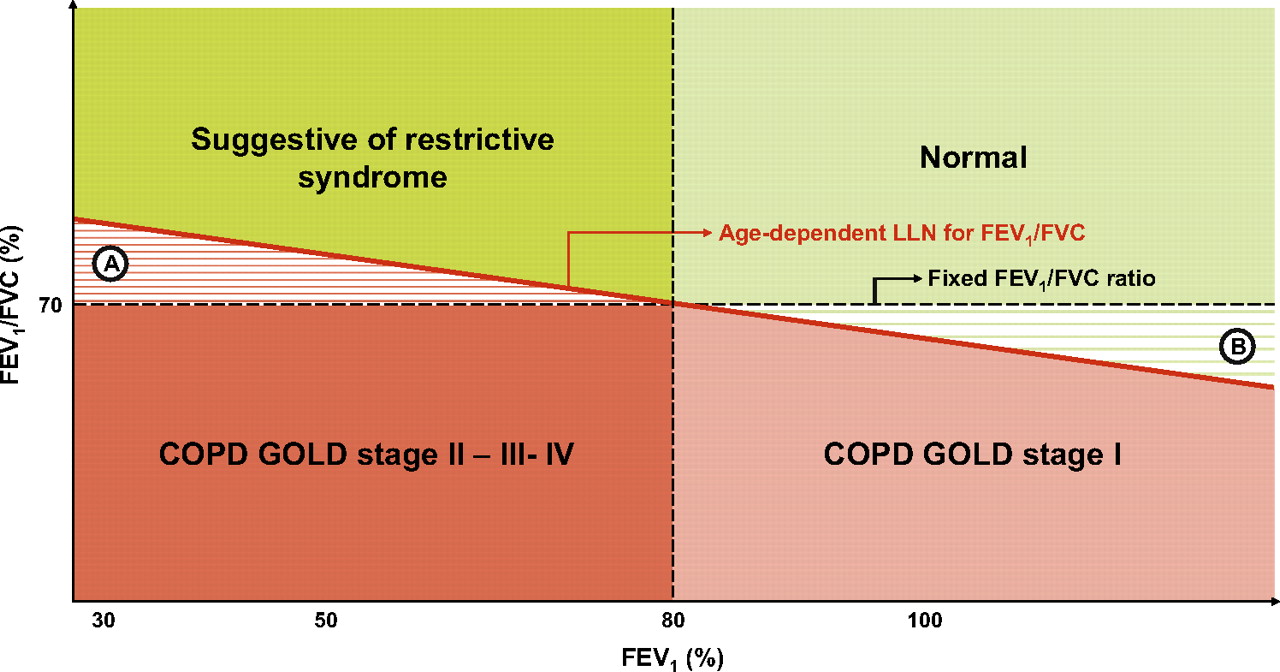
Adding to the confusion is the current use of the term Global Initiative for Obstructive Lung Disease Unclassified in adults with an FEV1/FVC ratio >0.70 but FEV1 <80% predicted (figure 1).15 Only a small subgroup of the—especially younger—subjects in this Global Initiative for Obstructive Lung Disease Unclassified category have airway obstruction based on an FEV1/FVC ratio < lower limit of normal.4 5 Most, however, have suggestive evidence of restrictive lung function disturbance, clearly needing confirmation by additional lung function tests.

{kind=link}
Simplified scheme of classification of individuals based upon FEV1 and FEV1/FVC ratio. Only in the appropriate clinical context, subjects with a post-bronchodilator FEV1/FVC <70% (Global Initiative for Obstructive Lung Disease (GOLD)) or < lower limit of normal, can be diagnosed with COPD (GOLD stage I if FEV1 >80%; GOLD stage II, III or IV if FEV1 <80%, <50% or <30%, respectively).
In summary, low FEV1/FVC ratios in adult life can be caused by many different diseases, such as bronchopulmonary dysplasia, asthma, COPD and CF. Moreover, the level of lung function can be compromised by preterm birth, low birth weight, passive smoke exposure in utero or early life, air pollution, viral infections and many other unknown factors.
Therefore, we propose that the term COPD should not be used because it is no more diagnostically precise than, for example, chronic renal failure. Instead, we should describe what we see, namely, low lung function and then define the associate characteristics after optimal bronchodilation (oral corticosteroid course and bronchodilators), that is:
irreversible airway obstruction associated with long-standing asthma;
irreversible airway obstruction with a strong history of smoking;
irreversible airway obstruction compatible with previous low birth weight.
Obviously, more sophisticated lung function tests, such as plethysmography, forced oscillation and lung clearance index, may help further to delineate the characteristics of low lung function. However, these are not feasible in most clinical contexts and in epidemiologic studies. Therefore, we throw down the gauntlet: spirometry is an essential tool in patient evaluation but dangerous for disease diagnosis, and the term COPD should only be used in the appropriate clinical (diagnostic) context.
References
Footnotes
Linked article 200584
Competing interests None.
Provenance and peer review Not commissioned; internally peer reviewed.