Article Text

Abstract
Interstitial lung abnormalities (ILA) can be incidentally detected in patients undergoing low-dose CT screening for lung cancer. In this retrospective study, we explore the downstream impact of ILA detection on interstitial lung disease (ILD) diagnosis and treatment. Using a targeted approach in a lung cancer screening programme, the rate of de novo ILD diagnosis was 1.5%. The extent of abnormality on CT and severity of lung function impairment, but not symptoms were the most important factors in differentiating ILA from ILD. Disease modifying therapies were commenced in 39% of ILD cases, the majority being antifibrotic therapy for idiopathic pulmonary fibrosis.
- Idiopathic pulmonary fibrosis
- Interstitial Fibrosis
- Lung Cancer
Statistics from Altmetric.com
Introduction
Early detection and treatment of lung cancer through low-dose CT (LDCT) screening reduces mortality.1 Interstitial lung abnormalities (ILA), incidentally detected CT scan findings potentially compatible with interstitial lung disease (ILD), are found in 4%–9% of older smokers undergoing LDCT screening.2 ILA can progress3 and have been associated with increased mortality.2 Differentiating ILA from ILD requires integration of clinical domains, physiology and CT features through multidisciplinary team (MDT) discussion. Studies have reported the prevalence and progression of ILA identified through lung cancer screening programmes,3 4 but few have investigated the impact on patient care. Here, we report new ILD diagnoses and treatments initiated following proactive identification and evaluation of patients referred from a targeted lung screening programme.
Methods
This retrospective study was conducted at the Royal Brompton Hospital between August 2018 and April 2021 through the West London lung cancer screening pilot.5 Ever-smokers aged 55–75 years were invited to a lung health check and offered LDCT if they met prespecified lung cancer risk scores,6 7 in line with NHS England protocols.8 Eligible participants underwent a baseline scan and were reinvited for a further “incident” scan 18–24 months later if the baseline scan was negative for lung cancer. Diagnoses were assigned following ILD MDT discussion.
Results
1853 subjects underwent LDCT screening. ILA >5% extent on CT were identified in 78/1853 (4.2%) of the cohort. 59 subjects (3.2%) with ILA fulfilled prespecified criteria for specialist ILD evaluation8 (figure 1). Fourty-three subjects (2.3%) underwent ILD assessment (table 1). Mean age was 68.8 years; 27/43 (63%) subjects were men. Cough and/or dyspnoea was reported by 23/43 (53.5%) subjects. Physical examination was performed in 21/43 (48.8%) subjects. Crackles were auscultated in 17/21 (80.9%) subjects examined. Mean forced vital capacity (FVC) was 89.5% SD:14.2% using Global Lung Function Initiative reference ranges with mean lung diffusing capacity for carbon monoxide (DLco) 63.6% SD:14.0%. Diagnostic bronchoalveolar lavage was performed in 8/43 (18.6%) subjects; lymphocytosis ≥20% was demonstrated in two cases, and pigment-laden macrophages in one case. Transbronchial lung cryobiopsy demonstrated non-necrotising granulomatous inflammation in one individual.

Case identification through LDCT screening. *Lung function testing ceased between March and November 2020 due to COVID-19 restrictions. ILA, interstitial lung abnormalities; ILD, interstitial lung disease; LDCT, low-dose CT.
Clinical characteristics of LDCT-screened subjects referred for ILD evaluation
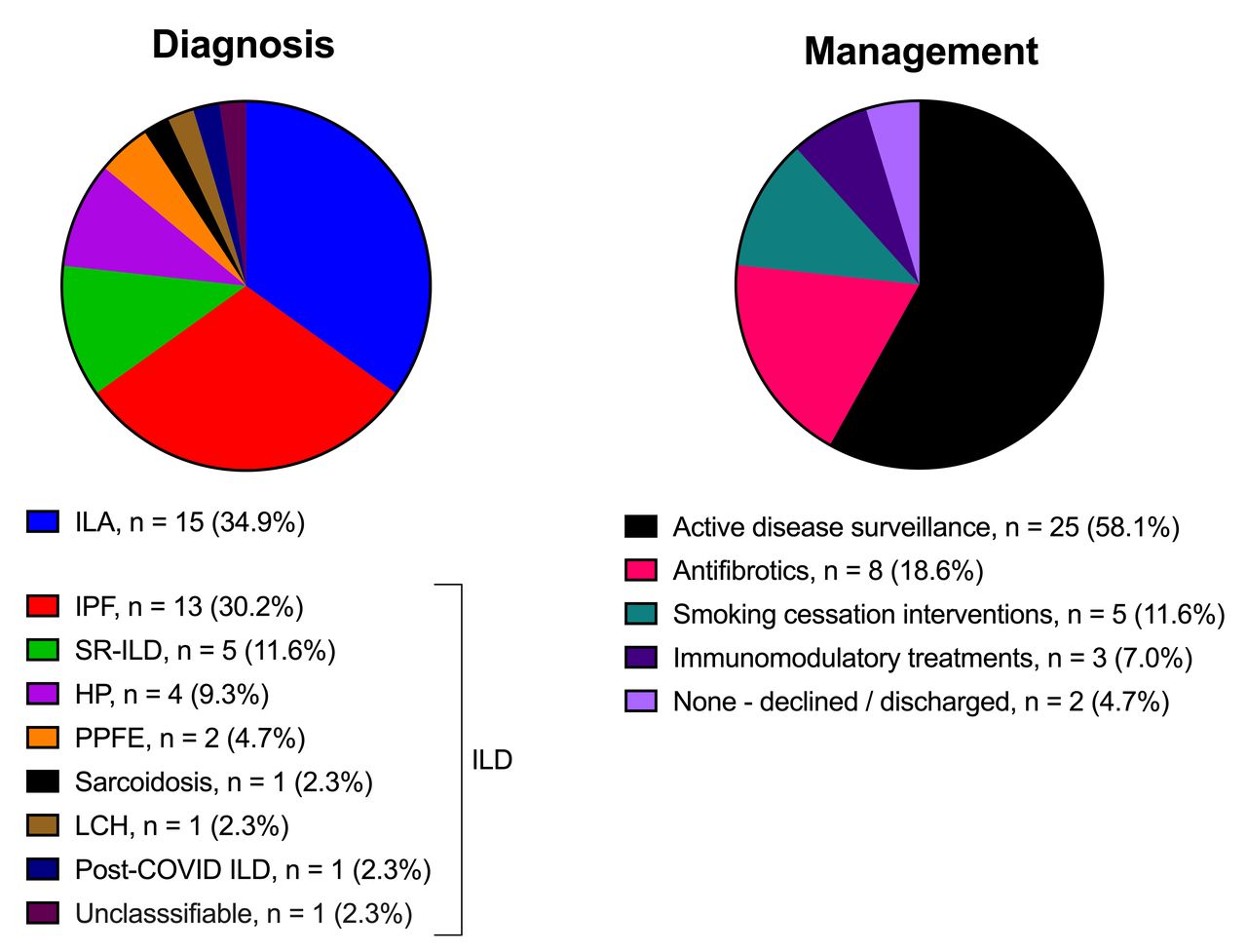
ILD was diagnosed in 28/43 (65.1%) subjects assessed (1.5% (95% CI 1.04 to 2.18) of the LDCT cohort), with the remaining 15/43 (34.9%) categorised as ILA. The most common ILD was idiopathic pulmonary fibrosis (IPF), diagnosed in 13/43 (30.2%) of subjects assessed (0.7% of the entire cohort). Other diagnoses are detailed in figure 2. Pirfenidone or nintedanib for IPF was commenced in 8/43 (18.6%) subjects who met the UK National Institute for Health and Care Excellence criteria with an FVC between 50% and 80% (figure 2). Immunomodulatory treatments were initiated in three patients; prednisolone for two cases of hypersensitivity pneumonitis, prednisolone and methotrexate for one patient with sarcoidosis.
{kind=link}
{kind=link}
Diagnosis and management of ILD detected through LDCT screening. HP, hypersensitivity pneumonitis; ILA, interstitial lung abnormalities; ILD, interstitial lung disease; IPF, idiopathic pulmonary fibrosis; LCH, Langerhans cell histiocytosis; LDCT, low-dose CT; PPFE, pleuroparenchymal fibroelastoses; SR-ILD, smoking-related ILD.
There were no significant differences in age, gender or smoking pack-years between participants with a final MDT diagnosis of ILD versus ILA. Individuals diagnosed with ILD had a greater extent of abnormality on CT; ≥10% extent ILA was reported in 89.3% of individuals with ILD compared with 46.7% of those with ILA. Respiratory symptoms were more frequently reported in the ILA group compared with the ILD group; 73.3% versus 42.9% potentially reflective of the comorbid nature of this population. Mean DLco was reduced in those diagnosed with ILD (60.4 SD: 12.6% (p=0.04)) and specifically, IPF (54.0 SD: 9.3% (p=0.003)) compared with ILA (69.4 SD: 15.9%). Mean FVC was lower in those with ILD (86.7 SD:13% (p=0.08)) and in IPF (85.7 SD: 10.1% (p=0.09)) compared with ILA (94.7 SD: 15.5%).
Discussion
1.51% of LDCT-screened subjects meeting prespecified criteria were newly diagnosed with ILD of which almost half had IPF. In the same screening programme, lung cancer was detected in 2.5%.5 In the NELSON trial, suspicious nodules were detected in 2.1% of CT scans, leading to lung cancer diagnosis in 0.9% of screened participants.1 The incidence of ILD is, therefore, comparable with that of lung cancer in this selected demographic. Outcomes with IPF are comparable to that of lung cancer and early intervention with antifibrotic therapy improves life expectancy.9 For other forms of ILD, close monitoring and early immunosuppression can reduce the risk of irreversible lung fibrosis.10 Furthermore, a proportion of patients diagnosed with ILA, initially monitored without treatment, are eventually diagnosed with IPF during follow-up. Lung cancer screening, therefore, provides an opportunity to detect and treat ILD early, potentially improving patient outcomes.
Diagnostic delays for patients with ILD are common. Half of participants referred for ILD evaluation reported respiratory symptoms and most had an abnormal physical examination. ILD should always be considered in patients with respiratory symptoms and crackles on lung auscultation. In our cohort, spirometry was within normal ranges, although lower in patients with ILD than ILA, but gas transfer was frequently reduced—laboratory lung function testing is therefore required in the comprehensive evaluation of these patients.
There were limitations to this study. The final cohort diagnosed with ILD through LDCT screening was derived from one region of the UK. ILD diagnoses were derived from a pre-selected population at high risk of lung cancer and excluded non-smokers and younger individuals who may also have occult ILD. Clinical examination and lung function data were incomplete due to COVID-19 restrictions. Sixteen subjects had not completed their diagnostic work-up and so the final ILD rate reported here may be an underestimate.
In conclusion, we demonstrate that at least 1.5% of participants attending for lung cancer screening have undiagnosed ILD. Pragmatic CT and spirometry referral criteria have the potential to expedite diagnoses of ILD without overwhelming specialist services. The degree of CT abnormality and lung function impairment but not symptoms were the most important factors in differentiating between ILA and ILD at MDT. IPF was highly represented in this high-risk cohort and 19% of all patients referred for evaluation were initiated on antifibrotic therapy, an intervention known to improve patient outcomes. This study demonstrates the value of targeted ILD case-finding in lung cancer screening programmes but requires confirmation across other screening populations and ILD centres. The resource utilisation and cost-effectiveness of this approach across international healthcare settings warrants further detailed evaluation.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants but was not approved by Ethics Committee or Institutional Board approval not required as this was a service evaluation study. Participants gave informed consent to participate in the study before taking part.
Footnotes
Twitter @RichardJHewitt, @DrPeteGeorge
Correction notice This article has been corrected since it was published Online First. The funding statement has been amended.
Contributors Study design: PMG, AD, RJH, ECB. Data acquisition: RJH, ECB, RG, HB, PMG, AD. Analysis, interpretation, manuscript drafting and revision and final approval of manuscript: RJH, ECB, RG, HB, VK, FC, MK, PLM, SRD, AUW, GJ, EAR, SVK, AD, PMG.
Funding RJH is supported by a NHLI funded Clinical Lectureship. The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests All authors have completed the ICMJE COI disclosure form and declare no support from any organisation for the submitted work. ECB, RG, HB, FC, MK, SVK report no competing interests. RJH reports participation in Boehringer Ingelheim educational events. VK reports speaker fees from Boehringer Ingelheim, Novartis, Roche. PLM reports grants from AstraZeneca, consulting fees from Hoffman-La Roche, Boehringer Ingelheim, AstraZeneca and speaker fees from Boehringer Ingelheim, Hoffman-La Roche. SRD reports consulting fees from Boehringer Ingelheim, Astra-Zeneca; participation on a data safety monitoring board for Astra-Zeneca. AUW reports consulting fees and speaker fees from Boehringer Ingelheim, Roche, and participation on a data safety monitoring or advisory board for Veracyte. RGJ reports grants from Astra Zeneca, Biogen, Galecto (all paid to institution); grants from GlaxoSmithKline, Nordic Biosciences, RedX, Pliant; consulting fees from Bristol Myers Squibb, Chiesi, Daewoong, Resolution Therapeutics, Pliant, Veracyte; speaker fees from Boehringer Ingelheim, Chiesi, Roche, PatientMPower, AztraZeneca; participation on a data safety monitoring board for Boehringer Ingelheim, Galapagos, Vicore; and is the President of Action for Pulmonary Fibrosis. EAR reports a grant, consulting fees and speaker fees from Boehringer Ingelheim (paid to institution); speaker fees from Roche and Chiesi (paid to institution); support to attend the ATS conference from Boehringer Ingelheim. AD reports consulting fees from Boehringer Ingelheim, Roche, Brainomix, Galapagos, Galecto, Vicore. PMG reports grants from Boehringer Ingelheim, MRC, Imperial College BRC; consulting fees from Boehringer Ingelheim, AstraZeneca; speaker fees from Boehringer Ingelheim, Roche, Cipla; support to attend the ATS and ERS from Boehringer Ingelheim and Roche; and is Medical Director of Brainomix LTD Stock options.
Provenance and peer review Not commissioned; externally peer reviewed.