Article Text

Abstract
This review aims to: (1) describe the rationale of pleural (PPL) and transpulmonary (PL) pressure measurements in children during mechanical ventilation (MV); (2) discuss its usefulness and limitations as a guide for protective MV; (3) propose future directions for paediatric research. We conducted a scoping review on PL in critically ill children using PubMed and Embase search engines. We included peer-reviewed studies using oesophageal (PES) and PL measurements in the paediatric intensive care unit (PICU) published until September 2021, and excluded studies in neonates and patients treated with non-invasive ventilation. PL corresponds to the difference between airway pressure and PPL. Oesophageal manometry allows measurement of PES, a good surrogate of PPL, to estimate PL directly at the bedside. Lung stress is the PL, while strain corresponds to the lung deformation induced by the changing volume during insufflation. Lung stress and strain are the main determinants of MV-related injuries with PL and PPL being key components. PL-targeted therapies allow tailoring of MV: (1) Positive end-expiratory pressure (PEEP) titration based on end-expiratory PL (direct measurement) may be used to avoid lung collapse in the lung surrounding the oesophagus. The clinical benefit of such strategy has not been demonstrated yet. This approach should consider the degree of recruitable lung, and may be limited to patients in which PEEP is set to achieve an end-expiratory PL value close to zero; (2) Protective ventilation based on end-inspiratory PL (derived from the ratio of lung and respiratory system elastances), might be used to limit overdistention and volutrauma by targeting lung stress values < 20–25 cmH2O; (3) PPL may be set to target a physiological respiratory effort in order to avoid both self-induced lung injury and ventilator-induced diaphragm dysfunction; (4) PPL or PL measurements may contribute to a better understanding of cardiopulmonary interactions. The growing cardiorespiratory system makes children theoretically more susceptible to atelectrauma, myotrauma and right ventricle failure. In children with acute respiratory distress, PPL and PL measurements may help to characterise how changes in PEEP affect PPL and potentially haemodynamics. In the PICU, PPL measurement to estimate respiratory effort is useful during weaning and ventilator liberation. Finally, the use of PPL tracings may improve the detection of patient ventilator asynchronies, which are frequent in children. Despite these numerous theoritcal benefits in children, PES measurement is rarely performed in routine paediatric practice. While the lack of robust clincal data partially explains this observation, important limitations of the existing methods to estimate PPL in children, such as their invasiveness and technical limitations, associated with the lack of reference values for lung and chest wall elastances may also play a role. PPL and PL monitoring have numerous potential clinical applications in the PICU to tailor protective MV, but its usefulness is counterbalanced by technical limitations. Paediatric evidence seems currently too weak to consider oesophageal manometry as a routine respiratory monitoring. The development and validation of a noninvasive estimation of PL and multimodal respiratory monitoring may be worth to be evaluated in the future.
- ARDS
- Critical Care
- Paediatric Physician
- Respiratory Measurement
Statistics from Altmetric.com
Introduction
Acute respiratory failure is one of the leading causes of admission to the paediatric intensive care unit (PICU).1 Although life-saving, mechanical ventilation (MV) may induce lung injury,2 diaphragm dysfunction3 and/or haemodynamic instability.4–6 Research during the last decades has aimed to optimise MV to limit deleterious effects. This concept of ‘protective’ ventilation has historically focused on the lung, but more recent strategies recognise the importance of also protecting the diaphragm.7
A number of techniques have been developed to deliver protective MV.8 9 In particular, oesophageal manometry allows for the estimation of pleural pressure (PPL) and the calculation of transpulmonary pressure (PL), which has important implications to understand how to best protect both the lung and the diaphragm. There have been a number of studies, including clinical trials, using P L in adults,10 but there are few paediatric studies. The aim of this review is: (1) to describe the physiological and clinical rationale of PPL and PL measurements in children during MV; (2) to discuss its usefulness and limitations as a guide for protective MV; (3) and to propose future directions for research in paediatrics.
Methods
We conducted a review of the medical literature on PPL and PL measurements in critically ill children. Detailed methodology is presented in online supplemental file.
Supplemental material
Physiological rationale for the measurement of transpulmonary pressure (PL)
Physiology of spontaneous and mechanically assisted breathing
Work of breathing corresponds to the energy generated by the respiratory system for the breathing process. During spontaneous breathing (SB), the pressure produced by the inspiratory muscles (PMUS) leads to a decrease of PPL and chest expansion, which in turn results in lung expansion, decrease of intra-alveolar pressure and air intake. During invasive MV, the ventilator partially (« assisted ») or totally (« controlled » ventilation) substitutes for the patient’s respiratory muscles, providing positive intrathoracic pressure (PAW) that allows chest expansion. The patient’s respiratory muscles and/or the ventilator have to overcome the load imposed by the structures of the respiratory system (conducting airways, lung parenchyma, chest wall), each of which has its own resistive and elastic properties. The total pressure generated by the respiratory system (PTOT) during a breathing cycle is used to overcome the resistance in the airways as well as expand the lung and chest wall. This relationship is depicted in the equation of motion (figure 1). This equation can be applied during static conditions (without airflow) to consider the elastic pressures required to move the tidal volume within the respiratory system, which includes both the pressure required to expand the chest wall (PCW, computed as the difference between PPL and atmospheric pressure) and the transpulmonary pressure (PL, computed as the difference between end-inspiratory alveolar pressure and PPL) (figure 1). The PL represents the real distending pressure accross the alveoli, and is the most precise marker of lung stress.

Schematic representation of the relationship between structures within the respiratory system. According to the equation of motion of the respiratory system. PTOT=PAW + PMUS (1). PTOT = P0+ERS*V+RRS*V’ (2). since PRS=PL + PCW, ERS=EL + ECW and the final equation can be written as. pAW +PMUS = P0+ECW*V+EL*V+RRS*V’ (3). ECW, chest wall elastance; EL, lung elastance; ERS, respiratory system elastance; PATM, atmospheric pressure; PAW, airways pressure; P0, pAW at the beginning of the ventilatory cycle; PCW, pressure difference across the chest wall; PL, transpulmonary pressure; PMUS, respiratory muscles’ generated-pressure; PPL, pleural pressure; PRS, pressure difference across the respiratory system; PTOT, total pressure applied to the respiratory system; V, air volume; V’, airflow.
PL and PPL to characterise overdistention
Stress and strain are important concepts to deliver protective ventilation. Lung stress is the PL, while strain corresponds to the change in lung size relative to its original size (ie, tidal volume/functional residual capacity (FRC)). Stress and strain are related to one another based on the specific elastance of the lung.11 Lung strain is high when the delivered tidal volume is high relative to the size of the lung at end-expiration. For this reason, low tidal volume strategies are most important for patients who have the largest reduction in FRC (ie, severe acute respiratory distress syndrome (ARDS)). Lung stress is high when the end-inspiratory PL is elevated, which is a function of the lung elastance and tidal volume. In routine clinical practice, lung stress is estimated by measuring the plateau pressure (PPLAT) (PAW measured at the end of an inspiratory occlusion) (figure 1), or the driving pressure (∆P) (plateau pressure minus positive end-expiratory pressure, PEEP),12 13 the later of which has been shown to be associated with mortality in ARDS.14 However, it is important to remember that both PPLAT and ∆P reflect both lung and chest wall components. Therefore, they are not precise measures of lung stress because they do not adjust for the pressure used to move the chest wall. For this, one must measure (or estimate) PPL.
Stress and strain on the lung may occur even in the absence of positive pressure ventilation, when patients have vigorous effort with injured lungs, a phenomenon deemed self-induced lung injury (P-SILI).15 Here large negative swings in PPL are generated by the patient, which may result in high PL (stress) as well as high tidal volume from high respiratory drive (strain), and may decrease alveolar pressure.16 Furthermore, there are important regional differences in the distribution of ventilation, and the ‘pendelluft’ phenomenon during strenuous efforts causes high PPL swings in the dependent (dorsal) lung, generating local stress and volutrauma by deviating gas from the non-dependent (ventral) regions.17
PL and PPL to titrate PEEP
In addition to characterising the risk of lung stress, PPL may also be useful to prevent atelectrauma. The end-expiratory PPL is a marker of the pressure the chest wall exerts at end expiration. It may be theoretically advantageous to titrate PEEP such that the end-expiratory PL (PEEP- PPL) is above zero. This may ensure that increases in PPL from poorly compliant chest walls are overcome with PEEP, such as observed in obese patients18 or in patients with intra-abdominal hypertension.19 In adults, several studies have shown some advantages of PEEP titration based on PL instead of oxygenation,20 21 but the only multicentric randomised controlled trial (RCT) published to date failed to demonstrate that a PL-targeted strategy improved outcomes over an empiric high-PEEP approach from the ARDSNet High-PEEP FiO2 table.22 Notably, in both groups, PEEP-PL was on average greater than zero, highlighting that for the entire population targeted therapy PL may not be better than an empiric high PEEP approach based on oxygenation. However, PEEP management must consider the degree of recruitable lung, and secondary analysis on this RCT demonstrated that patients who achieved a PL close to zero appeared to have the best outcomes.23
PL and PPL to understand patient effort, patient ventilator asynchrony and cardiopulmonary interactions
PPL or PL estimations may also be helpful to prevent ventilator-induced diaphragmatic dysfunction (VIDD). VIDD has been reported in children.24–26 Mechanisms underlying VIDD comprise ventilatory overassistance leading to low levels of inspiratory effort which may induce muscle atrophy,25 27 28 and patient-ventilator asynchrony (PVA), which in turn may lead to excessive/eccentric activity of the diaphragm.29 PPLestimates may afford titration of ventilator settings to maintain patient effort of breathing within a physiologic range, allow a better identification of PVA,30–32 and prevent muscle atrophy.33 Diaphragm atrophy is associated with a poor outcome.3 34 Estimation of patient effort using the PPL swings (such as with oesophageal manometry) may thus be an important tool to identify patients at high risk for P-SILI and VIDD.8 However, the optimal level of patient inspiratory effort remains unknown, although therapeutic targets have been suggested.29 35
Finally, the analysis of PPL and PL variations during MV may be important to better understand cardiopulmonary interactions. Right ventricle systolic failure (RVF) is a frequent complication of MV, especially in patients with significant hypoxaemia and ARDS.5 PPL is often increased, which can reduce systemic venous return and right ventricle (RV) preload,36 and the rise in PL increases pulmonary vascular resistances and RV afterload.4 6 Strategies including high levels of PEEP and recruitment manoeuvres may induce RVF,37 circulatory failure and death.38 Direct measurement of PL and PPL may characterise the impact of the lung distention on RV function to improve protective ventilation.
Rationale for the measurement of PL and PPL in children
Table 1 summarises the physiological rationale and the clinical applications for PPL and PL monitoring in mechanically ventilated children.
Summary of the rationale and clinical applications for PL and PPL monitoring in critically ill children undergoing invasive mechanical ventilation
Paediatric physiological specificities
There are important developmental and physiological differences between children and adults which may underscore different responses to ‘injurious’ MV. Children represent a diverse and heterogeneous population in terms of age and weight, diseases and respiratory mechanics, especially in neonates and infants. The respiratory and cardiovascular system of children is constantly evolving from infancy (under 1 year) to adolescence. In reality, there are few randomised controlled trials in children, although the physiological principles embraced by protective ventilation strategies are generally applicable to this population.
Infants have a low FRC and a more compliant chest wall, which may favour lung retraction and atelectasia.39 Inspiratory tidal volume is limited by the horizontal shape of the ribs and diaphragm, whose immature musculature increases the risk of fatigability.40 Due to these specific physiological features, infants are highly susceptible to dynamic hyperinflation during respiratory distress, in order to maintain end-expiratory lung volume. Diaphragm activation during expiration is common in young children under MV,41 42 which may promote fatigability and contribute to VIDD. Because of their small tidal volume, their high respiratory rate, and their highly variable breathing pattern, patient-ventilator synchrony is challenging in children, especially infants. In the infant’s lung, the lung volume induced by MV is associated with an increase in elastin concentrations and a decrease in collagen concentrations in greater proportions than in adults,43 increasing the risk of lung stress and strain.11 Conversely, high tidal volume generates more surfactant production as compared with adults, and the immaturity of the immune system directs the innate immune response towards the production of antiinflammatory cytokines.44 This may moderately protect the paediatric lung from the effects of high tidal volume. Nevertheless, ventilator-induced lung injury (VILI) has been well recognised in young animals45 and in clinical studies, although specific targets for lung-protective ventilation strategies from adults may not directly translate to children. Furthermore, pressure limited modes are more frequently used in children,46 priorising peak inspiratory pressure (PIP) rather than plateau pressure, and often targeting tidal volume based on actual body weight rather than predicted body weight. Indeed, observational studies have suggested that PIP and dynamic ∆P (PIP minus PEEP)47 48 are associated with outcome, although recent data also suggests that failure to reduce tidal volume below 7 mL/kg for children with severe PARDS was associated with higher mortality.46 These data suggest that both lung and diaphragm protective strategies may differ in paediatric ARDS (PARDS) as compared with ARDS in adults.
The developing heart of young children is characterised by low myocardial mass and compliance leading to a decrease in contractility and response to an increased preload.49 Furthermore, neonates and infants have higher pulmonary vascular resistances with higher RV after-load which is further exacerbated when they have cardiopulmonary disease.50 Finally, children have strong ventricular interdependence.51 52 Thus, in this fragile population, subtle variations of right pre and after-load induced by the variations of PL and PPL during MV may lead to RVF or global heart failure, and death, in a greater proportion than in adults.
Clinical applications for PL and PPL monitoring in children
PEEP titration
Because infants are particularly susceptible to atelectrauma, a tailored PEEP titration to maintain lung volume seems fundamental. In PARDS, ventilation with PEEP levels below those recommended by the ARDSnet PEEP/FiO2 table was associated with higher mortality.53 Nevertheless, paediatric intensivists are generally reluctant to increase PEEP.53 54 Some of this reluctance stems from concern about very compliant chest walls which may result in high PL, particularly in infants. Other concerns relate to potential haemodynamic effects of PEEP, although paediatric data suggest that PEEP levels exceeding 10 cmH2O do not change stroke volume nor cardiac index.55 Yet, the effect of PEEP variations on RV function remains unknown.56–58 PPL measurements therefore have many theoretical advantages in infants and children for PEEP management, as this will provide a direct measure of chest wall elastance, and the ability to characterise how changes in PEEP affect PPL and potentially haemodynamics. This seems particularly pertinent for children with congenital heart defects and during cardiopulmonary bypass.59 Unfortunately, studies focused on PEEP titration in children are scarce, and the only studies using a PL-targeted PEEP titration are case reports.60 61 Furthermore, there are technical limitations which are crucial to understand in young infants and children for PPL measurements, particularly for applications related to PEEP management (see below).
Estimation of patient effort and ventilator liberation
As previously discussed, PPL may be used to target physiological effort of breathing in order to avoid P-SILI and VIDD. In addition, PPL measurement to estimate respiratory effort is useful during weaning and ventilator liberation. High breathing effort is consistently a risk factor for extubation failure in children, although this assumption is based on subjective clinical examination. Direct measurements, both during SB trials and in the peri-extubation period, are useful to identify patients at risk of extubation failure and who may benefit from non-invasive respiratory support.26 They are also useful to identify patients who have postextubation upper airway obstruction, and follow the consequent therapeutic interventions.62
Patient-ventilator asynchrony
PVA is common in mechanically ventilated children,63 64 but the identification and characterisation of the different types of PVA may be challenging. The use of PPL tracings can enhance the detection of PVA by precisely characterising the timing and duration of patient effort. In particular, PES tracings are very useful to identify trigger based asynchronies such as ineffective triggering, delayed triggering, or reverse triggering.30 Trigger based asynchronies may be a risk factor for VIDD. In infants, ineffective and delayed triggering may cause additional respiratory effort (estimated by the calculation of the oesophageal pressure-time product (PTPES)). These trigger errors are less common in patients with preserved respiratory muscle strength and drive (suggested by a higher PTPES and respiratory rate).65
Conversely, infants who have very compliant chest wall may not be able to generate sufficient PPL variations to induce SILI. PES tracings may help to identify excessive breathing efforts due to insufficient ventilator support. This can lead to flow-undershoot/premature cycling with consequent double-cycle breaths, which may exacerbate both P-SILI and VILI. In ventilatory-dependent infants with bronchopulmonary dysplasia, titration of PEEP with PES has been shown to limit dynamic hyperinflation and improve patient-ventilator synchrony.66 Furthermore, reverse trigger appears to be quite common in children with ARDS who are heavily sedated, and Pes monitoring can help characterise the timing and magnitude of patient effort in relation to mechanical breaths.
Because the optimal level of respiratory effort remains unknown in children, the consequences of PVA are still a matter of debate. Indeed, in children, studies have failed to show any deleterious consequences of PVA on respiratory mechanics and outcome.64 65
PVA is defined as a mismatch between the patient’s ventilatory demand and the ventilator’s provided assistance. It is therefore mandatory to interpret respiratory effort in accordance with the patient’s respiratory drive. This explains the usefulness of measures to avoid or limit excessive or insufficient respiratory drive, such as the monitoring of the electrical activity of the diaphragm (Eadi), a surrogate of the central respiratory output to the diaphragm, which is increasingly used in children.8 Neurally adjusted ventilator assist (NAVA) is a proportional mode of ventilation in which assistance is cycled on and of according Eadi and is delivered in proportion to its intensity. During invasive ventilation, NAVA has been shown to decrease trigger and timing errors as compared with conventional ventilation in neonates, infants and older children67 68 This mode of ventilation may also improve patient’s comfort,69 and reduce sedation and length of stay.70 Finally, Eadi correlates with the effort of breathing71 and thus complete the respiratory assessment as a continuous monitoring tool.72
Despite many theoretical advantages in children, PES measurement is rarely performed in routine paediatric practice. While the lack of robust clincal data likely explains some of this, there are also important limitations of existing methods to estimate PPL in children, which are discussed below.
Paediatric limitations for PL and PPL monitoring
Methods describing accurate insertion of the oesophageal catheter for PES measurements are available for adults. Neverthleess, oesophageal manometry is used by less than 1% of adult intensivists,73 which highlights that the theoretical advantages to PES may be outweighed by technical limitations or ease of use, even in adults. There are certainly unique aspects regarding placement in children, as well as specific calibration of the oesophageal balloon to ensure accuracy, which are unique to children.
First, oesophageal pressure is usually measured with a balloon catheter, although liquid filled, piezo-resistive and fiberoptic catheters have also been described. With balloon catheters, the pressure inside the balloon (estimate of PPL) depends on the pressure transmitted by the surrounding structures, that is, the elastance of the esophagus (EES) and the elastic recoil of the balloon itself. The balloon is inflated to ensure that the holes in the catheter are patent, but if it is overinflated it may occlude the oesophagus, which will artificially increase the pressure. Thus, an inappropriate filling of the balloon may underestimate (underinflation) or overestimate (over-inflation) PPL.74 75 Estimation of PPL in children is even more difficult due to the lack of catheters designed for paediatric use. Furthermore, paediatric catheters are more subject to inaccurate calibration, as the size of the balloon relative to the size of the oesophagus results in a very small window of appropriate filling volume,76 and a narrow range for appropriate depth of insertion. Additionaly, an enteral feeding tube and the presence or absence of SB may also affect the optimal filling volume. For this reason, paediatric specific calibration-methods have been developed.76 As an alternative, several other types of technologies (ie, liquid filled catheters, piezoresistive catheters, fiberoptic catheters) have been used to estimate PPL swings, but many are insufficiently accurate to estimate the absolute value of PPL.77 78 The ideal catheter should include an integrated feeding tube to limit invasiveness and discomfort in children.
Second, PES does not reflect PPL over the entire lung height and depends on body position.79 In the supine position, PPL is higher in the dorsal regions and lower in the ventral regions. This vertical gradient is partly explained by the compressive gravitational forces of the mediastinum80 may be higher in the injured lung.81 82 Hence, PES corresponds to PPL in the mid-lungs (surrounding the oesophagus), and its use to estimate PPL (and PL) in the dorsal zones may lead to erroneous PEEP titration. To avoid this bias, it has been suggested that PL should be estimated with a calculation based on the changes of PES and PAW rather than their absolute value (elastance-derived method described in online supplemental file and figure 2).83 These calculations have not been validated in children. Furthermore, no study has yet investigated these regional differences as well as the impact of prone position versus supine position on PPL measurement in children. This makes the interpretation of PES more difficult and uncertain in children.
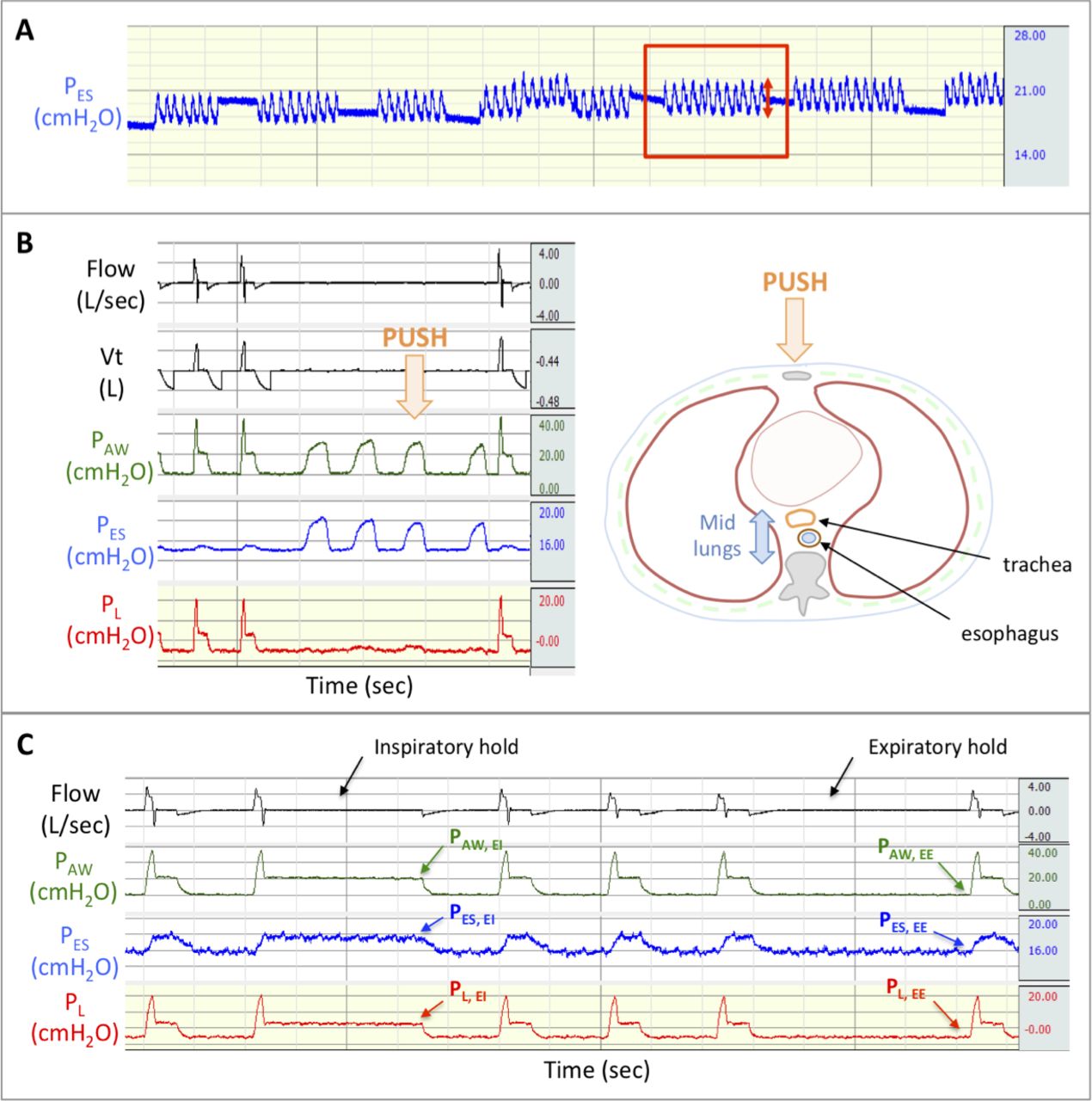
Technical aspects of oesophageal balloon catheter placement for PL monitoring during controlled ventilation. (A) Filling test: PES swings during balloon’s inflation with increasing volumes. Optimal volume (in red box) is the one where ∆PES is maximum (red double arrow). (B) Occlusion test: similar pAW and PES variations during a gentle compression of the chest wall while performing expiratory hold; oesophageal catheter reflects accurately PPL in the mid-lungs. PES provides a valid measure of PPL when the ratio approaches unity (0.8–1.2). (C) Static respiratory, chest wall and lung mechanics during inspiratory and expiratory holds. · direct method for expiratory-PL: Expiratory-PL=PL,EE=PAW,EE-PES,EE in adults, expiratory-PL should be close to zero. · Elastance-derived method for inspiratory-PL: pL, EI=PAW,EI-PES,EI ∆PL= PL,EI-PL,EE eL=∆PL/Vt and ERS=∆PAW/Vt. Inspiratory-PL= PAW,EI*EL/ERS = PAW,EI*∆PL/∆PAW in adults, inspiratory-PL should be limited to 20–25 cmH2O and ∆PL to 10–12 cmH2O. EE, end-expiratory; EI, end-inspiratory; PAW, airways pressure; PES, Oesophageal pressure; PL, Transpulmonary pressure; VT, tidal volume.
Third, optimal placement and calibration may be challenging in children. The length of the oesophagus is small relative to the size of the oesophageal balloon, which provides a narrow range for correct placement. Furthermore, cardiac oscillations may be more pronounced on PES tracings in some children, which sometimes makes it challenging to obtain accurate measures of absolute PPL (ie, with the cardiac oscillation the pressure can change by 2 cmH2O). Adult studies advocate the use of occlusion manoeuvres (to ensure PAW and PES are similar) to confirm placement and calibration. These methods may not perform as well in children who have more compliant chest walls.
Fourth, few studies have described the lung and chest wall mechanics in healthy children: normal values of lung compliance have been defined in older ventilated children84 or in spontaneously breathing preschool children,85 but there are no reference values for the entire paediatric age range, especially in mechanically ventilated children. Finally, parents may be reluctant to allow the use of an additional invasive measure, such as PES, in their child within the stressful environment of PICU.86
Table 2 summarises the catheters that may be used in children. However, most catheters have been used essentially in adults, the extrapolation to children has thus to be cautious.
Balloon catheters that may be used in children (tested in vitro)
Future directions for paediatric research and clinical practice
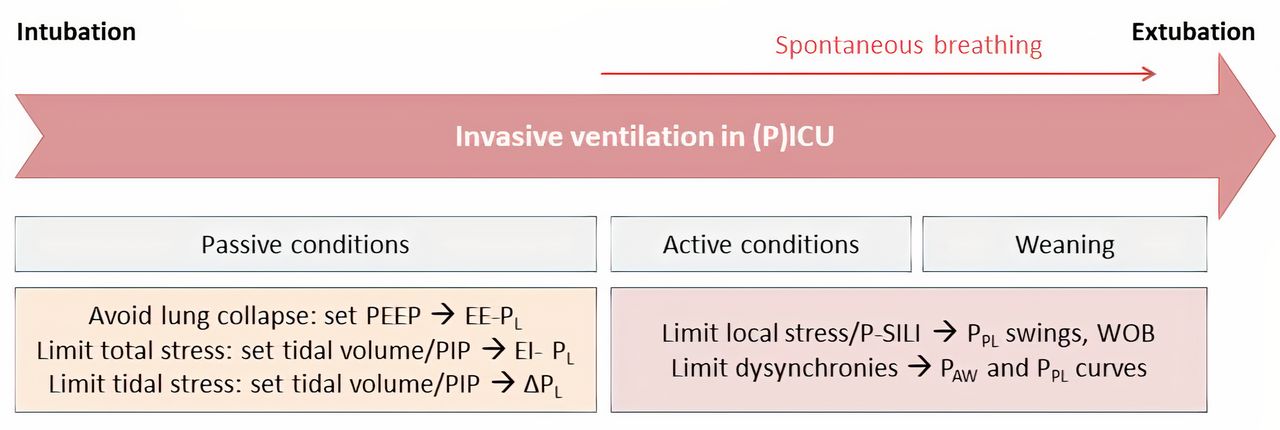
Despite its wide range of potential applications (figure 3), the use of PL to optimise protective MV remains limited. The numerous MV-induced complications raise doubts about the benefits of a titration based on a single physiological measure. The new concept of mechanical power, which considers PL together with insufflation flow, respiratory rate and PEEP, highlights the fact that monitoring of solely PL is probably insufficient to prevent VILI.87 PL might rather be included in a multimodal ventilatory strategy including other parameters reflecting respiratory mechanics, neuroventilatory control and/or haemodynamics. The use by trained physicians of standardised protocols allowing bedside assessment of respiratory and lung mechanics has shown to be associated with an improvement in protective ventilation and oxygenation.88 89 The growing interest in machine learning over the last decades led to the development of computer-based clinical decision support systems (CDS) for protective ventilation.90 91 A CDS including PES to maintain the effort of breathing within a safe window has been recently developed for critically ill children, and may shorten the duration of MV.33 This promising tool is currently being tested in a large randomised controlled trial.92 The investigation of PL measurement within multimodal ventilatory strategies may be interesting for future clinical studies.

{kind=link}
{kind=link}
{kind=link}
Schematic representation of the situations in which pleural and transpulmonary pressure monitoring may be of help at the bedside.EE, end-expiratory; EI, end-inspiratory; PAW, airways pressure; PL, transpulmonary pressure; PPL, pleural pressure; PEEP, positive end-expiratory pressure; PICU: paediatric intensive care unit; PIP, peak inspiratory pressure; P-SILI, patient self-inflicted lung injury; WOB, work of breathing.
Even if technical limitations of PES can be overcome, the technique is invasive. As such non-invasive estimation of PPL and PL, without a catheter is an important research focus. Several techniques are under evaluation and require further validation: (1) the « PEEP step » method is based on the assumption that EL can be calculated as the ratio of changes in PEEP and EELV during PEEP increment.93 The technique’s limitations (such as the assumption that ECW equals zero during PEEP increment, and the need for controlled ventilation) have restrained its use in patients with ARDS,94 without any evaluation in children; (2) the right atrial transmural pressure, which can be calculated as the intravascular central venous pressure (CVP) minus the surrounding pressure of the atrium, approaches PPL. Based on this assumption, it has been attempted for decades to approximate ∆PES using variations in CVP (∆CVP), with conflicting results.95 96 In children having undergone cardiac surgery, a new method using a derived-∆CVP during an occlusion test has provided a better estimate of ∆PES, allowing an accurate calculation of inspiratory PL.97 This encouraging method should be tested in children with PARDS who are more hypoxaemic, need higher PEEP and may have different elastance ratios; (3) the modifications of PAW curves during inspiratory holds (according to a technique similar to that of respiratory muscle functions) may provide a direct and accurate estimation of the degree of respiratory effort,98 provided that the patient remains passive at the end of inspiration. Finally, for spontaneously breathing children, airway occlusion manoeuvres such as the maximal inspiratory pressure (MIP) and the pressure generated after 0.1 sec of occlusion (P0.1) may provide a reliable way to identify patients with strong respiratory effort.99 100
Conclusion
PPL monitoring using oesophageal manometry is a promising tool to limit VILI, P-SILI and VIDD in children. Unfortunately, oesophageal manometry has many technical limitations in children, which confines its use to only a handful of research centres. Paediatric evidence seems currently too weak to use oesophageal manometry in routine respiratory monitoring. The low incidence rate of PARDS and the heterogeneity of critically ill children in terms of age, diseases and respiratory mechanics hinders large prospective controlled trials. To expand the use of such new tailored therapies in clinical practice, future research should integrate improvements in the technology for use in children, in addition to development of and validation of noninvasive estimation of PL and multimodal respiratory monitoring for use in children.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors MV-C, SK and BF conceptualised and designed the study. MV-C performed the initial search and classification for the articles. All the authors checked classification and inclusion of the selected articles (collection of data). MV-C drafted the first manuscript, supervised by BF, and was helped by AD, DC and RK, for specific sections. MO, FL, SR, SK, RK, DC, AD and BF reviewed, edited and approved the final version to be published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests AD reports personal fees from Medtronic, grants, personal fees and non-financial support from Philips, personal fees from Baxter, personal fees from Hamilton, personal fees and non-financial support from Fisher & Paykel, grants from French Ministry of Health, personal fees from Getinge, grants and personal fees from Respinor, grants and non-financial support from Lungpacer, outside the submitted work. MV-C reports non-financial support from Sentec, outside the submitted work. RK reports personal fees from OrangeMed Nihon Kohden, and grants from Masimo outside the submitted work.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.