Article Text

Abstract
Given the large numbers of people infected and high rates of ongoing morbidity, research is clearly required to address the needs of adult survivors of COVID-19 living with ongoing symptoms (long COVID). To help direct resource and research efforts, we completed a research prioritisation process incorporating views from adults with ongoing symptoms of COVID-19, carers, clinicians and clinical researchers. The final top 10 research questions were agreed at an independently mediated workshop and included: identifying underlying mechanisms of long COVID, establishing diagnostic tools, understanding trajectory of recovery and evaluating the role of interventions both during the acute and persistent phases of the illness.
- COVID-19
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
Introduction
Since its first description 2 years ago to date, the SARS-CoV-2 has infected at least 250 million people worldwide and resulted in over 5 million deaths.1 For survivors, there is a high rate of delayed recovery, ongoing symptoms, reduced health-related quality of life and inability to return to work.2 ‘long COVID’ describes the persistence of symptoms or disability after the acute infection, not explained by an alternative diagnosis.3 In patients hospitalised with COVID-19, only 3 out of 10 patients felt fully recovered at 6 months4 and 12 months postdischarge.5 With over half a million adults admitted to hospital in the UK to date,6 symptomatic survivors of COVID-19, represent a large and growing population.
Given the persistence of the coronavirus pandemic and the large numbers of people affected, it is important to define research priorities to aid effective targeting of resources. Previous attempts to do this have focused on the research priorities of the clinical community in adults7 and airways disease.8 The WHO and International Severe Acute Respiratory and emerging Infection Consortium have recently published six key research priorities for coronavirus which were refined through a multistakeholder forum.9 Research prioritisation involves a broad reach of patient and clinical stakeholders as well as considering questions of feasibility. One approach successfully deployed in other disease areas is that of the James Lind Alliance (JLA), a non-profit-making initiative partly funded by the National Institute for Health Research. The JLA has a well-established process to ensure that those most affected by a condition are involved in prioritising research (https://www.jla.nihr.ac.uk/).
The post-hospital COVID-19 (PHOSP-COVID) study is a UK-wide national research collaboration examining the long-term sequelae of COVID-19 (https://www.phosp.org). Over 7500 patients discharged from over 80 UK hospitals between March 2020 and March 2021 were recruited by March 2022. This places the PHOSP-COVID consortium in a unique position to establish a priority setting partnership (PSP) for research into long COVID. The aim was to produce a top 10 research priority question list for survivors of a hospital admission with COVID-19.
Methods
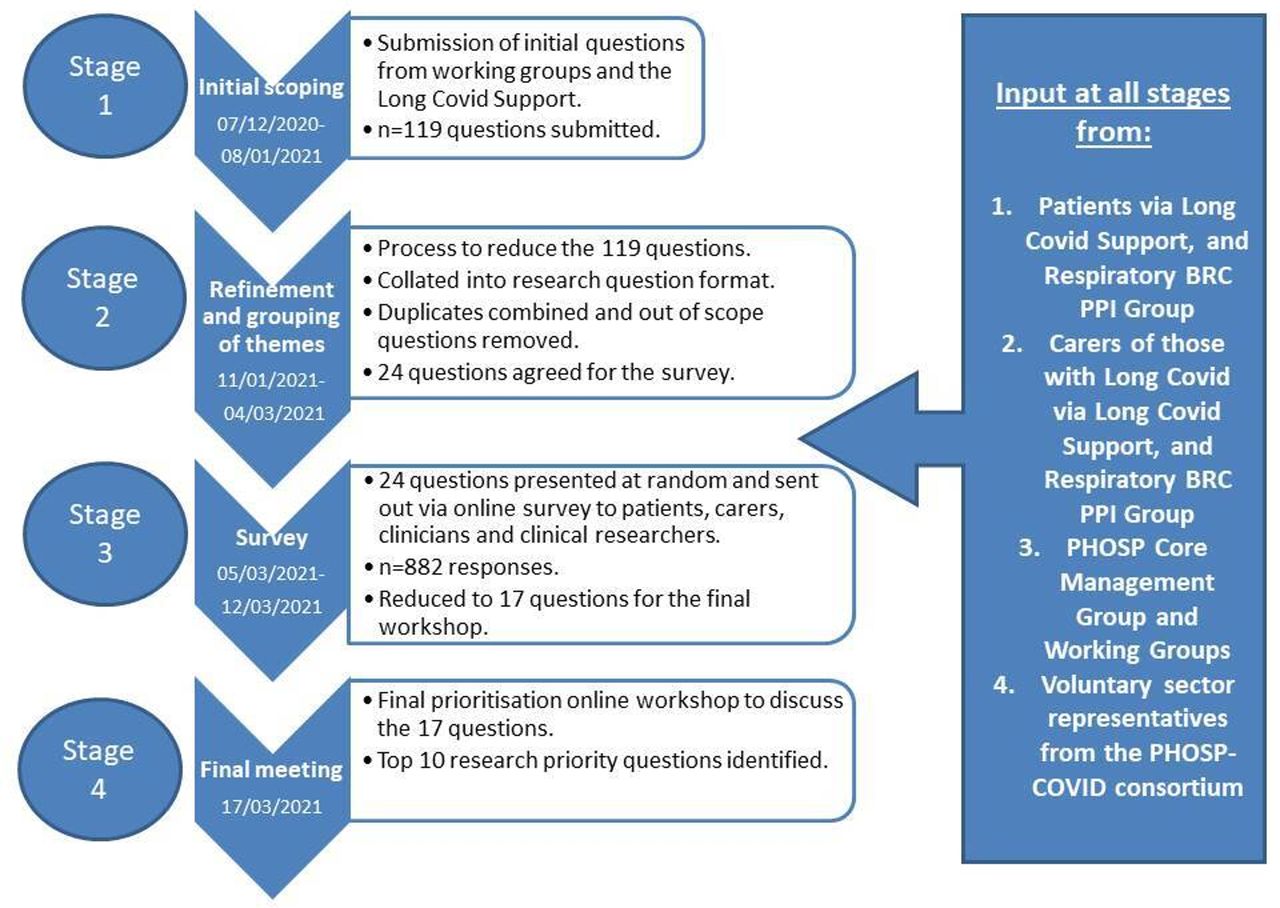
Our PSP took place between December 2020 and March 2021 and incorporated views from adults with self-reported experience of long COVID (both hospitalised and non-hospitalised for the acute illness), carers, clinicians and clinical researchers. We used an adapted version of the JLA process10 as outlined in figure 1. The elicitation survey requested contributors answer the following: ‘what questions would you like to see answered by research into the longer term consequences post-hospital admission for COVID-19?’ This was shared with multiple patients, clinicians and relevant stakeholders including members of the 13 PHOSP-COVID working groups (step 1) detailed in online supplemental figure S1. The initial questions were combined, reworded (step 2) and then shared across multiple platforms via an online prioritisation survey (step 3). Survey questions were presented in random order for each individual. The final top 10 research questions were agreed at a dedicated prioritisation workshop (online supplemental figure S2) mediated by independent JLA facilitators and hosted via videoconference (step 4). Ethical approval was not required but patients and clinicians provided verbal consent to be recorded during the workshop.
Supplemental material
{kind=link}
Methodology of the research prioritisation process and input at all stages from key stakeholders. BRC PPI, Biomedical Research Centre Patient and Public Involvement; PHOSP, post-hospitalisation COVID-19.
Results
The elicitation survey generated 119 questions from long Covid Support (patient group) and the PHOSP-COVID working groups (online supplemental tables S1 and S2). There was considerable overlap in questions posed by patients and clinicians and between different working groups. Similar questions around specific organs/symptoms were combined and questions outside of scope were omitted. A refined list of 24 questions was reviewed by patient groups to ensure wording was clear (online supplemental table S3).
There were 882 respondents to the online survey of whom 819 (93%) were individuals with self-reported long COVID. There was consistency in the prioritisation shown between individuals with self -reported long COVID who were either hospitalised or non-hospitalised (online supplemental table S4). The highest ranked 17 questions were selected from this for the prioritisation workshop (online supplemental table S5). The final list of top 10 priority questions is shown in box 1.
Outcome of research prioritisation: final list of top 10 research questions (not ranked).
What are the underlying mechanisms of long COVID that drive symptoms and/or organ impairment?
What imaging techniques or scans may be able to detect and predict the development of organ problems or wider systemic issues?
What happens to the immune system throughout patients’ recovery from COVID-19?
What can data at 6 and 12 months tell us about the long-term trajectory of illness?
What blood or other laboratory tests may be able to detect and predict the development of organ problems or wider systemic issues?
What is the impact of treatment(s) during the acute (initial) stage of COVID-19 on recovery?
What are the problems within the muscles associated with symptoms limiting activity/function/exercise? If so, what can be done to help?
What medications, dietary changes, supplements, rehabilitation and therapies aid recovery?
What can be done to support mental well-being during recovery?
What is the risk of future adverse health events (eg, stroke, heart attack)?
Discussion
In this codeveloped priority setting process, we have identified key research priorities for improving our understanding of long COVID. Patients, patient charities and carers were closely involved throughout the process, including in question generation, phrasing and prioritisation. The final research question list was, therefore, broad and reflects the major problems reported 1-year postdischarge from hospital.2 5 It differs from previous reports published earlier in the pandemic, which were largely informed by clinician input.7 8 Our identified priorities included understanding the underlying mechanisms of long COVID, which drive ongoing symptomatic illness. Related to this, there was an emphasis on identifying diagnostic and prognostic tools, including both imaging and biomarker-based approaches. Finally, there was also a strong emphasis on the potential role of both pharmacological and non-pharmacological interventions to treat symptoms.
Adherence to the principles of JLA methodology was a strength of this PSP, but the need to generate these data rapidly during a pandemic meant that we were unable to follow the full JLA process. For example, the time scale for delivery was significantly shortened. Shorter response times may have impacted on survey responses. We cannot calculate the response rate as the survey was made available publically and the denominator is, therefore, unknown. We were unable to collect detailed demographic data from the survey respondents, so we cannot be certain how representative the sample is. The survey respondents were biased towards individuals with self-reported long COVID who had not been admitted to hospital. The workshop, however, involved an equal number of hospitalised and non-hospitalised patient attendees, and between those with lived experience or other expertise. As our understanding of long COVID evolves, it may be necessary to re-evaluate research priorities
To summarise, we have completed a comprehensive and inclusive research prioritisation exercise to identify the top priority questions for research to improve outcomes for survivors of a hospital admission for COVID-19. The relevance may extend to people with long COVID who were not hospitalised. Given the large numbers of people with long COVID, and the persistence of the pandemic, this is an important resource to help inform future research strategies and policy.
Ethics statements
Patient consent for publication
Ethics approval
The PHOSP-COVID study involves human participants and was approved by Leeds West Research Ethics Committee20/YH/0225. Participants gave informed consent to participate in the PHOSP-COVID study. No specific consent was necessary for the prioritisation exercise.
Acknowledgments
The authors would like to thank Suzannah Kinsella, Toto Grunland, Tricia Ellis and Amy Street from the James Lind Alliance (JLA) for facilitating the online workshop, in addition to Maryrose Tarpey (co-author).
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @ClaireHastie1, @Moodwife, @ColinBerryMD, @bolton_char, @alexrhorsley, @REvans_Breathe
Collaborators The PHOSP Consortium.
Contributors The manuscript was initially drafted by LH-W, RAE, AH, MM, KP, KH and further developed by the writing committee. LH-W, KP, KH, CH, RAE, CEB, MT made substantial contributions to the conception and design of the work. LH-W, KP, KH, CH, RAE, MT made substantial contributions to the acquisition of data. OE, HM, BR, MR, ADS, JG, JJ, SJS, LVW, AH, MM, CEB, RAE made contributions to the analysis or interpretation of data for the work. CH, KR, NR, NS, DA, PB, JC, CC, MD, NG, RG, LS, CB, CBo, TC, ADS, JRG, SH, JJ, BR, MR, SJS, DT, MT, MM were attendees at the workshop and therefore to the acquisition of data. All authors contributed to data interpretation, critical review and revision of the manuscript. All authors had full access to all the data in the study and had final responsibility for the decision to submit for publication. RAE is guarantor of the published work.
Funding PHOSP-COVID is supported by a grant from the MRC-UK Research and Innovation and the Department of Health and Social Care through the National Institute for Health Research (NIHR) rapid response panel to tackle COVID-19 (grant references: MR/V027859/1 and COV0319). Core funding was provided by NIHR Leicester Biomedical Research Centre to support the PHOSP-COVID coordination team, and NIHR Biomedical Research Centres (BRCs), Clinical Research Facilities (CRF) and NIHR Health Protection Research Unit (HPRU) and Translational Research Collaborations (TRCs) network across the country. This research was funded in whole or in part by the Wellcome Trust [209553/Z/17/Z] for author JJ. RAE held a NIHR Clinical Scientist Fellowship CS-2016-16-020 during the conduct of the study.
Disclaimer The views expressed in this publication are those of the author(s) and not necessarily those of the MRC, NIHR or the Department of Health and Social Care.
Competing interests LH-W reports grants from the NIHR and ARC, outside the submitted work. TC reports grants from UK NIHR, UKRI and Guy’s and St Thomas’ Charity. She has delivered workshops on persistent physical symptoms in the context of long-term conditions, during the conduct of the study for which she has received payment. She is the author of self-help books on fatigue. She is a member of the NICE expert advisory panel for Covid19 Rapid Guidelines.JJ reports fees from Boehringer Ingelheim, Roche, NHSX and GlaxoSmithKline unrelated to the submitted work. JJ is supported by Wellcome Trust Clinical Research Career Development Fellowship 209,553/Z/17/Z and the NIHR UCLH Biomedical Research Centre, UK.SH reports consultancy for Eli Lily, NovoNordisk and Zealand Pharma for which his institution has received payment. He serves on a speaker panel for NovoNordisk for which he and his institution receive payment. MR is currently employed by Roches on a one year senior academic/ industry fellowship. JDC reports grants and personal fees from AstraZeneca, Boehringer-Ingelheim, GlaxoSmithKline, Novartis, and Insmed, personal fees from Chiesi, Zambon, Janssen, and Grifols, and grants from Gilead Sciences, outside the submitted work. AH reports personal fees from Vertex Pharmaceuticals, Mylan Healthcare, and the Cystic Fibrosis Foundation, and grants from JP Moulton Trust and NIHR, outside the submitted work. MT reports personal fees from Merck Sharp & Dohme and GlaxoSmithKline, and grants and personal fees from Bayer and Actelion, during the conduct of the study. LVW reports grants from GlaxoSmithKline and Orion, outside the submitted work. ADS reports grants and personal fees from AstraZeneca, Bayer, Boehringer, Chiesi, Forest Laboratories, GlaxoSmithKline, Grifols, Insmed, MedImmune, Novartis, Pfizer, and 30T, outside the submitted work. RAE reports grants from GlaxoSmithKline during the conduct of the study; and grants from the National Institute for Health Research (NIHR) and personal fees from GlaxoSmithKline, AstraZeneca, and Chiesi, outside the submitted work. All other authors declare no competing interests.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.