Article Text

Statistics from Altmetric.com
This British Thoracic Society (BTS) Clinical Statement addresses occupational asthma and includes key clinical practice points. In an era in which medical practice is increasingly determined by evidence-based guidelines, it must be acknowledged from the outset that there is little or no published evidence for some of the areas covered in this statement1 2; thus, much of the advice is based on expert opinion and accumulated clinical experience.
Methodology
The Clinical Statement Group (CSG) was chaired by Dr Chris Barber. Membership was drawn from current and former members of the BTS Occupational and Environmental Lung Disease Specialist Advisory Group. The CSG identified key areas requiring clinical practice points. The overall content was developed to reflect the scope approved by the BTS Standards of Care Committee (SOCC). Following discussions of broad statement content, individual sections were drafted by group members. A final edited draft was reviewed by the BTS SOCC before posting for public consultation and peer review on the BTS website (August/September 2021). The revised document was approved by the BTS SOCC in November 2021 before final publication.
Summary of clinical practice points
Section 1—introduction
Healthcare professionals should be aware that occupational exposures account for around one in six cases of asthma in adults of working age.
Over 400 causes of Occupational Asthma (OA) have been described; these are categorised as high-molecular weight (HMW) or low-molecular weight (LMW) ‘respiratory sensitisers’.
Although individual susceptibility plays a key role, the main risk factor for the development of OA is the level of allergen exposure in the workplace.
Section 2—work context
Health surveillance is a form of workplace screening that can identify OA cases early. In the UK, it usually consists of an annual symptom questionnaire and spirometry.
Workers found at health surveillance to have new asthma symptoms or abnormal lung function should be referred as soon as possible to a specialist with expertise in OA.
Section 3—diagnosis
Many patients with OA in the UK are diagnosed at a late stage; healthcare professionals should be aware of the important benefits of recognising cases early.
All patients of working age with new symptoms suggestive of asthma, reappearance of childhood asthma, deteriorating asthma control or unexplained airflow obstruction should be asked about their job, and whether their symptoms are the same, better or worse on days away from work (eg, rest days or holidays).
Symptomatic asthma patients in high-risk jobs, and those reporting improvement away from work, should be referred as quickly as possible for specialist assessment (where possible, directly to a specialist occupational lung disease service)
A diagnosis of OA has important health and employment implications and should not be made based on a compatible history alone.
The diagnosis of OA is most easily made prior to workplace adaptations and starting maintenance treatment.
Objective tests commonly used in the UK include skin prick tests (SPTs), specific IgE antibody levels and serial measures of peak expiratory flow (PEF) or airway responsiveness; workplace and specific inhalation challenges (SIC) are less commonly required for OA diagnosis.
Section 4—management
Managing patients with OA can be complex and should wherever possible be carried out by a physician with specialist expertise in this condition.
It is important to educate patients with OA that the best opportunity for improved asthma control comes from early, and complete, cessation of exposure to the cause.
Management of OA includes standard pharmacotherapy, asthma education and smoking cessation advice, following national guidelines.
Patients with OA may have coexisting and related conditions (eg, occupational rhinitis, breathing pattern disorder, inducible laryngeal obstruction (ILO), anxiety and depression) that require assessment and treatment.
Clinicians should work in partnership with patients to develop (and adapt as necessary) a personalised management plan aiming for the best possible balance between long-term health and employment outcomes.
Where consent is given, liaising directly with occupational health providers and/or employers gives the best chance of suitable workplace adaptations being made, to keep patients and their coworkers safely employed.
Patients with OA should be provided with written information confirming their diagnosis, the implications this has on their current and future jobs as well as Industrial Injuries Disablement Benefit (IIDB) and civil compensation advice.
While there is potential for ongoing exposure to the cause, patients with OA should remain under specialist follow-up to monitor asthma control, lung function and the impact of any workplace interventions.
Section 5—prognosis
Around one in six patients with OA meet established criteria for severe asthma.
Prognosis in OA is largely determined by asthma severity at the time of diagnosis, and whether workers continue to be exposed to the cause thereafter.
Around 25–30% of OA patients who permanently cease exposure will make a full recovery, and another 30–35% will report a reduction in symptoms with treatment.
Patients with OA who remain exposed to the cause are at risk of accelerated lung function decline, which may result in a degree of fixed airflow obstruction.
Patient with OA have an increased risk of unemployment, with approximately one in three being out of work 3–5 years after diagnosis.
Anxiety and depression are common in OA, affecting up to half of patients.
Section 1 introduction
Asthma is a common health condition in the UK adult population, affecting over 5 million individuals. For those in employment, asthma control may be adversely affected by factors in the workplace, and the term ‘work-related asthma’ (WRA) is used.1 3 Although the true frequency of this condition is unknown, it is relatively common, affecting around 20%–25% of working individuals with asthma.4–6
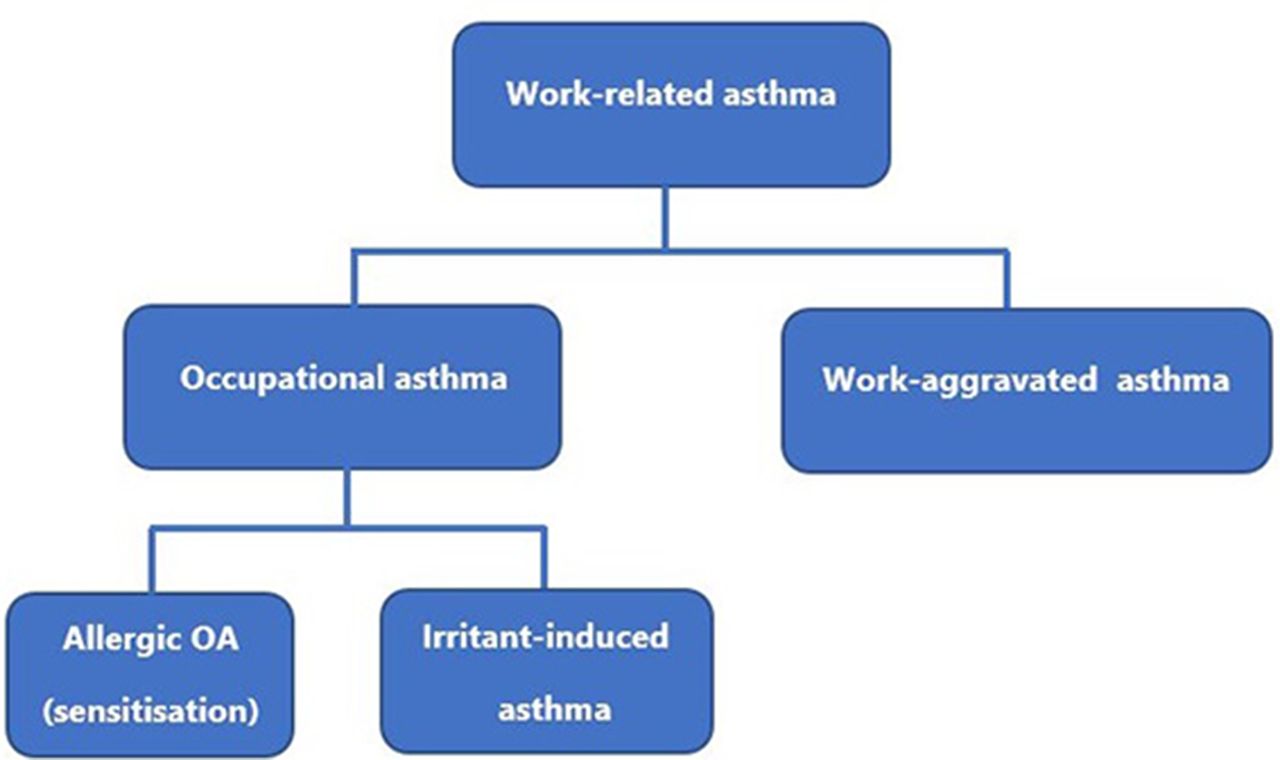
WRA is subdivided into three main phenotypes—work-aggravated asthma (WAA), allergic occupational asthma due to sensitisation and irritant-induced asthma (IIA)3 (figure 1).

Classification of work-related asthma.
Patients with WAA either have pre-existing asthma or develop coincidental adult-onset asthma and report symptoms that are made worse by non-specific factors in the workplace. Common causes of WAA include extremes of workplace temperature or humidity, exertion from manual work tasks, workplace stress or anxiety and exposure to non-specific dusts, fumes, or air pollution.
In contrast, occupational asthma is caused by airborne exposures in the working environment and accounts for around one in six cases of adult asthma.7 This condition is further subdivided into two separate conditions; IIA (covered in online supplemental Appendix 1) and occupational asthma due to allergic sensitisation (the main topic of this document; from now on referred to simply as ‘OA’).
Supplemental material
Causation
Although there are over 400 known causes of OA (known as asthmagens),2 most cases in the UK are related to exposure to a small number of workplace allergens, most commonly flour dust or isocyanates.8 Asthmagens are usually divided into HMW or LMW sensitisers1 9; commonly reported causes are shown in table 1. OA caused by repeated exposure to HMW proteins is an IgE-associated response, involving T-helper cells. This immune mechanism is also known to be relevant to a small number of LMW causes (eg, acid anhydrides and platinum salts), but for the majority, the immune pathways responsible for sensitisation remain to be determined.10
Frequently reported causes of occupational asthma, by molecular weight
Whatever the underlying mechanism, OA due to allergic sensitisation requires a period of repeated allergen exposure, the duration of time between first exposure and symptom onset being referred to as the ‘latent period’. Although the highest risk of OA is within the first year of exposure,1 reported latency is variable, ranging from a few weeks to many years.11 Sensitised workers (particularly with HMW allergens) are also at risk of other related forms of occupational allergy, such as rhinitis and conjunctivitis, which may precede, or coincide with, the onset of asthma symptoms.1
The most important risk factor for the development of OA (and the preceding allergic sensitisation) is the level of exposure to the cause.1 In addition, individual susceptibility plays an important role, as only a proportion of similarly exposed workers become sensitised, and only some of these will ever develop OA. Research studies of exposed populations of workers have not established consistent individual risk factors to account for this, but in some cases have found an increased risk among workers with an allergic (atopic) tendency, who are cigarette smokers, or have certain genetic polymorphisms.1 12
Clinical practice points
Healthcare professionals should be aware that occupational exposures account for around one in six cases of asthma in adults of working age.
Over 400 causes of OA have been described; these are categorised as HMW or LMW ‘respiratory sensitisers’.
Although individual susceptibility plays a key role, the main risk factor for the development of OA is the level of allergen exposure in the workplace.
Section 2 work context
Being in work is important for long-term health and well-being, providing individuals with income, social interaction, purpose and identity.13 The benefits of being employed require workplaces to be safe and free from risks to health; there is a legal duty for employers to consider this under the Health and Safety at Work Act14 and Control of Substances Hazardous to Health (COSHH) Regulations15 (more detail is provided in online supplemental Appendix 2). Employers are required to carry out risk assessments to identify any potential asthmagens and decide how to prevent or minimise the risk of OA in their workforce. Based on the hierarchy of controls (online supplemental Appendix 2), the most effective measures should be used wherever practical (figure 2). If there is a residual risk of exposure to an asthmagen, health surveillance for OA is required.15 16

Diagram representing the ‘hierarchy of control measures’ from most effective at the top, to least effective at the bottom. RPE, respiratory protective equipment.
Health surveillance
Although a largely preventable disease, there is no ‘safe-level’ of exposure that will completely prevent OA in all individuals. Health surveillance is a form of secondary prevention (similar in concept to health screening) that aims to identify workers with OA at an early stage, reducing the severity and impact of the disease.15 16 When workers are part of a health surveillance programme, there is some evidence that the diagnostic process is shorter and that the cases identified are less severe.17 18 Unfortunately, most patients developing OA are not identified early through this process, as only ~30% of British workers have access to occupational health.19
Annual surveillance is generally carried out by an occupational health provider and usually consists of a respiratory symptom questionnaire and spirometry; in some special circumstances such as the detergent and precious metal refining industries, immunological surveillance is also used.16 Workers found to have new symptoms of asthma, airflow obstruction, accelerated forced expiratory volume (FEV)1 decline ((≥15% from baseline, in addition to expected age-related loss)20 or sensitisation to a workplace allergen, may be referred to an occupational physician, their General Practitioner (GP) or directly to a specialist centre. A successful health surveillance programme requires careful planning, engagement of the workforce and a good relationship between managers and employees. Workers will naturally be less likely to report asthma symptoms if they are concerned that this might have a negative impact on their income or employment prospects.21 22
Clinical practice points
Health surveillance is a form of workplace screening that can identify OA cases early. In the UK, it usually consists of an annual symptom questionnaire and spirometry.
Workers found at health surveillance to have new asthma symptoms or abnormal lung function should be referred as soon as possible to a specialist with expertise in OA.
Section 3 diagnosis
Early diagnosis of OA is important, but a UK study found the average duration of symptoms prior to diagnosis was 4 years23; in keeping with the diagnostic delays of between 1.5 and 5 years reported elsewhere.24–27 The reasons for late diagnosis are multifactorial; in some cases, a lack of awareness or patient engagement is responsible,22 28 whereas in others, diagnostic delays result from missed opportunities to ask simple screening questions in primary and secondary care.29 30
A high index of suspicion is, therefore, required, and a suggested algorithm for the assessment and referral of patients presenting with possible OA to healthcare workers in primary or (non-specialist) secondary care is shown in figure 3. While the choice of referral centre is decided by the initial healthcare professional,31 where available this should be directly to a specialist centre with an occupational lung disease outpatient service; the UK has a well-established and linked network of centres that have access to the full range of OA diagnostic facilities (the Group of Occupational Respiratory Disease Specialists (GORDS)).32 Early assessment of workers with suspected OA is important, and for those who remain exposed in the workplace, it is reasonable to expect a first appointment within 6 weeks of referral.

Recommended algorithm for the assessment and referral of patients with possible occupational asthma presenting in primary or non-specialist secondary care.
The diagnostic process
Establishing, or excluding OA has potentially serious consequences for individual patients, their coworkers and their employers; wherever possible, this should be supported by the results of standard objective tests.1 2 No single diagnostic test exists for OA, and the exact approach used will vary, based on the circumstances of the individual patient, the level of practice and experience of the healthcare professional and the testing facilities that are available. The diagnostic process is reliant on patient engagement and some will choose not to proceed due to employment concerns. In other cases, it may not be possible to make a definitive diagnosis, as patients may have left the employment that may have caused their asthma and have no intention of returning to it or similar work. In these cases, the diagnosis is reliant on the clinical and occupational history, available contemporary measurements of lung function and, in suitable circumstances, the identification of specific sensitisation.
Clinical and occupational history
History taking plays a key role in making a diagnosis in OA1 33 but requires specialist knowledge, training and experience. In addition to the standard clinical assessment for a patient with suspected asthma, additional time is required to take a full occupational history; 1-hour outpatient appointments are the recommended standard for new patient consultations.34 Some of the important elements of the occupational history are listed in table 2.
Key elements of the occupational history for patients with suspected OA
A detailed discussion of respiratory symptoms should be documented, as well as their relationship to work, using neutral questions such as:
‘Is your (cough, wheeze, chest tightness) the same, better or worse on your days away from work, such as rest days or holidays?’
A diagnosis of OA cannot be made based on history alone; however,1 2 as symptoms of other conditions (eg, WAA, ILO, and chronic obstructive pulmonary disease) may also improve away from work. Equally, an absence of work-related symptoms cannot be used in isolation to definitively exclude the diagnosis of OA, as these may not be reported by some patients with chronic disease, poor health perception or employment concerns.
Eliciting a history of exposure to a known asthmagen is, therefore, of paramount importance, as this, in combination with work-related asthma symptoms, significantly increases the probability of OA.
In addition to the respiratory history, patients should also be asked whether they have any symptoms suggestive of other occupational allergies (rhinitis, conjunctivitis or contact dermatitis), or coexisting conditions (eg, breathing pattern disorders, ILO, anxiety and depression).35 36
The differential diagnosis of OA is discussed further in online supplemental appendix 3.
First-line diagnostic tests
In general, diagnostic tests for OA lose sensitivity over time when exposure to the cause has ceased or is significantly reduced37 and can also be affected by asthma medication.38 Where it is safe to do so, investigations should, therefore, be carried out as early as possible, prior to the commencement of maintenance therapy, and while patients are still working in the job considered to be the possible cause of their asthma. A summary of the diagnostic tests used in OA is provided in online supplemental appendix 4.
Serial PEF recordings
For many patients, serial PEF measures offer a cheap and simple first-line approach to assessing the physiological response to inhaled agents in the workplace, and in specialist settings, acceptable records can be obtained in up to two-thirds of those in whom OA is being considered.1 They are only helpful if the patient is still exposed to the potential causal agent and require measurements during periods of time at, and away, from work. Work-related PEF changes do not usually confirm a specific cause for OA, and may also be seen in WAA, and occupational hypersensitivity pneumonitis.39
Dependant on locally agreed protocols, PEF recording may be commenced by occupational health, primary or secondary care practitioners at the time of referral, so that charts are available for analysis when patients are seen in specialist centres. Patients may need to be taught how to use the PEF metre (standard or data-logging) and how to keep a record of the readings (a YouTube video is available).40 Copies of all charts should be retained by the patient, and these should ideally be completed on a pro forma that aids data entry into software that permits their interpretation.41 Suitable record forms and support are available online.42 43
The following are evidence-based minimum requirements for serial PEF recordings1 2:
at least four readings a day (prebronchodilator where possible and taking the best of three each time as the recorded value). It is ideal to aim for 2 hourly recordings during waking hours in order that at least four readings will be recorded.
Carried out for at least 3 weeks. Ideally, there should be at least 3 days in each consecutive work period, four evenly spaced readings per day and three series of consecutive days at work with three periods away.
Work times, tasks, exposures and medication use should also be recorded.
Ideally, the doses of maintenance asthma medication should be kept constant during the recording period.
A previous meta-analysis of 31 serial PEF studies reported a pooled sensitivity of 75% and specificity of 79% for a diagnosis of OA, with higher values (82% and 88%) for records with more complete data.44 The method of analysis of serial PEF records is a matter of choice, although most UK centres use a computerised quantitative approach to ease comparison between cases and between centres; the Oasys software permits pattern recognition and produces an Oasys score (>2.5 confirming a positive work effect).41 In addition to the Oasys score, other diagnostic metrics are also calculated from the same raw data.,45–47
Where findings are equivocal, it is recommended that the monitoring is repeated over a longer period, ideally including a more prolonged time away from work48 (eg, before, during and on return from a week or more of annual leave).
Immunological testing: specific IgE and SPT
If detected, a positive SPT or elevated level of specific IgE antibodies to a workplace allergen confirm sensitisation, but not the presence (or definite future risk) of OA.1 Their diagnostic utility for OA is greater for HMW allergens with a clear immunological mechanism (eg, enzymes, laboratory animals, latex and wheat flour), where sensitivity and specificity are each around 0.7.49 Specific IgE tests are also available for a limited number of LMW agents (eg, acid anhydrides and isocyanates) and, when present, have high specificity (0.89) for diagnosis.49
Spirometry
All patients with suspected OA should have their PEF, FEV1 and forced vital capacity (FVC) measured and interpreted according to international guidelines.50 Measured values are commonly within normal limits, but in some cases, bronchodilator testing confirms reversible airflow obstruction. In addition to its diagnostic value, spirometry is also important to provide a baseline for future monitoring, and to use as a prognostic indicator.20 51
Cross shift changes in FEV1 have previously been investigated as a diagnostic tool in OA, but the available evidence points to this being an insensitive approach.52 Where available, the pattern of previous spirometry results (often from health surveillance) can be more informative, for example, if there has been progressive deterioration in FEV1, followed by marked improvement, that can be clearly linked to a reduction in exposure.
Fractional exhaled nitric oxide and sputum eosinophils
Measuring airway inflammation with markers such as fractional exhaled nitric oxide (FeNO) or induced sputum eosinophil counts has an established role in the assessment of patients with suspected asthma,2 53 but normal levels may be found in a proportion of patients with OA.1 2 Limited data support their use in assessing the inflammatory responses after SIC testing,54 with a rise in FeNO occurring later (at ~24 hours) than that seen for sputum eosinophils (at ~6 hours). Such tests are more useful with OA due to HMW agents, as LMW chemicals are less likely to cause eosinophilic disease.55 56
The role of serial measures of airway inflammation, comparing periods at and away from work, has also been investigated in a small number of studies.57–59 In one of these, a greater than 1% work-related rise in sputum eosinophils was found to have a sensitivity of 65% and specificity of 76% for diagnosis, when compared with SIC.59
Further studies are required to establish the role of tests of airway inflammation in OA diagnosis, and practical logistic issues may limit their availability.
Non-specific bronchial hyper-responsiveness testing
Single measures of airway reactivity using, for example, mannitol or histamine inhalation, are well-established diagnostic tests for asthma but have a relatively low sensitivity (36–64%) for OA diagnosis,1 as in some cases of early disease, airway reactivity fully resolves within a few days of being off work. The test is most useful, therefore, in symptomatic workers with recent exposure (ie, tested within a few hours of leaving work), where the absence of non-specific bronchial hyper-responsiveness (NSBHR) makes OA very unlikely.60 Limited data suggest that the overall diagnostic sensitivity of NSBHR testing may be improved by the addition of FeNO and sputum eosinophil measurements.61
Serial measures of airway reactivity (often over periods of work and rest, or pre-SIC and post-SIC) may also be used in investigating OA, although the evidence to support their use is confounded by many methodological factors.2
Specific inhalation and workplace challenge
Although specific inhalation54–56 and workplace challenges62–64 are important diagnostic tests in OA, these specialised techniques are not widely available in the UK, and most patients are diagnosed from the results of other investigations.1 More information about challenge testing is provided in online supplemental Appendix 4.
Further sources of information
Specialist centres may offer to undertake workplace visits, often arranged with help from the occupational health provider, but these are time consuming and require both the consent of the patient and the permission of the employer. Information may be more readily available from employer websites or photos and video clips that patients have taken on their mobile phone. Material Safety Data Sheets (see Appendix 2) are readily available on the internet or via a patient’s employer; substances containing known respiratory sensitising agents should be given a health hazard label ‘H334’ (formerly R42).
Clinical practice points
Many patients with OA in the UK are diagnosed at a late stage; healthcare professionals should be aware of the important benefits of recognising cases early.
All patients of working age with new symptoms suggestive of asthma, reappearance of childhood asthma, deteriorating asthma control or unexplained airflow obstruction should be asked about their job, and whether their symptoms are the same, better or worse on days away from work (eg, rest days or holidays).
Symptomatic asthma patients in high-risk jobs, and those reporting improvement away from work, should be referred as quickly as possible for specialist assessment (where possible, directly to a specialist occupational lung disease service).
A diagnosis of OA has important health and employment implications and should not be made based on a compatible history alone.
The diagnosis of OA is most easily made prior to workplace adaptations and starting maintenance treatment.
Objective tests commonly used in the UK include SPTs, specific IgE antibody levels and serial measures of PEF or airway responsiveness; workplace and SICs are less commonly required for OA diagnosis.
Section 4 management
Managing OA is a form of precision medicine,65 aiming to attain the best balance between long-term health and employment outcomes for each individual patient. Careful consideration must be given to demographic, medical and workplace factors (table 3) that vary between patients, and often change in importance over the course of the illness. Figure 4 shows a summary of the key aspects of OA management.
Summary of factors influencing management of OA

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagram summarising the key elements of OA Management. *Liaison with occupational health (OH) or the employer and contacting the Health and Safety Executive (HSE) require patient consent. +Management of any co-existing conditions including rhinitis, breathing pattern disorder, inducible laryngeal obstruction (ILO), anxiety and depression.
Medical management
The pharmacological treatment of OA is the same as that of asthma unrelated to work and should follow national guidelines.2 53 Treatment regimens and action plans need to be flexible, to allow for the marked variability in symptoms that may occur between periods at and away from work, particularly with long absences (eg, holidays, furlough or sick leave). Few studies have specifically investigated the pharmacological treatment of OA, and those available have been limited by small sample size.66 67 Specific allergen immunotherapy has also been used in a small number of cases of OA with, at most, modest results, but the lack of available extracts, potential side effects, associated time commitments and costs limit its use.68 Biological therapies targeting immune pathways are increasingly used in the management of severe asthma, but the current published evidence in OA is limited to case reports of the use of omalizumab.69–71
In addition to asthma management, smoking cessation is important, and patients should also be treated for related conditions that may coexist with OA, including occupational rhinitis, breathing pattern disorder, ILO, anxiety and depression.35 36 72
Workplace interventions to prevent (or reduce) exposure to the cause
After making a diagnosis of OA, clinicians have a key role in educating patients about the nature of their condition and the likely long-term health outcomes that may occur if they remain exposed in the workplace.73 In addition, experienced OA specialists will explore the individual’s preferences and work circumstances, to discuss whether it is likely that the patient’s work could be adapted to prevent or substantially reduce exposure to the causal agent. For many patients, where non-exposed work roles are not available, receiving standard asthma medication and remaining employed in a role with the same or reduced levels of exposure offers a more acceptable compromise than long-term unemployment.
Respiratory protective equipment (RPE) is often seen as a simple and cheap solution to prevent further exposure for patients with OA but is the least effective control measure (figure 2). Although there are no large studies of long-term outcomes, the use of an air-fed helmet respirator may allow some workers with OA to remain at work with continued exposure to the causative agent.1 74
The advantages and disadvantages of potential employment options are summarised in online supplemental Appendix 5.
Liaison with occupational health/employers
An employer has a duty under the Equality Act 2010 (see online supplemental Appendix 2), to make reasonable adjustments for employees with disability due to OA, and communication with the workplace is usually necessary to facilitate this. All patients have a right to confidential medical care, however, and where workers expressly state that they do not want their employer to be contacted, often due to concerns about their job security, this should be respected.
Any communication requires explicit consent (preferably in writing) and patients should have the opportunity to comment on the factual content of letters or medical reports prior to their being sent. In general, communication is easier, and outcomes are often better, where access to an occupational health service is available.18
Following written notification of a diagnosis of OA in one of their employees, British employers are legally obliged under Reporting of Injuries, Diseases and Dangerous Occurrences Regulations (RIDDOR)75 (see Appendix 2) to report the case to the Health and Safety Executive (HSE). In addition, a review of existing control measures and a survey of the health of other exposed workers should both be undertaken (COSHH regulations).15
Benefits and compensation advice
In the UK, patients with OA are eligible to make a claim for IIDB.76 This is a statutory benefit payable, without consideration of fault, to employed earners who have acquired a ‘prescribed’ workplace disease such as OA due to sensitisation. Claims can be made online or by post and are followed by a face-to-face assessment by an appointed doctor who will confirm (or otherwise) the diagnosis. Only those judged to have a disability ≥14% are awarded benefit for OA; around half of claims are successful in this respect.
Patients with OA may also wish to make a legal claim in civil law against their employer for a ‘personal injury’34; this is best done with the advice of an experienced solicitor and patients who are members of a Trade Union can seek advice through their local representative. Patients should be advised that claims for personal injury are subjected to a statute of limitations and must be submitted within 3 years of knowingly having the problem.
Communication with patients
Patients with a confirmed diagnosis of OA should be given a clear explanation of their condition, ideally confirmed in writing, include the likely health consequences of ongoing exposure, and the implications for future employment.1 73 Letters should also include advice relating to relevant benefits and compensation patients may wish to explore.
Follow-up
While there is potential for on-going exposure to the cause, patients with OA should have regular follow-up in a specialist clinic indefinitely, to monitor asthma control, medication requirements and annual FEV1 decline. Repeating serial peak flow monitoring after workplace adjustments can also be valuable for monitoring purposes, with loss of previously noted work-related variability being reassuring.
Depending on severity, patients who are no longer exposed but have persistent asthma symptoms can be managed in general practice, non-specialist respiratory clinics or a severe asthma service.
Reporting cases to the national surveillance scheme
All respiratory physicians are encouraged to report anonymised cases of OA to the national Surveillance of Work-related and Occupational Respiratory Disease (SWORD) (see Appendix 2) scheme that is funded by the HSE and run through the University of Manchester. HSE reviews the annual data collected to analyse trends in causation,8 77 to identify relevant industry sectors that may benefit from future research or inspection campaigns.
Clinical practice points
Managing patients with OA can be complex and should wherever possible be carried out by a physician with specialist expertise in this condition.
It is important to educate patients with OA that the best opportunity for improved asthma control comes from early, and complete, cessation of exposure to the cause.
Management of OA includes standard pharmacotherapy, asthma education and smoking cessation advice, following national guidelines.
Patients with OA may have coexisting and related conditions (eg, occupational rhinitis, breathing pattern disorder, ILO, anxiety and depression) that require assessment and treatment.
Clinicians should work in partnership with patients to develop (and adapt as necessary) a personalised management plan aiming for the best possible balance between long-term health and employment outcomes.
Where consent is given, liaising directly with occupational health providers and/or employers gives the best chance of suitable workplace adaptations being made, to keep patients and their coworkers safely employed.
Patients with OA should be provided with written information confirming their diagnosis, the implications this has on their current and future jobs as well as IIDB and civil compensation advice.
While there is potential for ongoing exposure to the cause, patients with OA should remain under specialist follow-up to monitor asthma control, lung function and the impact of any workplace interventions.
Section 5 prognosis
Although there is the potential for OA to fully resolve if managed early enough,73 in reality most patients develop chronic asthma, with around one in six meeting criteria for severe disease.78 Patients with OA have a high risk of anxiety, depression and impaired quality of life, due to the combination of long-term ill health and associated adverse socioeconomic outcomes.18 79 80
Whatever methodology is used to attain a diagnosis, prognosis in OA is largely determined by two main factors, relating to the duration and level of exposure to the cause.1 2 73 81–83 Longer delays in case recognition, with more prolonged periods of symptomatic exposure, adversely affect prognosis, resulting in increased asthma severity at the time of diagnosis (as evidenced by the degree of airflow obstruction, the level of NSBHR, and, where available, the magnitude of fall in FEV1 seen at SIC).
Following confirmation of the diagnosis, the second main prognostic factor relates to the degree of ongoing exposure to the cause. If complete cessation is possible, 25%–30% of patients can expect a full recovery over a 3–5-year period, and another 30%–35% will report a reduction in asthma symptoms with treatment.73 Clinical improvement is mostly seen in the first 2 years but may continue at a slower pace over a longer period.84 Although the underlying mechanisms responsible remain to be established,61 the remaining patients do not get better despite completely avoiding the cause, and, in some cases asthma severity progresses despite good compliance with appropriate medication.
Unfortunately, workplace interventions resulting in total cessation of exposure carry the greatest risk of job loss, with over half being out of work 3–5 years postdiagnosis.73 Although the prospect of a good health outcome is lower for those who remain at work with reduced exposures (eg, from relocation to a lower exposure role, or use of RPE), a recent meta-analysis found the chances of remaining in employment to be ~14–15 times greater than for workers who had completely ceased exposure.73
For workers who continue in the same job, exposed without adaptations, OA clinical outcomes are usually worse, with the majority (~80%) reporting no improvement or worsening of symptoms, despite treatment.73 These patients are also at an increased risk of accelerated lung function decline (on average ~100 mL/year), which may result in a degree of fixed airflow obstruction.51
A summary of prognostic factors in OA is provided in table 4.
Prognostic indicators in OA
Clinical practice points
Around one in six patients with OA meet established criteria for severe asthma.
Prognosis in OA is largely determined by asthma severity at the time of diagnosis, and whether workers continue to be exposed to the cause thereafter.
Around 25%–30% of OA patients who permanently cease exposure will make a full recovery, and another 30%–35% will report a reduction in symptoms with treatment.
Patients with OA who remain exposed to the cause are at risk of accelerated lung function decline, which may result in a degree of fixed airflow obstruction.
Patients with OA have an increased risk of unemployment, with approximately one in three being out of work 3–5 years after diagnosis.
Anxiety and depression are common in OA, affecting up to half of patients.
Online appendices
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
References
Footnotes
Contributors All authors were responsible for the drafting and review of the document. The corresponding author, CB, was responsible for final approval of the manuscript. CB—drafting, review and final approval. PC—drafting and review. JF—drafting and review. DF—drafting and review. JH—drafting and review. HM—drafting and review. GIW—drafting and review.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer A Clinical Statement reflects the expert views of a group of specialists who are well versed on the topic concerned, and who carefully examine the available evidence in relation to their own clinical practice. A Clinical Statement does not involve a formal evidence review and is not developed in accordance with clinical practice guideline methodology. Clinical Statements are not intended as legal documents or a primary source of detailed technical information. Readers are encouraged to consider the information presented and reach their own conclusions.
The contents of this publication express the views of the authors, and not necessarily of HSE policy or policy makers.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.