Article Text

Statistics from Altmetric.com
Clinical case
Maria Luisa Nicolardi (specialty respiratory fellow)
A 19-year-old male smoker presented in the emergency room after accidental aspiration of an unquantifiable amount of Pyrofluid, a liquid mixture of high-boiling aliphatic/paraffin aromatic free hydrocarbons, during a fire-eating performance. A few minutes after the aspiration he started to feel sick, with shortness of breath and mild dry cough. On admission to our hospital, he had an episode of emesis and presented burning retrosternal chest pain and dyspnoea. Physical examination revealed oxygen saturation (SpO2) on ambient air of 92%, tachypnoea, tachycardia, normal temperature. Chest auscultation showed the presence of breath sounds without additional pathological sounds. The rest of the systemic examination was normal. Oropharyngoscopy was negative for oral lesions. Laboratory exams showed a neutrophilic leukocytosis (white cell count (WCC) 15.56×109/L, neutrophil 10.91×109/L), without increased C reactive protein (CRP) levels. Arterial blood gases on room air revealed PaO2 8.9 kPa, PaCO2 5.5 kPa, pH 7.30, (HCO3-) 20 mmol/L, (Lac) 3.8 mmol/L, and PaO2/inspired oxygen fraction (FiO2) 42.4 kPa. Chest X-ray demonstrated mild accentuation of the broncho-vascular structure with a consolidation in the left basal area (figure 1A). High-resolution chest CT (HRCT) showed bilateral parenchymal consolidation involving most of the inferior lobes and a complete occlusion of the lower lobar bronchus bilaterally; moreover, fluid-dense effusion was present in the right basal area (figure 1B). Although blood cultures and microbiological tests on sputum were negative, a broad-spectrum antibiotic therapy was initiated with piperacillin/tazobactam. The patient was also treated with systemic steroids, analgesics and oxygen therapy via a Venturi mask at FiO2 of 0.4.
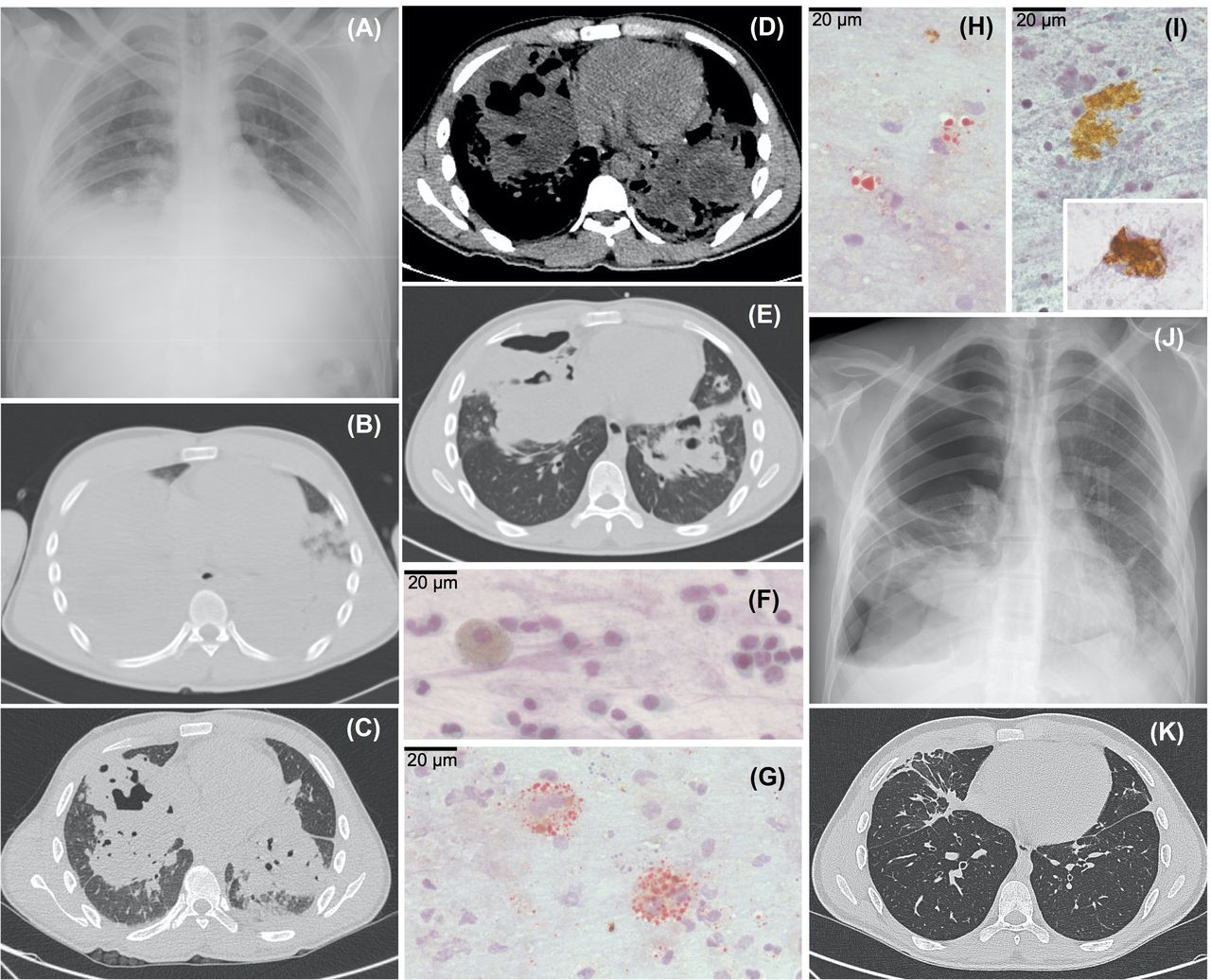
(A) Chest X-ray, day 1; (B) High-resolution chest tomography (HRCT), day 1; (C) HRCT, day 10; (D, E) HRCT, day 23; (F, G, H, I) cytological examination on sputum (magnification ×600; scale bar 20 μ), day 23; (J) chest X-ray, day 25; (K) HRCT, day 90. See text for comments.
On day 2, as arterial blood gases status worsened, cycles of high flow nasal cannula and non-invasive ventilation (NIV) were administered. In addition, bronchodilators, teicoplanin and fluconazole were added to therapy. As a result, clinical stability was achieved in the next days.
On day 8, the patient was transferred to our pulmonology ward. On admission, he had chest pain and dyspnoea, SpO2 was 97% while receiving FiO2 0.6. On lung auscultation, a reduction of breath sounds and diffuse crackles were heard.
Alessandra Oliva (infectious disease consultant)
On day 10, I was called for counselling because the patient was feverish (temperature >38°C), with dry cough and dyspnoea persisting. Blood examinations showed neutrophilic leukocytosis (WCC 23.57×109/L, neutrophil 21.31×109/L) and elevated CRP (112.200 µg/L, upper limit of normal 6.000 µg/L). Microbiological tests showed a positive nasal swab for methicillin-resistant Staphylococcus Aureus, positive blood cultures for Staphylococcus haemolyticus and positive Aspergillus galactomannan in the sputum. I then prescribed a targeted therapy with linezolid in addition to broad spectrum piperacillin/tazobactam and isavuconazole.
Giorgio Maria Masci (radiology consultant)
On day 10, a new HRCT was obtained showing a reduction of parenchymal consolidation of the right lower lobe, but persistence of left lower lobe consolidation with multiple cavitation (ie, pneumatocele) (figure 1C). Similar findings were observed in the middle lobe and in the lingula, together with small pseudonodular thickenings in the subpleural area and fibrotic striae at the bases. Parenchymal consolidations were characterised by polycyclic areas of fat-fluid density (eg, Housfield units from 0 to −50) highly suggestive of lipoid pneumonia (figure 1D). A small amount of pleural effusion at the left lung base and pericardial effusion were also found. No lymphadenopathy was observed. These findings are compatible with a complicated pneumonia, with a possible lipoid component, related to aspiration of hydrocarbons.
Maria Luisa Nicolardi (specialty respiratory fellow)
In the following days, the patient reported progressive reduction of dyspnoea and chest pain, but persistence of dry cough. Diffuse crackles at lung auscultation were unchanged, while arterial blood gases status progressively improved and oxygen supplementation was progressively reduced. Laboratory exams showed normal cell count and a reduction in CRP level. Antibiotic and antifungal therapy was continued.
On day 23, the patient’s clinical condition suddenly worsened: he was pyretic (temperature 39.5°C) with productive cough with dark and bloody sputum. Lung HRCT and sputum examination for microbiology and cytology were scheduled.
Alessandra Oliva (infectious disease consultant)
Microbiological and culture tests on sputum were positive for Enterobacter cloacae, Stenotrophomonas maltophilia, Serratia marcescens; in addition Aspergillus galactomannan index was positive. Blood cultures were negative. Blood laboratory exams showed leucopenia (WCC 1.23×109/L, neutrophil 0.30×109/L, lymphocytes 0.69×109/L) and a mild increase in CRP level. As a result, I decided to switch antibiotic therapy to meropenem, ciprofloxacin and vancomycin and to continue isavuconazole.
Giorgio Maria Masci (radiology consultant)
On day 23, a chest CT scan showed moderate reduction of the consolidations of the middle lobe and left lower lobe, with persistence of the lipoid content and partial reduction of pneumatoceles. Bilateral pneumothorax was also present, more evident at the anterior base of right lung (figure 1E).
Valeria Ascoli and Niccolo’ Noccioli (histopathology consultants)
Sputum sent on day 23 appeared brownish in colour. Alcohol-fixed, papanicolaou-stained smears showed abundant cellular debris in the background associated with finely vacuolated macrophages, neutrophils, lymphocytes and bronchial cells with regressive changes, devoid of cilia (figure 1F); there were also sheets of metaplastic bronchial epithelium. Air-dried, Oil-red-O stained smears showed profuse extracellular lipid droplets of different size with macrophage uptake of lipids (lipophages) (figure 1G,H). Extracellular and intracellular crystal-like aggregates of an undefined amorphous dark-yellow pigment were seen in the background and within macrophages (figure 1I).
Maria Luisa Nicolardi (specialty respiratory fellow)
On day 25, the patient complained of severe acute chest pain, exacerbated by breathing and cough, with desaturation (SpO2 92%, on FiO2 0.28), tachypnoea and tachycardia. On chest auscultation a reduction of breath sounds in the right hemithorax was audible. Chest X-ray revealed a right side pneumothorax, extended from apex to the base (figure 1J). A thoracic surgical consultation was requested.
Sara Mantovani (chest surgery consultant)
On my arrival, the patient presented an extensive pneumothorax that required pleural drainage. After informed consent, a chest drain (12 French) was placed into the 4th intercostal space along the right mid-clavicular line. The chest drain was left in suction for a few days, with drainage of air and haematic pleural effusion. After 1 week, the chest X-ray showed complete pneumothorax resolution and the chest drain was removed.
Maria Luisa Nicolardi (specialty respiratory fellow)
One month after admission, the patient’s clinical condition had gradually improved. Productive cough decrease, and dyspnoea and chest pain resolved. Inflammatory indexes and microbiological tests were negative. A new HRCT proved a further reduction of the two consolidations of the middle lobe and left lower lobe . Antibiotics and oxygen therapy were suspended. The patient was discharged after 40 days, with a clinical and radiological follow-up planned.
Three months after aspiration of Pyrofluid, the patient no longer have any symptoms. SpO2 was 100% on room air. On lung auscultation, breath sounds were normal. HRCT showed: ‘an almost complete resolution of middle lobe and left lower lobe consolidations and no pneumatoceles; new onset of fibrocicatricial striae of connection with the pleura and some small traction bronchiectasis; absence of pneumothorax, pleural and pericardial effusion and lymphadenopathy’ (figure 1K). On spirometry, lung volumes were within the normal range.
Discussion
Paolo Palange (chief respiratory division)
This is a description of a very severe fire eater's lung (FEL) admitted for hypercapnic respiratory failure requiring oxygen supplementation during NIV. In addition, our clinical case clearly depicts the possible fatal complications of FEL and how they should be treated. It also provides evidence that, in young subjects, the lung has the ability to regenerate after severe FEL with complete recovery of lung structure and function within 3 months from acute injury.
FEL is an acute exogenous lipoid pneumonia caused by aspiration into the airways of liquid hydrocarbons. High volatility, low viscosity and low surface tension that characterise these hydrocarbons causes a rapid diffusion in the bronchial tree, a destruction of the surfactant barrier and cellular membranes associated with a decrease in lung compliance. Lipoid materials are not metabolised by tissue enzymes but induce emulsification and subsequent phagocytosis from macrophages, as seen in our case with numerous lipophages and abundant extracellular lipids (figure 1G,H). We also noticed intra/extracellular dark-yellow pigment that probably represents a substance mixed with liquid hydrocarbons (figure 1I). The alveolar macrophage activation together with cytokine release triggers a prolonged inflammatory response. The lipids may remain within the macrophages for a long time but after their lysis are released back into the alveoli. This lipid release may trigger a giant-cell response and lead to fibrosis.1–3
Clinical manifestation usually occurs in the first 12 hours after aspiration and can vary from mild to life-threatening, depending on the amount of fluid aspirated. In a review of 123 patients with FEL, the vast majority with mild to moderate disease (mean duration hospitalisation 11 days in 18 patients out of 123), the most frequently symptoms observed included dry cough, chest pain, dyspnoea and fever2; haemoptysis, myalgia, nausea and emesis may also be present.1–4 Chest auscultation may reveal crackles, and blood tests show neutrophil leucocytosis and high CRP levels. Radiologic manifestation at 12–24 hours after aspiration show unilateral or bilateral ground glass opacities and consolidation areas that frequently involve the middle lobe or the lower lobes.1–3 Possible complications of FEL are pneumatoceles, widespread lung consolidation, superinfections, abscesses, pleural effusion, bronchopleural fistula, pneumothorax and adult respiratory distress syndrome.2 3
The optimal treatment of FEL has not yet been established, particularly in severe cases. Early antibiotic therapy may be justified, also considering that clinical, laboratory and radiologic findings of FEL overlap with bacterial pneumonia. Moreover, it seems that the severe form of FEL has a good prognosis if superinfection can be prevented. As reported in the literature, systemic corticosteroids can be administered in severe cases to limit the inflammatory response and fibrosis.2 3 Inhalation of large amounts of hydrocarbons can lead to a severe respiratory distress that requires mechanical ventilation.3 Surgical resection is usually unwarranted as lipoid pneumonia may regress spontaneously; surgery, however, can be useful in the management of complications.
Importantly, our case demonstrates that, despite the severe initial presentation, FEL usually has a favourable resolution, and ‘restitutio ad integrum’ can be obtained between a few weeks and 3 months from injury,1 4 and that the overall mortality rate is less than 1%.3 In this respect, recent studies provide evidence that young adults have a great ability to regenerate lung tissue and that lung repair capacity declines with ageing.5
Finally, our observation demonstrates that in severe FEL a long-term follow-up is necessary, because several complications may occur particularly within the first month of the disease. Also, we strongly encourage a conservative attitude, as the lung can show a complete regeneration even if the initial damage is extensive (figure 2).

{kind=link}
{kind=link}
Fire eater in action.
Ethics statements
Patient consent for publication
Footnotes
Contributors All authors acted as consultants in the clinical case described and edit end review the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves