Article Text

Abstract
Background No data on healthcare utilisation and associated costs for the many rare entities of children’s interstitial lung diseases (chILD) exist. This paper portrays healthcare utilisation structures among individuals with chILD, provides a pan-European estimate of a 3-month interval per-capita costs and delineates crucial cost drivers.
Methods Based on longitudinal healthcare resource utilisation pattern of 445 children included in the Kids Lung Register diagnosed with chILD across 10 European countries, we delineated direct medical and non-medical costs of care per 3-month interval. Country-specific utilisation patterns were assessed with a children-tailored modification of the validated FIMA questionnaire and valued by German unit costs. Costs of care and their drivers were subsequently identified via gamma-distributed generalised linear regression models.
Results During the 3 months prior to inclusion into the registry (baseline), the rate of hospital admissions and inpatient days was high. Unadjusted direct medical per capita costs (€19 818) exceeded indirect (€1 907) and direct non-medical costs (€1 125) by far. Country-specific total costs ranged from €8 713 in Italy to €28 788 in Poland. Highest expenses were caused by the disease categories ‘diffuse parenchymal lung disease (DPLD)-diffuse developmental disorders’ (€45 536) and ‘DPLD-unclear in the non-neonate’ (€47 011). During a follow-up time of up to 5 years, direct medical costs dropped, whereas indirect costs and non-medical costs remained stable.
Conclusions This is the first prospective, longitudinal study analysing healthcare resource utilisation and costs for chILD across different European countries. Our results indicate that chILD is associated with high utilisation of healthcare services, placing a substantial economic burden on health systems.
- paediatric interstitial lung disease
- paediatric lung disaese
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is the key question?
What are healthcare utilisation structures and crucial costs drivers among individuals with children’s interstitial lung diseases (chILD) across Europe?
What is the bottom line?
Healthcare resource utilisation and costs for chILD across different European countries indicate a high economic burden of the disease.
Why read on?
This first prospective, longitudinal study provides a pan-European estimate of per-capita costs and identifies the impact factors for costs of care.
Introduction
Children’s interstitial lung diseases (chILD), sometimes labelled diffuse parenchymal lung diseases (DPLD), cover many rare conditions that mainly affect the lung parenchyma, leading to impaired alveolar gas exchange. Aetiology and pathogenesis are broad. The leading clinical symptoms are tachypnoea, hypoxemia, retractions, crackles, and failure to thrive.1
Several studies have identified lower incidence and prevalence rates for chILD than for adult ILD. 2 Incidence and prevalence estimates vary across Europe. One study from UK and Ireland reported a prevalence of 0.36/100 000 children.3 In Germany, an annual incidence rate of 0.13/100 000 children has been calculated,4 whereas a much higher number has been published for Denmark with an incidence rate of 10.76/100 000.5 According to a recent study from Spain, the average incidence amounted to 0.82/100 000 per year; the prevalence was 4.65/100 000.6 Overall, chILD-related mortality is presumed to be around 15%, with deaths within the first 6 months of life being most common.4 7
The current categorisation system of chILD distinguishes between the following two groups: ‘A—DPLD disorders manifesting primary in infancy’ and ‘B—DPLD disorders occurring at all ages’. These are further subdivided into distinct categories and subcategories.1 8 However, recognition and diagnoses depend on the experience of a clinical centre. Thus, patients often go through a long diagnostic odyssey before receiving optimal care.9 So far, no evidence-based treatments or guidelines for any chILD are available.1 10 11
Data on healthcare resource utilisation or medical costs in chILD are sparse. Evaluation of resource utilisation can help understand healthcare needs, prioritise resource allocation for policymakers, identify key parameters in cost-effectiveness studies; it also indicates the need for new therapeutic strategies to reduce the socioeconomic burden of chILD.12–18
Methods
Kids Lung Register
The Kids Lung Register is a web‐based management platform collecting data of rare paediatric lung disorders with a focus on chILD.19 Implemented in 2015, the objective was to build a descriptive collection of chILD patients together with core biobank materials. The minimum data set includes demographics, disease descriptors, clinical examination, laboratory results, radiology and the conclusions of an international peer-review diagnostic team (www.childeu.net). Every physician can register as referring centre and include patients with a suspected diagnosis of chILD. Each case entered is reviewed by a multidisciplinary review board, consisting of radiologists, pathologists and clinicians with expertise in chILD to ensure diagnostic accuracy. The diagnoses of chILD are made in accordance with the clinical guidelines of the American Thoracic Society1 and the European management platform for interstitial lung diseases in children.8 Following this expert review process, the clinical course of the patients is longitudinally followed up at defined study visits taking place 6 and 12 months after inclusion and annually thereafter.
Study design and population
At the time of this study (early 2021), baseline data of 774 chILD patients were included in the Kids Lung Register. All centres including patient information in the chILD EU registry were invited to participate. The analysed economic data stemmed from a lung-specific modified version of the validated FIMA questionnaire20 21 that was tailored to healthcare needs of children (online supplemental file B). The questionnaire was available in eight languages (German, English, Turkish, Italian, Polish, Danish, Spanish and Hungarian). Patients whose caretakers spoke another language were excluded. Also, questionnaires with 10% or more missing values in reported utilisation outcomes were excluded.
Supplemental material
Healthcare utilisation and costs
In order to evaluate healthcare utilisation and costs, parents were asked to complete the questionnaire at each study visit with a follow-up period of up to 5 years postbaseline. Thus, all visits to various medical professionals (physicians and therapists), days of hospitalisation or rehabilitation, use of disease-specific medical aids, hours of (non-)professional caregiving, distances to healthcare institutions, days of accompaniment in clinics and productivity loss of caregivers during the 3 months prior to a study visit were systematically assessed. Healthcare utilisation patterns were monetarily valued using societal German unit costs22 updated via source research according to the base year 2015, the year of register implementation and their subsequent analysis stratified by country of treatment. Additionally, the type of pharmaceuticals used, frequency of intake and duration of administration were collected during the study visits and classified according to the Anatomical Therapeutic Chemical classification system.23 Most drugs stated at clinical visits were commonly available and inexpensive, but prices for the same pharmaceuticals varied widely.24 Thus, we chose to not include medication expenses in the final analysis, and only listed the drugs used.
Direct medical costs
Outpatient visits, healthcare professional visits, hospital and rehabilitation stays as well as care requirements accounted for direct medical costs. To avoid double counting, valuation of direct medical resources was limited to days on which the child was not admitted to the hospital. A table of cost units are found in online supplemental table 1a,b.
Supplemental material
Demographics and disease characteristics
Direct non-medical costs
Non-medical resource utilisation consisted of additional informal care, travel distances to healthcare institutions and days of accompaniment in hospitals or rehabilitation clinics. In order to calculate informal care costs, we offset informal care hours with reported hours of productivity loss to avoid double counting for informal care and indirect costs. Reported informal care hours were limited to a maximum of 16 hours per day.25 To calculate transportation costs, two-way travel distances covering the distance to hospitals and various medical professionals were multiplied by a flat rate of €0.30/km (travel flat rate by German tax law). The reported days of inpatient accompaniment were multiplied by €45.
Indirect costs (productivity loss)
For indirect burden of the disease, we collected information on parental productivity loss, including reductions in working hours and days of absence from work. For the assessment of indirect costs, we chose a human-capital approach, applying an average gross hourly wage to the reported hours of parental productivity loss assuming an 8-hour working day and an average gross salary of €17.59/hour to price days of absence.26 However, we did not assess the counter value of parents giving up their job to care for the child.
Statistics
For the descriptive analysis of the study population and healthcare resource utilisation, we calculated frequency and proportions as well as medians, means, IQR, SD or 95% CI. Non-normal distributed group differences (age at inclusion) were tested with the Kurskal-Wallis test. Utilisation patterns stratified by country of treatment and disease categories were described, since service provision and treatment decisions may differ. Countries with more than 10 participants (Germany, UK, Poland, Turkey and Italy) were analysed separately, whereas countries with less than 10 participants (Switzerland, Denmark, Hungary, Austria and Spain) were evaluated jointly with their pooled results reported as ‘other countries’. Unadjusted mean per capita costs were calculated in a 3-month interval. For children younger than 3 months cost calculations pertained to their age in days.
To generate a pan-European cost estimate, we applied a generalised linear model (GLM) with gamma distribution and log link, to account for the skewness of cost data.27 The model was adjusted for age in years, sex (male vs female), disease category (category A vs B) and country of treatment (Germany vs others). The latter covariate was due to the fact that, at baseline, over 50% of the patients were treated in Germany and that owing to the small sample sizes of the other countries, a nominal categorisation would have led to model non-convergence. To estimate mean direct medical costs, direct non-medical costs and total medical costs with their corresponding 95% CIs, we used a one-part GLM. Gamma models are only defined for positive values. Thus, a value of €1 was assigned to the few individuals without any costs to keep them in the analysis. Results were considered statistically significant if the p values were less than 0.05. Due to a large number of individuals with €0 indirect costs (56.7% of the sample), a two-part model was applied to estimate indirect costs.28 In the first part, the probability of incurring expenditures was predicted by a logistic model. In the second part, costs for individuals with non-zero costs were estimated using a gamma model. Due to the stepwise analysis, estimated total costs in the regression model do not equal the sum of estimated separate cost components. We considered results to be significant if the estimates of both models indicated the same direction and if at least one of the p values was less than 0.05.29
Supplementing the main analysis, we performed sensitivity analyses. We excluded children younger than 3 months (n=42) due to differences in the time span of cost calculation and repeated all performed regression analyses.
The statistical evaluation of the data was done using SPSS software for statistical analyses (V.26.0) and GraphPad Prism (V. 8.4.3).
Results
Study population
Four hundred and fourty-five patients from 10 European countries and 48 study sites were included. All but one questionnaire, which was entered incompletely into the register, were included in the final analysis. Median age at register inclusion was 3.8 (IQR 0.74–10.6) years, median time between chILD first suspected and baseline visit was 0.43 (IQR 0.03–5.4) years. There was no difference of age at register inclusion across countries (p=0.136). The spectrum of chILD categories and subcategories observed was broad. The majority of participants were allocated in the disease subgroup ‘A3—DPLD-infant conditions of undefined aetiology’ (21%), ‘A4—DPLD related to alveolar surfactant region’ (22%), and ‘B1—DPLD related to systemic disease processes’ (14%) (table 1) and mainly stemmed from Germany (n=239; 53.7%), followed by UK (n=80; 18.0%), Turkey (n=45; 10.1%), Poland (n=38; 8.5%) and Italy (n=19; 4.3%). This reflects the demographics of the entire registry (online supplemental table 2a–d).
Resource utilisation
Resource utilisation patterns at baseline and during follow-up are shown in table 2. During the observation period, outpatient visits, mostly general practitioners and paediatricians, and visits at healthcare professionals, mostly physiotherapists and psychologists, were frequent. Over two-thirds of the patients were consulting physicians with more than two outpatient visits per quarter. The high rate of hospital admission (62% at baseline, 35% at 6 months follow-up) and inpatient days (median 17 days at baseline and 5 days at 6 months) dropped substantially over time. Less than 5% of the patients were admitted to rehabilitation during the observation time. About two-thirds of the patients received medical aids. Most frequently used were devices for long-time oxygen therapy (66%), inhalation (41%) and pulse oximeters (45%). Most pharmaceuticals administered were systemic glucocorticosteroids (46%), macrolides (24%) or hydroxychloroquine (15%).
Resource utilisation per capita (assessment of 3-month interval before visit)
Costs of care (unadjusted)
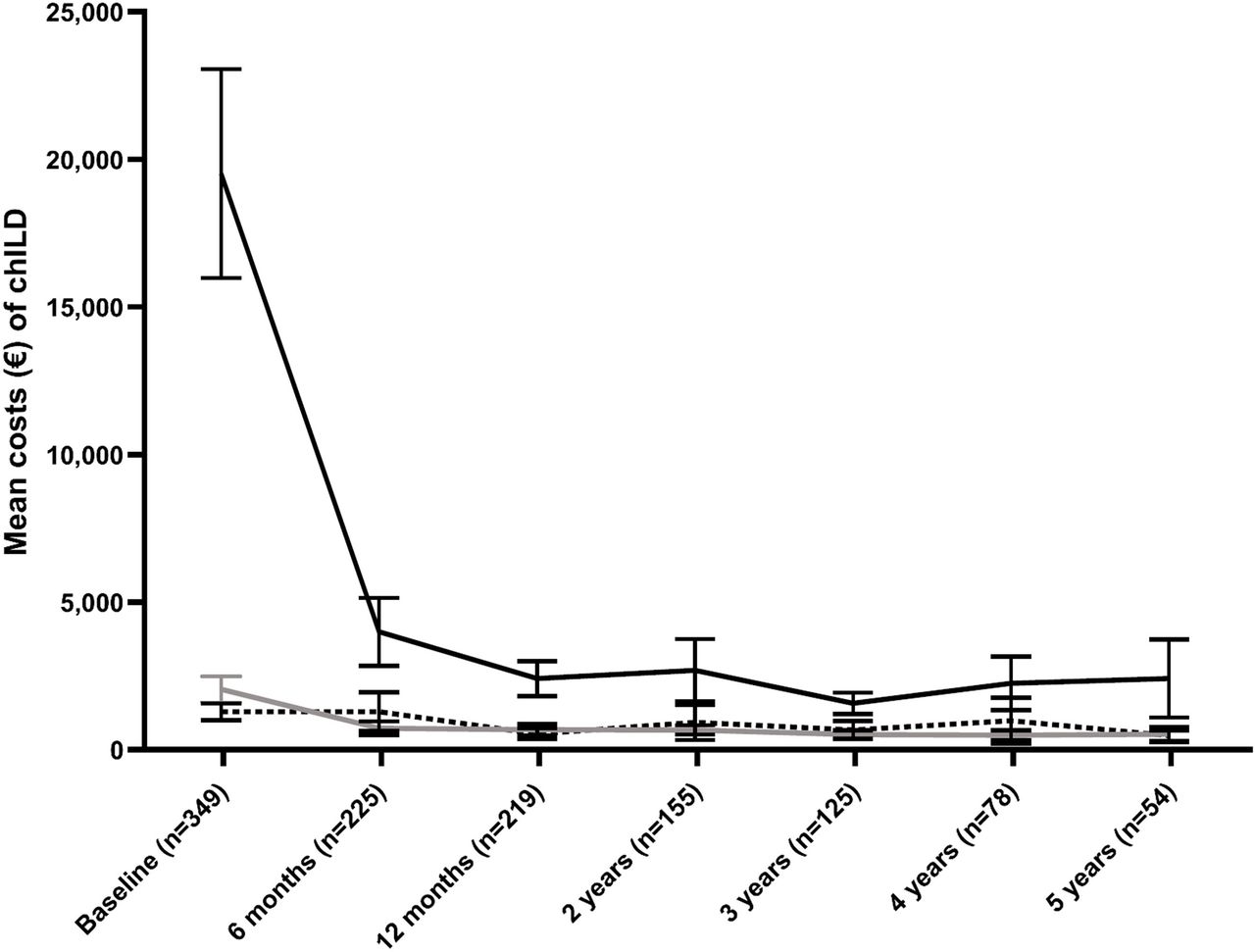
Direct medical costs were the most substantial cost component and stemmed from a high amount of hospitalisation expenses (figure 1, table 3). At baseline, direct medical costs (€19 818; 95% CI €16 187 to €34 448) were followed by indirect costs (€1 907; 95% CI €1 458 to €2 355) and direct non-medical costs (€1 125; 95% CI €873 to €1 412). Throughout the follow-up period, fewer hospital admissions were reported, and direct medical costs dropped compared with indirect costs and direct non-medical costs which remained almost stable (figures 1 and 2).

Mean total medical costs (and 95% CIs) in a 3-month interval for healthcare resource utilisation per patient at baseline and during follow-up. At baseline, most substantial were direct medical costs (€19 818; solid black line), followed by indirect costs (€1 907; solid grey line) and direct non-medical costs (€1 125; dashed black line). During follow-up, direct medical costs dropped substantially. chILD, children’s interstitial lung diseases.

Distribution of total medical costs in a 3-month interval for healthcare resource utilisation at baseline and during follow-up. During follow-up, direct medical costs (solid black bar) dropped compared with indirect costs (dashed black bar) and direct non-medical costs (solid grey bar).
Unadjusted mean (SD; range) of costs (€) in 3 months per capita
Costs at baseline stratified by country and disease (unadjusted)
The average country- and category-specific unadjusted costs are shown in figure 3, figure 4 and online supplemental table 3. The highest total medical costs (€28 788; 95% CI €14 628 to €42 970), direct medical costs (€24 493; 95% CI €12 757 to €38 228) and direct non-medical costs (€1 333; 95% CI €764 to €1 901) were found in Poland. These high direct medical costs were driven by high hospitalisation rates, whereas spending on outpatient medical care (€273; 95% CI €123 to €422) was rather low. The highest indirect costs were observed in Italy (€2 832; 95% CI €370 to € 5 294). In Turkey, there were no costs for informal care at all.

Mean total medical costs (direct medical costs: solid black bar, direct non-medical costs: solid grey bar, indirect costs: dashed black bar) in a 3-month interval of chILD stratified by country at baseline. Error bars indicate SD of total medical costs. chILD, children’s interstitial lung diseases.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mean total medical costs (direct medical costs: black bar, direct non-medical costs: grey bar, indirect costs: white bar) in a 3-month interval of chILD stratified by category at baseline. Error bars indicate SD of total medical costs. chILD, children’s interstitial lung diseases.
The model-based pan-European cost estimate was €22 849 (95%CI €19 216 to €27 169). Direct medical costs were estimated at €19 818 (95%CI €16 530 to €23 760), direct non-medical costs at €2 862 (95%CI €2 115 to €4 073) and indirect costs at €1 907 (95%CI €1 008 to €1 647). The GLMs indicate a significant inverse association between age and estimated total costs (one-part model; estimate=0.899, p<0.001), direct medical costs (one-part model; estimate=0.822, p<0.001), non-medical costs (one-part model; estimate=0.931, p<0.001) as well as indirect costs (two-part model; estimate=0.891/0.981, p<0.001/0.088) (table 4). Treatment outside Germany was associated with significantly reduced total costs (one-part model; estimate=0.713, p=0.002). Having a chILD of category B was linked to increased total costs (one-part model; estimate=1.56, p<0.001) and direct medical costs (one-part model; estimate=1.77, p=0.014).
Influencing factors on costs of care at baseline
The results of the sensitivity analysis were in line with the main analysis while the magnitude of the estimates changed slightly, and impact of other countries on indirect costs was no longer significant.
Discussion
This is the first study analysing healthcare resource utilisation and costs for chILD across different European countries. We found that chILD was associated with a high utilisation of healthcare services. During the 3-month period prior to inclusion into the registry (baseline), mean per capita costs of care were substantial (€22 849), with the largest cost components being direct medical costs (€19 818). Over the years, direct medical costs dropped, but remained the largest cost component. These extraordinarily high healthcare costs presented at young age were mostly caused by (1) high hospitalisation rates (initial complex diagnostic workup and the time to establish therapy)30 and (2) the mortality effect (high costs before death and increased mortality rate in chILD within the first 6 months of life).4 7 However, as the epidemiology of chILD is not well characterised, one has to be cautious about making statements regarding how representative the Kids Lung Register cohort is. The results of this study cannot be used to estimate the overall economic burden in anyone’s jurisdiction.
Based on the observed utilisation patterns at baseline, we also provided a pan-European cost-estimate and identified the impact factors for costs of care. The results indicate that in chILD, the main cost driver was inpatient treatment. In countries with a relatively high hospitalisation rate like Poland, direct medical costs and subsequently total medical costs were particularly high. Outpatient care in Poland is mainly provided by general practitioners, who serve as gate keepers to specialised medical treatment and provide only a small range of services themselves. Thus, the management of chILD patients as inpatients reflects common practice of paediatric healthcare.31 32 However, in Poland, we found the highest rate of children diagnosed with ‘Persistent tachypnoea of infancy’. Depending on local policy, various diagnostic means may be used, including high-resolution CT, bronchoscopy or sometimes a lung biopsy, which may prolong the time as inpatient.33 Thus, we think that not merely the distribution of different diagnoses across the various countries, but the different healthcare structures and procedures used are causing cost disparities between different European countries.
Furthermore, chILD poses a burden on caregivers due to the additional informal care requirements and productivity loss. The absence of informal care effort in Turkey is particularly interesting. As such, there is a need to further assess informal care requirements, additionally considering the cultural and socioeconomic characteristics of observed countries.
The GLMs indicate a significant inverse association between age and estimated total costs as well as the separated costs components. This inverse association could mainly be caused by a more liberal admittance to hospital for surveillance of the younger children. However, our ability to generalise the significantly higher estimated average costs for children diagnosed with ‘DPLD disorders occurring at all ages’ (B categories) is limited, due to the unequal distribution of disease categories in our study sample and the heterogeneous clinical presentations.
Published data on healthcare service utilisation among chILD individuals are limited and no studies are available that systematically evaluate the economic burden of chILD on health systems and caregivers.34 Only one case report analysed the healthcare utilisation of a child with surfactant protein C deficiency. Until the age of 8 years and 10 months, the child had over 32 hospital admissions and spent 443 days in inpatient care.35
Data on healthcare costs of other rare paediatric disorders are scarce. A recent review systematically analysed the medical costs of rare diseases.17 Direct medical expenses over a 3-month period for Fragile X syndrome and Niemann Pick disease were reported to be about €7 76336 and €12 486, respectively.37 Most data concern healthcare utilisation of cystic fibrosis (CF), the most frequent paediatric autosomal recessive disease in Caucasian population,38 with respiratory failure being the primary cause of morbidity and mortality.39 For CF direct medical costs over a 3-month interval ranged from €1 777 to €12 889 per capita.40–42 In chILD, the profile of high-cost accumulation in infancy which then subside is inverse to that in CF with rather low medical costs at younger age, which increase substantially over time and may result in even higher overall lifetime costs.42 43 However, comparing CF to chILD is a sensitive issue. In CF, medical costs are mainly driven by cost of outpatient drug prescriptions, accounting for almost half of the total medical costs.17 26 44 Also, the recent cost-intensive introduction of a causative treatment of CF with CFTR modulators may affect the longitudinal healthcare resource utilisation.42 In chILD, however, no specific treatments are established and among the 20 most cost-intensive drugs listed for CF,42 only one treatment, inhaled sodium chloride, is commonly used in chILD. It has to be noted that the analysed base year of some of the previously mentioned studies dates back more than 10 years and the inflation of medical costs compared with chILD is underestimated. Furthermore, when comparing analyses of healthcare costs of different diseases and studies, one must consider various biases including different data sources and cost calculations.45
There are several limitations to interpreting these findings. First, this is not a population-representative study. Severe diagnoses or prolonged clinical courses could be over-represented. As mild manifestations might not be reported to referring centres and be disregarded in the analysis, mean costs might be overestimated. Second, although all but one questionnaire were completely filled out, economic data of only about half of the patients included at baseline were entered into the register. This could limit the external validity. Also, we did not monitor compliance to fill out questionnaires. However, since the distribution of diagnoses in the categories and subcategories was the same across patients with and without questionnaires entered, we believe that there was no systematic bias. Third, we used self-assessment questionnaires with the request to recall the healthcare utilisation of the last 3 months. By recalling healthcare utilisation in the last quarter and not annually, the analysis might be more influenced by singular events, like hospitalisation or the lack of corresponding events. However, this reduces the memory-bias and telescoping effects as it is more difficult to correctly remember events that date back to earlier points in time. Fourth, owing to convergence issues, our model reflected country binary coded. Therefore, heterogeneous structures in the pooled sample of countries other than Germany were treated on a par and potential non-uniform associations were disregarded. The pan-European cost estimate does not fully address country-specific cost structures and the non-random variability in the population. Fifth, although the total number of children with rare diseases like chILD is rather large, only a small proportion across single diagnoses and countries could be analysed, and estimates of medical costs were heavily influenced by single outliers. Sixth, some components of therapy might differ by country and specific medical treatments might not be included in the prices for hospital treatment. Also, our sample consisted of individuals with heterogeneous disease characteristics, resulting in different care needs. Finally, the analysed countries have different healthcare systems, with differing access to and coverage of healthcare services, which might influence healthcare utilisation and thereby cost structures. As stated above, we chose not to include medication expenses in the final analysis. For an earnest cost calculation of pharmaceutical expenses, future studies might include claims data (eg, from sickness funds) as done before.42
Overall, this is the first comprehensive assessment and analysis of healthcare resource utilisation to evaluate the economic burden of chILD among European countries. Results indicate that chILD is associated with a substantial economic burden. The development of standardised diagnostic approaches and new therapeutic strategies might reduce the economic burden of chILD.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Ethics Commission at the Ludwig Maximilians University of Munich, Pettenkoferstr. 8, 80336 München (EK 026‐06, 257‐10, 111‐13, 20‐329). Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
LS and MG are joint senior authors.
LS and MG contributed equally.
Collaborators The chILD-EU collaborators are Tugba Sysmanlar, Ayse Aslan (Ankara Gazi University, Turkey), Susanne Zeidler (Asklepios Sankt Augustin Krankenhaus, Germany), Veronika Baumeister, Folke Brinkmann (Bochum Ruhr Universität, Germany), Isabelle Rochat (Centre hospitalier universitaire vaudois Lausanne, Switzerland), Sebastian Becker (Darmstädter Kinderkliniken, Germany), Claudia Eismann, Meike Köhler, Dörthe Neuner, Andrea Schams, Waltraud Wesselak, Sabine Witt, Matthias Kappler, Mandeep Kaur (Dr. von Hauner Children’s Hospital, University Hospital LMU Munich, Germany), Silvia Castillo Corullón (Fundación de Investigación del Hospital Clínico Universitario de Valencia, Spain), Lale Bayir, Nagehan Ciftci (Hannover Medical School, Germany), Hildegard Seidl (Helmholzzentrum Munich, Germany), Lauren McCann (Imperial College London, United Kingdom), Chiara Carolina Abbas, Tobias Ehrenreich, Philipp Latzin (Inselspital Bern, Switzerland), Ayse Aizit Kilinc (Istanbul Cerrahpasa University, Medicine Faculty Hospital, Turkey), Tobias Hübner, Holger Köster (Kinderklinik Oldenburg, Germany), Martin Schebek (Klinikum Kassel, Germany), Matteo Fontana, Nicolas Regamey (Luzerner Kantonsspital, Switzerland), Stanislaw Boguslawski, Honorata Marczak (Medical University of Warsaw, Poland), Deborah Adelsberger (Oldenburg Zentrum für Kinder- und Jugendmedizin, Germany), Achim Freihorst (Ostalab Klinikum Aalen, Germany), Frederik Buchvald (Rigshospitalet Copenhagen, Denmark), Gemma Donohoe (Royal Children’s Hospital Manchester, United Kingdom), Morag MacLean, Fiona Redmond (Royal Hospital for Sick Children Edinburgh, United Kingdom), Cordula Koerner-Rettberg (Ruhr University-Bochum, Germany), Abigel Kolonics-Farkas (Semmelweis University, Hungary), Sarah Shortland (Sheffield Children’s Hospital, United Kingdom), Amy Collier (Southampton General Hospital, United Kingdom), Kathrin Seidemann (Städtische Klinikum Karlsruhe, Germany), Lutz Nährlich (Universität Giessen, Germany), Peter Meißner (Universität Ulm, Germany), Susanne Hämmerling, Benjamin Hanebeck (Universitätsklinikum Heidelberg, Germany), Dominik Schöndorf, Olaf Sommerburg (Universitätsklinikum Heidelberg, Germany), Winfried Baden (Universitätsklinikum Tübingen, Germany), Sune Rubak (University Aarhus, Denmark), Steve Turner (University Aberdeen, United Kingdom), Martin Rosewich, Johannes Schulze, Pera-Silvija Jerkic (University Frankfurt/Main, Germany), Christiane Lex (University Göttignen, Germany), Frans De Baets (University Hospital Gent, Belgium), Zsolt Szepfalusi (University Hospital Vienna, Austria), Edyta Glowacka (University Krakau, Poland), Freerk Prenzel (University Leipzig, Germany), Marijke Proesmans (University Leuven, Belgium), Nazan Cobanoglu (University of Ankara, Turkey), Florian Stehling (University of Essen, Germany), Gisela Anthony, Hans Rock (University of Marburg, Germany), Angelo Barbato, Deborah Snijders (University of Padua, Italy), Andrea Heinzmann (Universtätsklinikum Freiburg, Germany).
Contributors ES: processed the experimental data, performed the analytic calculations, designed the figures and took the lead in writing the manuscript. ES, MG, NS, JC, MW, SC, NE, NK, JL, KK, NU, DK handed out the questionnaires and entered the data into the Kids Lung Register. ES and MG conceived, implemented and planned the study. PM and LS helped in developing the methodology, data curation, formal analysis and verified the analytical methods. MG supervised the study and acquired the funding. NS, JC, MW, SC, NE, NK, JL, KK, NU, DK, MP, CG, LS and MG contributed to the final manuscript providing critical feedback. MG is the guarantor, accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Funding This work was supported by the European Register and Biobank on Childhood Interstitial Lung Diseases (chILD-EU register) funded by the European Commission under FP7-HEALTH-2012-INNOVATION-1, HEALTH.2012.2.4.4-2: Observational trials in rare diseases. MG is supported by DFG (Gr 970/9-1), FP7 Coordination of Non‐Community Research Programmes (Gr FP7‐305653‐chILD‐EU), Cost CA (16125 ENTeR-chILD) and European Respiratory Society Clinical Research Collaboration (CRC).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Author note Participants contributing less than 2% of the analysed health resource utilisation and medical costs are listed under the chILD-EU collaborators.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.