Article Text

Abstract
Rationale Dietary nitrate supplementation improves skeletal muscle oxygen utilisation and vascular endothelial function. We hypothesised that these effects might be sufficient to improve exercise performance in patients with COPD and hypoxia severe enough to require supplemental oxygen.
Methods We conducted a single-centre, double-blind, placebo-controlled, cross-over study, enrolling adults with COPD who were established users of long-term oxygen therapy. Participants performed an endurance shuttle walk test, using their prescribed oxygen, 3 hours after consuming either 140 mL of nitrate-rich beetroot juice (BRJ) (12.9 mmol nitrate) or placebo (nitrate-depleted BRJ). Treatment order was allocated (1:1) by computer-generated block randomisation.
Measurements The primary outcome was endurance shuttle walk test time. The secondary outcomes included area under the curve to isotime for fingertip oxygen saturation and heart rate parameters during the test, blood pressure, and endothelial function assessed using flow-mediated dilatation. Plasma nitrate and nitrite levels as well as FENO were also measured.
Main results 20 participants were recruited and all completed the study. Nitrate-rich BRJ supplementation prolonged exercise endurance time in all participants as compared with placebo: median (IQR) 194.6 (147.5–411.7) s vs 159.1 (121.9–298.5) s, estimated treatment effect 62 (33–106) s (p<0.0001). Supplementation also improved endothelial function: NR-BRJ group +4.1% (−1.1% to 14.8%) vs placebo BRJ group −5.0% (−10.6% to –0.6%) (p=0.0003).
Conclusion Acute dietary nitrate supplementation increases exercise endurance in patients with COPD who require supplemental oxygen.
Trial registration number ISRCTN14888729.
- exercise
- COPD pharmacology
- long term oxygen therapy (LTOT)
Data availability statement
Data are available upon reasonable request. Individual participant data that underlie the results in the article after de-identification (text, tables, figures and appendices) will be made available from the corresponding author upon request. The study protocol and statistical analysis plan will also be available. Data will be available indefinitely.
Statistics from Altmetric.com
Key messages
What is the key question?
Can dietary nitrate supplementation enhance exercise performance in individuals with a hypoxic COPD phenotype?
What is the bottom line?
In a double-blind, placebo-controlled, randomised cross-over study, an acute dose of dietary nitrate increased endurance shuttle walk time in individuals with a hypoxic COPD phenotype.
Why read on?
As COPD becomes more severe, hypoxaemia may develop which impacts on the ability to perform day-to-day activities.
Interventions which improve endothelial function, as demonstrated here, and increase the efficiency of oxygen use may help to address this.
Introduction
People with COPD may develop hypoxaemia as the condition becomes more severe, impacting on their ability to perform day-to-day activities. Mechanisms include ventilation perfusion mismatch, reduced cardiac output due to hyperinflation and pulmonary vascular limitation, as well as reduced muscle efficiency.1–5 In individuals who are sufficiently hypoxaemic, long-term oxygen therapy (LTOT) improves survival, and in many individuals ambulatory oxygen therapy (AOT) improves exercise performance.6
Nitric oxide (NO) has potential as a modulator of exercise performance. A ubiquitous signalling molecule, NO is involved in a number of processes at a tissue and cellular level, including mitochondrial and cellular respiration,7 8 glucose uptake into the skeletal muscle,9 skeletal muscle contraction,10 11 neurotransmission12 and fatigue development.13 NO is produced both by oxygen-dependent NO synthases catalysing its production from L-arginine and an alternative nitrate (NO3 −)–nitrite (NO2 −)–NO pathway.14 The latter can be influenced by supplementation with exogenous dietary NO3 − and is enhanced in conditions of hypoxia and low pH as found in exercising skeletal muscle.15
Dietary NO3 − supplementation has been shown to reduce the oxygen cost of exercise in healthy individuals in normoxic conditions16 17 and in conditions of hypoxaemia.18–23 Recently our research group has shown that it augments improvement in exercise capacity seen in people with COPD following pulmonary rehabilitation.24 25 We have also previously shown that dietary NO3 − supplementation reduces the oxygen cost of exercise during endurance cycle ergometry in COPD.26 However, that study, which excluded patients who required supplemental oxygen, did not demonstrate an improvement in exercise capacity.
The aim of the present study was therefore to assess the acute effect of dietary supplementation in the form of nitrate-rich beetroot juice (NR-BRJ) on exercise performance in individuals with COPD who require supplemental oxygen on exertion, hypothesising that this would increase exercise capacity, measured as endurance shuttle walk time (ESWT), as well as improve endothelial function in people with this specific phenotype.
Materials and methods
Study design
The EDEN-OX (Effect of Dietary Nitrate Supplementation on Exercise Performance in Hypoxia) study was a single-centre, double-blind, placebo-controlled, randomised cross-over trial comparing the effects of dietary NO3 − supplementation with a matched placebo in individuals with COPD who require LTOT and use AOT during exercise. All participants provided informed consent. The study was registered prospectively in a publicly accessible database. The data presented here relate only to the planned COPD cohort in that study.
People with Global Initiative for Chronic Obstructive Lung Disease grade II–IV COPD27 who were established users of LTOT, in accordance with the NICE guidelines,28 were recruited from the outpatient clinical services of Royal Brompton and Harefield NHS Foundation Trust (North West London) between 4 November 2016 and 8 August 2017, with the last participant’s final visit completed on 15 January 2018.
Exclusion criteria for the study included clinical instability (ie, less than 1 month after an exacerbation), significant comorbidity limiting exercise tolerance, significant renal impairment (estimated glomerular filtration rate <50 mL/min), hypotension (systolic blood pressure <100 mm Hg), pregnancy, use of NO3 −-based medicine or phosphodiesterase V inhibitors, or presence of other conditions that might be influenced by NO3 − supplementation (ie, ischaemic heart disease or peripheral vascular disease). These conditions were assessed at the screening visit through review of clinical history and assessment of relevant clinical data.
Methods
Interventions
The intervention was a commercially available concentrated NO3 −-rich BRJ (NR-BRJ) (98%) drink cut with organic lemon juice (2%) containing 0.8 g, 12.9 mmol NO3 − (140 mL Beet-It Sport Shot, James White Drinks, Ipswich, UK). The placebo beetroot juice (PL-BRJ), produced by James White, was 140 mL of the same beverage in which NO3 − was removed by a standardised method of passing the juice, prior to pasteurisation, through an ion exchange column, containing Purolite A520E, which exchanges NO3 − against chloride.29 The PL-BRJ is identical in appearance, packaging, taste and smell, and also causes beeturia (orange to red discolouration of urine).
Study conduct
At an initial baseline visit, COPD Assessment Test, Hospital Anxiety and Depression Scale, and Medical Research Council Dyspnoea Scale scores were recorded. Body composition was measured by bioelectrical impedance analysis using a Bodystat 4000 device (Bodystat, Isle of Man, UK). Participants then performed two incremental shuttle walk tests to determine the walking speed to be used for the ESWT30 and then a practice ESWT. All walking tests throughout the study were performed on the participant’s usual AOT flow rate, and the method for carrying the AOT was recorded to ensure the same method was always used (online supplemental appendix figure E1).
Supplemental material
Prior to the two subsequent intervention visits and throughout the study period, participants were asked to avoid the use of antimicrobial mouthwash and chewing gum, as these have been shown to reduce the oral facultative bacteria whose NO3 − reductase activity is essential for the metabolism of an oral NO3 − load.31 They were asked to consume the same meal on the morning of each study assessment. This was to create as standardised conditions as possible, reducing differing levels of dietary NO3 − consumption as a source of variation within individuals, while not altering their usual diet greatly. They were also asked to match caffeine consumption to standardise any ergogenic effect arising from it32 and to avoid strenuous exercise in the 24-hour period prior to the intervention visits.
The two intervention visits began at the same time of day (±2 hours), with a minimum of 7-day washout period and a maximum 1-month gap between them. Participants were randomly assigned to the order in which they received NR-BRJ or PL-BRJ using a computer-generated block randomisation list, with a block size of 10, produced by an independent statistician. The researchers responsible for enrolment and outcome measurements remained blinded throughout the study and during data analysis. Following their arrival, after a 10 min rest period, participants were observed consuming either the NR-BRJ or the PL-BRJ, and empty bottles were collected and recorded. All outcome measures were undertaken 3 hours after ingestion of either NR-BRJ or PL-BRJ.
Outcomes
Exercise capacity
The primary outcome was ESWT compared between treatment conditions. Given the cross-over design and taking 65 s (95% CI 45 to 85) to be the minimal clinically important difference(MCID) in ESWT30 and a pooled mean difference within individuals of 26 s for repeat testing, to have an 80% statistical power, with a significance level of 0.05, 16 participants would be required to reject the null hypothesis that the active intervention was not superior to placebo. To allow for a 25% withdrawal rate, a sample size of 20 was chosen.
Plasma nitrate/nitrite levels and markers of oxidative stress
Plasma NO3 − and NO2 − levels were used as a combined biomarker of NO3 − ingestion, metabolism and NO availability.33 34 Plasma samples were obtained on arrival and 3 hours after consumption of NR-BRJ or PL-BRJ (see online supplemental appendix for full details).
Oxidative stress biomarkers were assessed in plasma samples by a combination of three distinct readouts, including antioxidant potential, that is, measurement of the ferric-reducing ability of plasma (FRAP),35 lipid oxidation products by thiobarbituric acid reactive substances (TBARS)36 and total free thiols with normalisation for protein37 (see online supplemental appendix for full details).
Fractional exhaled nitric oxide
FENO was measured as a steady exhalation rate of 50 mL/s with a NIOX Mino (Aerocrine Systems, Solna, Sweden) at the screening visit and then at the intervention visits at baseline prior to NR-BRJ/PL-BRJ consumption and then at six further intervals (30, 60, 90, 120, 150 and 180 min). Both the study participant and the researchers were blinded to the results, and an independent researcher, not directly involved with the trial, uploaded the data into a password-protected database. These data were only available to the researchers following unblinding of the study.
Endothelial function
Endothelial function was assessed by flow-mediated dilatation (FMD) of the brachial artery 3 hours after NR-BRJ/PL-BRJ consumption38 using a high-resolution Doppler ultrasound to measure at baseline and sequentially over a period of 120 s after release of circulatory arrest of the upper arm.39 All measurements were performed by a single trained operator (see online supplemental appendix for full details).
Continuous oxygen saturation and heart rate analysis
For each ESWT performed, pulse oximetry values were recorded (Pulsox 300i Pulse Oximeter, Konica Minolta, Tokyo, Japan) throughout until the participant had recovered (recovery was defined by return of Borg Dyspnoea Scale to that recorded prior to the ESWT). To maintain blinding, the pulse oximeter display was covered throughout the testing and the data were downloaded by an independent researcher, not directly involved with the trial, who uploaded the data to a password-protected database. These data were only available to the researchers following unblinding of the trial.
Statistical analysis
Data are presented as mean (SD), or if not normally distributed as median and IQR. Differences in response between treatment conditions were assessed using a paired t-test or a Wilcoxon signed-rank test as appropriate. Treatment effect was estimated using the Hodges-Lehmann estimate of shift parameters. The process of determining the Hodges-Lehmann estimator entails estimating the average difference in outcomes (x-y) for every possible n(n+1)/2 pair and then deriving the overall median of all averages (the Hodges-Lehmann estimator). A distribution-free CI is estimated using large-sample approximation. Analysis was performed using SPSS V.24 for Windows and Stata V.16.1 for Windows.
To compare continuous oxygen saturations (SpO2) and heart rate (HR) between the two treatment conditions, individual ESWT data periods were subjected to a 30 s rolling average using MATLAB (MATLAB and Statistics Toolbox Release V.2017a, The MathWorks, Natick, Massachusetts, USA) and then expressed as percentages of isotime (defined as the duration of the shortest of the two ESWT). These individual responses were then grouped to allow analysis of HR and SpO2 against the percentage of isotime (plotted at the midpoint of each 10th percentile of isotime). The area under the curve (AUC) was assessed for each individual participant and the two treatment conditions compared using Wilcoxon signed-rank test. Figures were prepared using GraphPad Prism V.6.0 for Windows (GraphPad Software, San Diego, California, USA). A p value of <0.05 was considered statistically significant.
Results
We screened 67 people for eligibility (figure 1); 31 declined to participate, 7 had a comorbidity precluding participation and 9 were not using supplementary oxygen. Of the 20 participants enrolled in the study, 10 were randomised to receive PL-BRJ first and 10 NR-BRJ first. All participants completed the study. Table 1 shows their baseline characteristics, which were well matched between the two order allocation groups. There were no serious adverse effects reported, although all participants reported beeturia. The average time between each intervention visit was 7 days.
Characteristics of cross-over allocation groups: NR-BRJ or PL-BRJ received first

CONSORT diagram for recruitment and trial completion. CONSORT, Consolidated Standards of Reporting Trials; NR-BRJ, nitrate-rich beetroot juice; PL-BRJ, placebo beetroot juice.
Exercise outcomes
Exercise endurance time was longer for all study participants after NR-BRJ compared with PL-BRJ (figure 2): median (IQR) ESWT: NR-BRJ 194.6 (147.5–411.7) s vs PL-BRJ 159.1 (121.9–298.5) s, estimated treatment effect 62.5 (95% CI 33 to 106) s (p=0.000089). There was no evidence of an intervention order effect (online supplemental appendix figure E2). There was one individual who was a clear outlier for exercise endurance response. However, a sensitivity analysis removing their data led to a slight change in primary study outcome but not the overall statistical significance: median (IQR) ESWT: NR-BRJ 193.8 (145–389.6) s vs PL-BRJ 158.2 (121.6–236.6) s, estimated treatment effect 56.5 (95% CI 30 to 88) s, indicating a significant increase in ESWT with NR-BRJ (p=0.0001) (online supplemental appendix results E1).

Effect of dietary nitrate supplementation on ESWT (in seconds) for PL-BRJ and NR-BRJ dosing conditions. Data presented as individual ESWT (in seconds) in both dosing conditions. Wilcoxon signed-rank test was used to compare ESWT between the different dosing conditions: NR-BRJ 194.6 (147.5–411.7) s vs PL-BRJ 159.1 (121.9–298.5) s, estimated treatment effect 62 s (95% CI 33 to 106). ***p<0.0001. ESWT, endurance shuttle walk test; NR-BRJ, nitrate-rich beetroot juice; PL-BRJ, placebo beetroot juice.
Pulse oximetry data were available for only 18 participants because recording failed for 2 of them. The average AUC for SpO2 was higher in the NR-BRJ group compared with the PL-BRJ group. These differences were more apparent at isotime and peak exercise, with no difference at rest, during warm-up or recovery (figure 3A and online supplemental appendix table E1). The estimated treatment effect was also statistically significant: 43.69 (29.09–58.28) (p<0.0001). The AUC for HR response to NR-BRJ or PL-BRJ did not show any difference. The estimated treatment effect was also not statistically significant (−41.17 (−116.74 to 34.40), p=0.27) (figure 3B and online supplemental appendix table E1).

Effect of dietary nitrate supplementation on isotime oxygen saturation and heart rate during endurance shuttle walk test. (A) Oxygen saturation analysis in the NR-BRJ (red) and PL-BRJ (black) dosing conditions at the 10th percentile of isotime and at rest, warm-up, peak exercise and recovery. Data presented as median and IQR. The area under the curve for each treatment group was estimated and reported as mean (SD). Saturation for when the subjects were on PL-BRJ was 1161.85 (47.59) and when the subjects were on NR-BRJ was 1205.54 (46.39). The treatment effect was estimated to be 43.69 (29.09–58.28) (p<0.0001). The results suggest that on average the area under the curve for saturations was higher when on NR-BRJ than when on PL-BRJ. These differences tended to show more during the isotime and peak periods. (B) Heart rate analysis in the NR-BRJ (red) and PL-BRJ (black) dosing conditions at the 10th percentile of isotime and at rest, warm-up, peak exercise and recovery. Data presented as median and IQR. The area under the curve for each treatment group was estimated and reported as mean (SD). The mean (SD) area under the curve for the heart rate data when the subjects were on PL-BRJ was 1299.93 (186.05) and for when the subjects were on NR-BRJ was 1258.76 (174.01). The estimated treatment effect was −41.17 (−116.74 to 34.40) (p=0.27). The results show that while at individual time points the heart rate was higher for when the subjects were on PL-BRJ, there was no statistically significant difference in the area under the curve. bpm, beats per minute; NR-BRJ, nitrate-rich beetroot juice; PL-BRJ, placebo beetroot juice.
Endothelial function and blood pressure
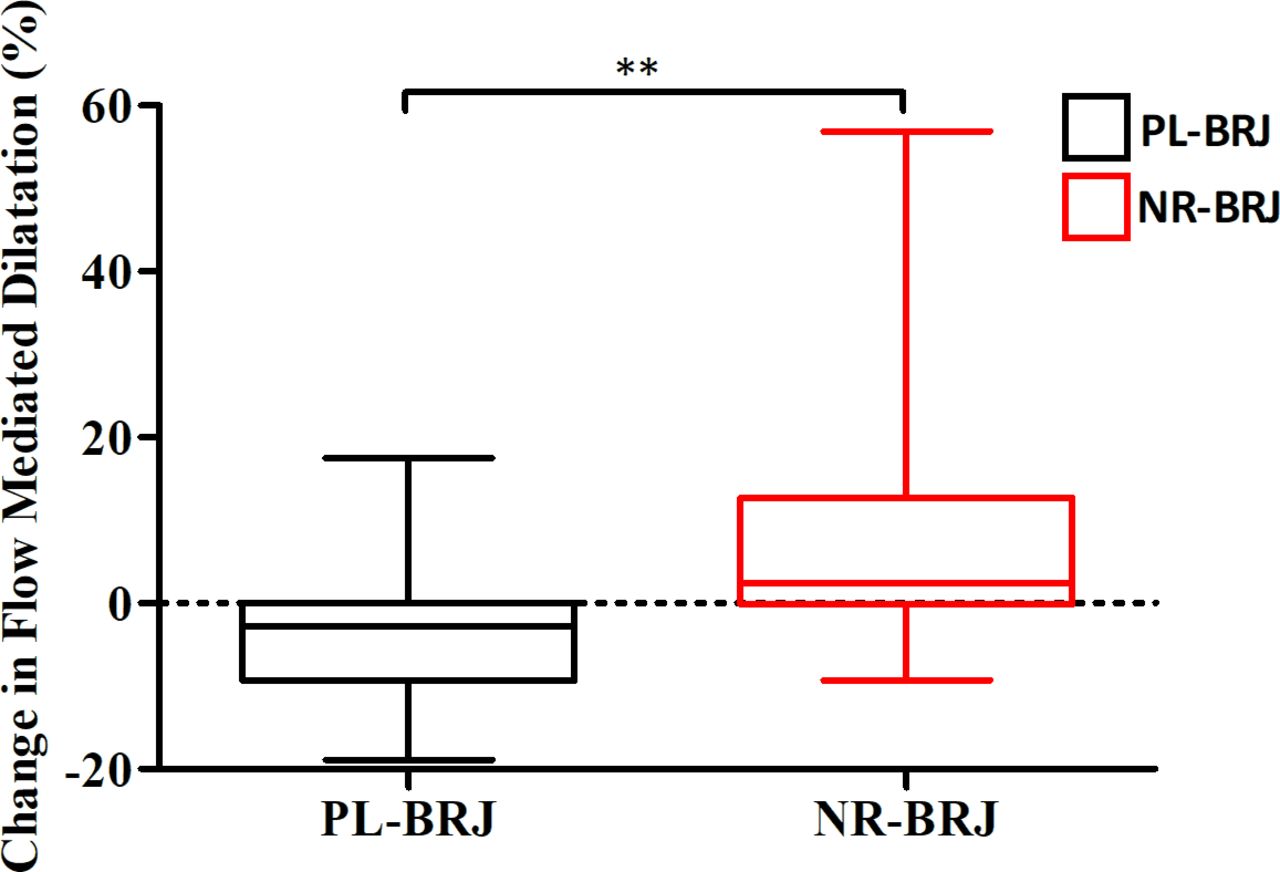
Two participants declined the FMD assessment; therefore, data were available for 18 participants. At 180 min following dosing, FMD increased: NR-BRJ 4.1% (−1.1% to 14.8%) compared with placebo −5.0% (−10.6% to −0.6%), estimated treatment effect −11.9% (95% CI −18.9 to −7.15) (p=0.0003) (figure 4).

Effect of dietary nitrate supplementation on blood pressure parameters. Change in blood pressure parameters (sBP, dBP and MAP) relative to baseline blood pressure 3 hours prior to dosing with either NR-BRJ or PL-BRJ. Data presented as 25th–75th percentile with the solid line representing the median value and the whiskers the minimum to maximum values. Wilcoxon signed-rank test was used to compare blood pressure parameters. Median (IQR) change in sBP: NR-BRJ −1.5 (15.0–10.8) mm Hg vs PL-BRJ −0.5 (−10.5 to 6.8) mm Hg (p=1.0). Median (IQR) in dBP: NR-BRJ 4.0 (−14.0 to 7.0) mm Hg vs PL-BRJ −1.0 (−9.3 to 5.0) mm Hg (p=0.481). Median (IQR) change in MAP: NR-BRJ −5.0 (−15.3 to 6) mm Hg vs PL-BRJ −2.5 (−13.5 to 7) mm Hg (p=0.359). dBP, diastolic blood pressure; MAP, mean arterial pressure; NR-BRJ, nitrate-rich beetroot juice; PL-BRJ, placebo beetroot juice; sBP, systolic blood pressure.
There was no statistically significant difference in change in blood pressure parameters from predosing levels between NR-BRJ and PL-BRJ (figure 5): median (IQR) ∆systolicBP: NR-BRJ −1.5 (15.0–10.8) mm Hg vs PL-BRJ −0.5 (−10.5 to 6.8) mm Hg, estimated treatment effect 1 mm Hg (95% CI −5.5 to 7.0) (p=1.0); ∆diastolicBP: NR-BRJ −4.0 (−14.0 to 7.0) mm Hg vs PL-BRJ −1.0 (−9.3 to 5.0) mm Hg, estimated treatment effect 1 mm Hg (95% CI −3 to 5) (p=0.481); mean arterial pressure: NR-BRJ −5.0 (−15.3 to 6.0) mm Hg vs PL-BRJ −2.5 (−13.5 to 7) mm Hg, estimated treatment effect 1.5 mm Hg (95% CI −3.5 to 5) (p=0.359).
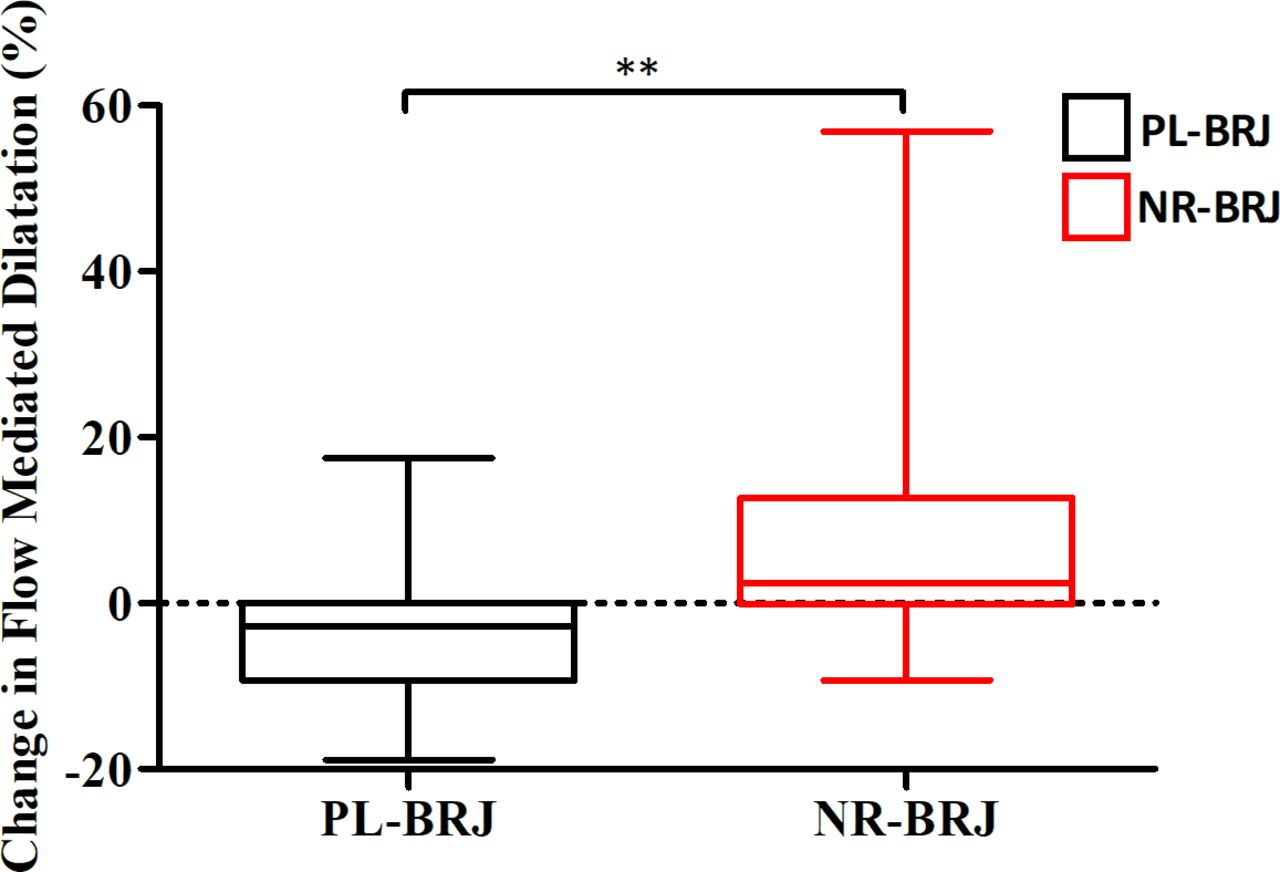
Effect of dietary nitrate supplementation on endothelial function. Percentage change in FMD from baseline and 180 min after supplementation with NR-BRJ or PL-BRJ. Data presented at the 25th and 75th percentile boxes with the solid line representing the median value and the whiskers the minimum and maximum values. Wilcoxon signed-rank test was used to compare the percentage change in FMD in the NR-BRJ (red) and PL-BRJ (black) dosing conditions. There was a statistically significant difference in the FMD percentage change with an increase in the NR-BRJ group (4.1, −1.1 to 14.8) versus a reduction in the PL-BRJ group (−5.0, −10.6 to −0.6). **p=0.0003. FMD, flow-mediated dilatation; NR-BRJ, nitrate-rich beetroot juice; PL-BRJ, placebo beetroot juice.
Plasma nitrate and nitrite levels and oxidative stress markers
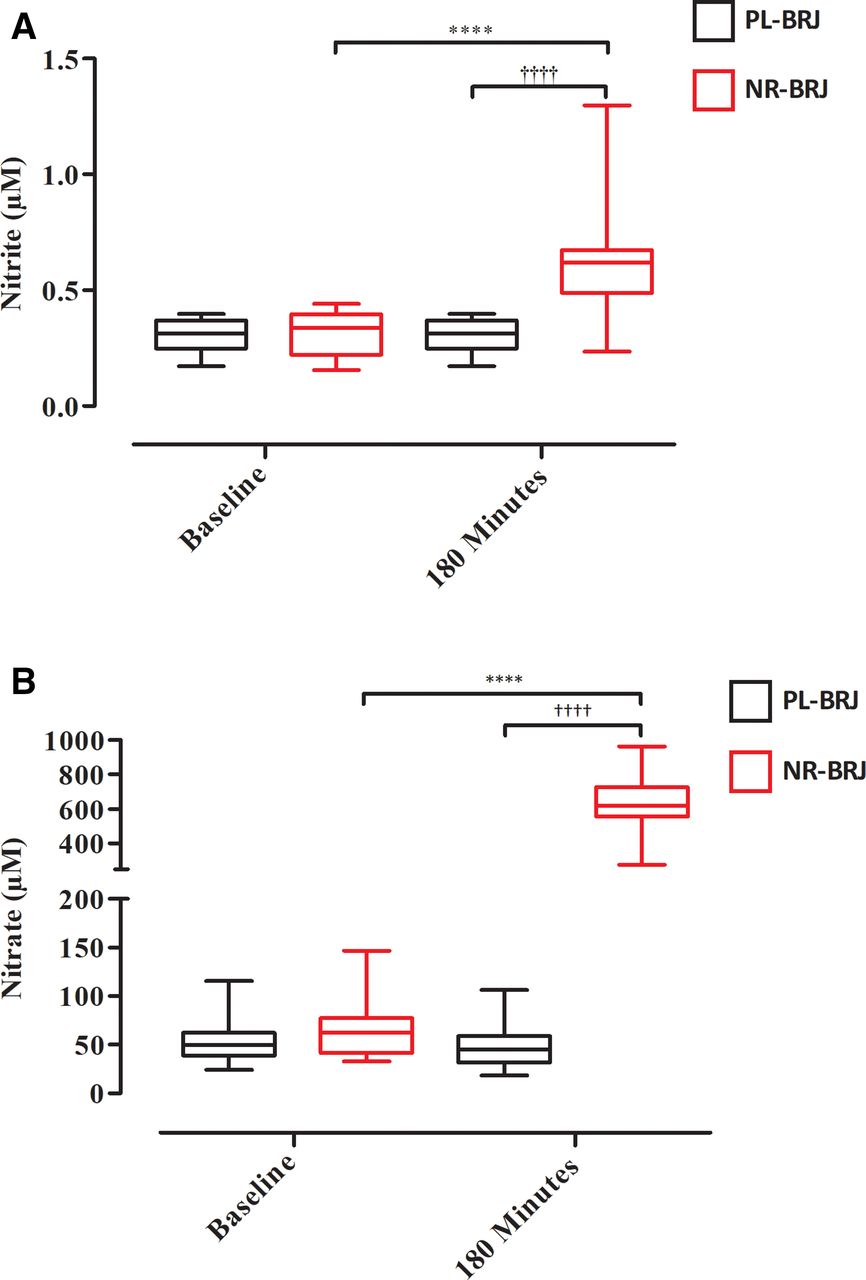
Paired data on plasma NO2 − and NO3 − concentrations were available for 19 participants, as 1 individual declined sampling. Following supplementation with NR-BRJ, there was an 84% increase in plasma NO2 − and an 887% increase in plasma NO3 − at 180 min post supplementation, but no change with placebo (figure 6 and online supplemental appendix table E2). Both the NR-BRJ and PL-BRJ supplements were analysed for NO2 − and NO3 − content as well (online supplemental appendix table E3). The change in plasma NO3 − and NO2 − from baseline to 180 s was calculated and used to estimate the treatment effect of NR-BRJ. The treatment effect of NO3 − was 550 (461–639) µM. The results suggest that this was higher for NR-BRJ than for PL-BRJ and this change was statistically significant (p=0.0003). The treatment effect of NO2 − was 0.248 (0.138–0.408) µM. The results suggest that this was higher for NR-BRJ than for PL-BRJ and this change was statistically significant (p=0.0011).

Plasma nitrite and nitrate levels. Data presented are median (IQR) with whiskers representing minimum to maximum values. Plasma NO2 − and NO3 − concentrations were measured at baseline (0 min) and 180 min after dosing with the interventions. Wilcoxon signed-rank test was used to compare change in plasma NO2 − and NO3 − concentrations between the intervention groups. Mann-Whitney U test was used to compare change in plasma NO2 − and NO3 − concentrations between the treatment conditions. (A) Changes in plasma NO2 − concentrations. There was a statistically significant difference between baseline plasma NO2 − concentration and postdosing with NR-BRJ for plasma NO2 −: predosing plasma NO2 − concentration 0.306 (0.227–0.402) µM vs postdosing 0.620 (0.488–0.673) µM; ****p=0.000076. There was also a statistically significant difference between postdosing plasma NO2 − concentration between NR-BRJ and PL-BRJ dosing conditions: postdose of NR-BRJ NO2 − concentration 0.620 (0.488–0.673) µM vs postdose of PL-BRJ NO2 − concentration 0.306 (0.227–0.402) µM; †††† p=0.000009. (B) Changes in plasma NO3 − levels. There was a statistically significant difference between baseline plasma NO3 − concentration and postdosing with NR-BRJ for plasma NO3 −: predosing plasma NO3 − concentration 62.59 (41.68–77.29) μM vs postdosing 617 (556.25–725.88) μM; ****p=0.00004. There was also a statistically significant difference between postdosing plasma NO3 − concentration between NR-BRJ and PL-BRJ dosing conditions: postdose NR-BRJ NO3 − plasma concentration 617.71 (556.25–725.88) μM vs PL-BRJ plasma NO3 − concentration 45.31 (31.39–58.84) μM; †††† p=5.66×10−11). NO2 −, nitrite; NO3 −, nitrate; NR-BRJ, nitrate-rich beetroot juice; PL-BRJ, placebo beetroot juice.
There was no statistically significant difference in measures of oxidative stress following acute consumption of either supplement: FRAP: NR-BRJ 1018 (853.0–1125) µM vs PL-BRJ 930.2 (836.8–1073) µM (p=1.0); TBARS: NR-BRJ 1.499 (0.855–3.209) mM vs PL-BRJ 0.971 (0.766–1.614) mM (p=0.4); total free thiol per protein: NR-BRJ 7.079 (5.961–8.115) µmol/g protein vs PL-BRJ 6.942 (5.768–8.026) µmol/g protein (p=0.5) (online supplemental appendix figure E3).
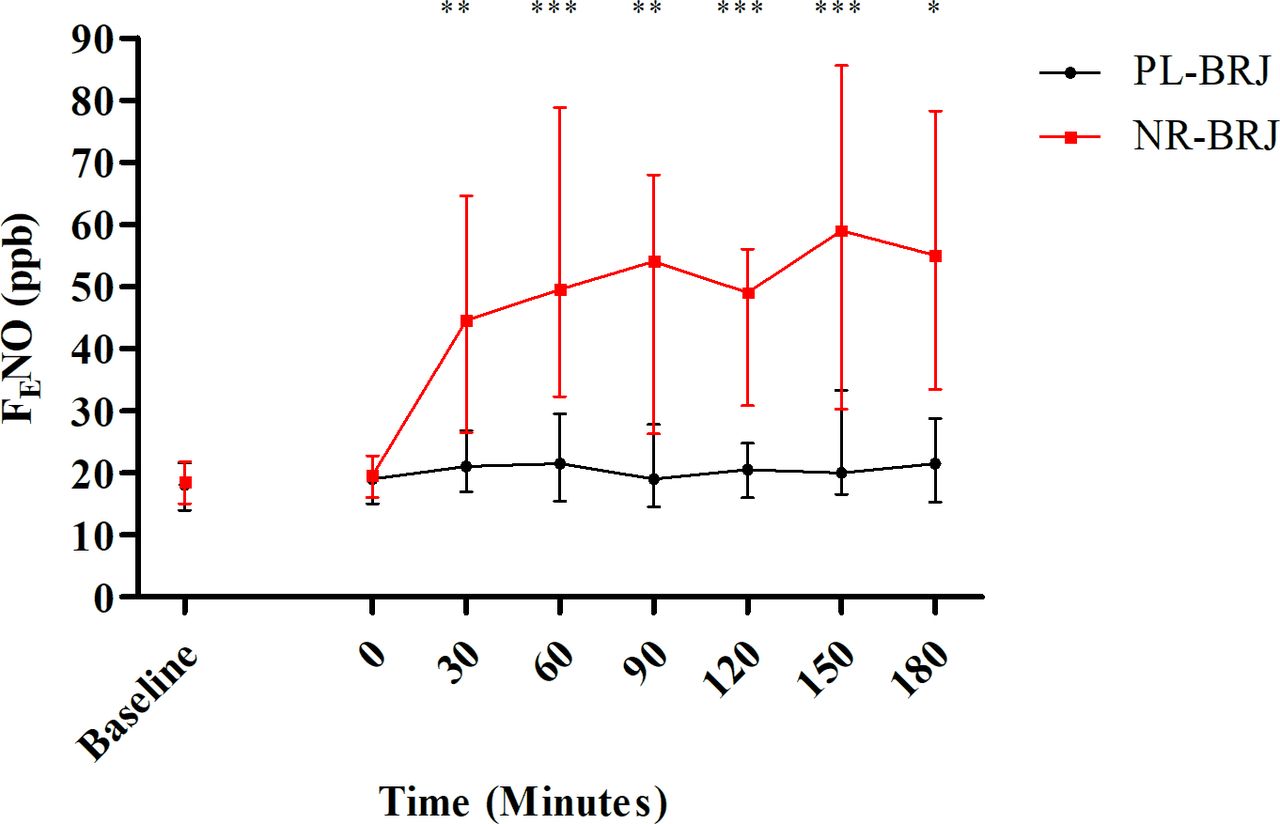
Paired measures of FENO were available for 16 participants at all seven time points (figure 7 and online supplemental appendix table E4). For four participants, there was device failure resulting in no data being recorded. The median (IQR) AUC for when the subjects were on PL-BRJ was 3622.5 (3181.9–4796.9) and the corresponding result for when the subjects were on NR-BRJ was 9440.6 (6273.8–11 831.3), and the treatment effect with its 95% CI was 5407 (3096 to 7576) (p=0.0011). The results suggest that the FENO levels while the subjects were on NR-BRJ were significantly higher than when they were on PL-BRJ. Postacute (0 min) supplementation with NR-BRJ FENO increased by 184% at 180 min post supplementation.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Exhaled nitric oxide. Data presented are median (dot) with whiskers representing IQR and with red dot and line representing NR-BRJ and black dot and line representing PL-BRJ. FENO was measured at baseline (study visit 1) and subsequently at intervention visits at seven time points (0, 30, 60, 90, 120, 150 and 180 min) dosing with either NR-BRJ or PL-BRJ. Kruskal-Wallis H test was used to assess the effect of either NR-BRJ or PL-BRJ on FENO. In both intervention groups there was no statistical difference between FENO at baseline (measured at study visit 1) and time point 0 min (measured at intervention visits prior to supplementation with intervention beverage). There was a statistically significant difference between measured FENO at all subsequent time points postintervention consumption. 30 min p=0.0011, 60 min p=0.0001, 90 min p=0.0006, 120 min p=0.0002, 150 min p=0.0002, 180 min *p=0.0024; **p≤0.01, ***p≤0.001 (see online supplemental appendix Table E4). NR-BRJ, nitrate-rich beetroot juice; PL-BRJ, placebo beetroot juice; ppb, parts per billion.
Discussion
The major finding of this study was that, in people with COPD who are hypoxic to the extent that they meet the criteria for LTOT, dietary NO3 − supplementation improves exercise capacity compared with placebo. The improvement in ESWT that we observed was accompanied by less desaturation during exercise. Supplementation also improved endothelial function assessed using FMD. In line with previous observations,24 25 blood pressure was numerically lower as well but the difference in response was not statistically significant.
Significance of findings
Although studies have previously considered dietary NO3 − supplementation in COPD with inconsistent results,24–26 40 this is the first stratified medicine approach focusing on the specific phenotype of individuals with COPD with hypoxaemia requiring LTOT. Our previous study, in non-hypoxaemic patients with COPD, found that there was a reduction in the oxygen cost of exercise during cycle ergometry yet no improvement in exercise capacity.26 In conditions of hypoxia, the L-arginine–nitric oxide synthasese pathway is compromised, while the NO3 −–NO2 −–NO pathway is facilitated due to a lesser inhibition of NO2 − bioactivation by oxygen.14 20 22 As such, dietary NO3 − supplementation could be expected to have more impact in hypoxic rather than normoxic individuals, both through effects on the skeletal muscle and impacts on the pulmonary vasculature.
The mechanism by which ESWT lengthened is likely to involve multiple synergistic pathways. The finding of relatively preserved SpO2 during exercise in the NO3 −-supplemented condition could reflect more efficient oxygen utilisation peripherally, a beneficial impact on central haemodynamics associated with/related to reduced hypoxia-induced pulmonary vasoconstriction, or a combination of the two. Despite each participant using their prescribed oxygen for each walk test, there was an observed desaturation in the placebo arm. This could mean that their oxygen prescription may have been insufficient and that a higher flow rate might also have increased exercise capacity. This finding of the attenuation of desaturation by NR-BRJ may well be explained by the enhancement of the NO3 −–NO2 −–NO pathway in conditions of hypoxia.
The observation that NO3 − supplementation was associated with improvements in endothelial function assessed using FMD is likely to be relevant to the acute mechanism of benefit from NO3 − supplementation, but also raises the possibility that longer-term dosing might reduce the risk of vascular events which are common in COPD. The effects seen are almost certainly not COPD-specific and work is needed to investigate possible benefits in other long-term lung conditions associated with hypoxia, including interstitial lung diseases and the various categories of pulmonary hypertension.
The estimated treatment effect of dietary NO3 − supplementation on ESWT found in this study was 62.5 s, which falls fractionally short of the MCID defined in pharmacotherapy trials as 65 s.30 However, in pharmacological trials where the ESWT is the outcome, interventions are typically administered over weeks or months. The demonstration of an effect of similar magnitude in a single-dose study is therefore encouraging, although further studies of longer-term use will be needed before any clinical recommendations can be made.
Study limitations
The use of a robust placebo strengthens the reliability of the findings, as does the fact that the improvement in walking time was accompanied by an appropriate physiological response (lower HR and higher SpO2). An additional strength was the use of a walking rather than a cycling test, which is of clinical relevance to patients as it reflects most individuals’ main form of exercise and daily physical activity. This was a single-dose study and therefore questions remain as to the impact that regular dosing might have and whether this would translate into meaningful clinical effects. The dose used was selected based on previous studies, but future work should investigate whether there is a dose response or ceiling effect. We have also shown that the NR-BRJ does indeed contain a higher quantity of NO3 − and provide independent confirmation that NO3 − is only present at very low levels in the placebo juice used in our study.
Conclusion
BRJ is cheap and readily accessible and has the potential to be used widely as a dietary supplement if effective in specific patient groups. Its beneficial effects appear to be mediated by inorganic NO3 − without affecting plasma redox status, on acute administration. Further mechanistic work is needed to work out the relative impact of the possible mechanisms, in particular the impact of muscle versus pulmonary or cardiac/systemic circulation effects, and longer-term studies will be needed to establish if the effects on exercise performance and endothelial function observed here translate into clinically meaningful benefits.
Data availability statement
Data are available upon reasonable request. Individual participant data that underlie the results in the article after de-identification (text, tables, figures and appendices) will be made available from the corresponding author upon request. The study protocol and statistical analysis plan will also be available. Data will be available indefinitely.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the London - Chelsea Research and Ethics Committee (ref: 15/LO/0975) and conducted in line with the principles of the Declaration of Helsinki.
Acknowledgments
The authors would like to thank all the participants who took part in this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @DrMattPav, @apl104, @COPDdoc
Contributors NSH and MIP developed the original idea for the research study. NSH and MJP designed and wrote the study protocol. WASB designed the statistical analysis plan. MJP, AL and SCB undertook patient visits and collected trial data. MF, BOF and MM-L undertook plasma analysis. MJP analysed the data and wrote the first draft of the manuscript. All authors edited and contributed to the final manuscript. NSH is the guarantor.
Funding The study was funded by a grant from Moulton Charitable Foundation.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.